
Abstract
This prospective observational study evaluates the role of tympanoplasty type III in cholesteatoma ear disease during same sitting with mastoid surgery using cartilage ossiculoplasty. Forty patients of chronic suppurative otitis media-cholesteatoma disease were recruited in the study. All the patients had extensive cholesteatoma and underwent canal wall down mastoid surgery. Tympanoplasty type III, that is, stapes columella, minor columella, or major columella, was done in each case along with mastoid surgery depending upon the remnant ossicular status. Conchal cartilage graft was used for ossiculoplasty along with temporalis fascia graft. Hearing and graft uptake results were evaluated at the end of 6 months postoperatively. Of the 40 cases, 3 cases failed tympanoplasty. In the remaining 37 cases, a statistically significant hearing improvement (air–bone gap of 33 dB) was observed postoperatively. Seven cases underwent stapes columella, 13 cases underwent minor columella, and 17 cases underwent major columella tympanoplasty type III. Although a hearing improvement was recorded in all these subgroups, a statistically significant hearing gain was present only in tympanoplasty type III minor columella cases thereby underlying the importance of intact stapes. However, it is difficult to discern the type of tympanoplasty type III that the patient would undergo prior to the ear surgery
Introduction
The principle aim of mastoid surgery in management of cholesteatoma ear disease is eradication of the disease. Secondary aims include reconstructive surgery to get a dry ear and a suitable sound transfer mechanism. 1 Clearly, restoration of hearing is now regarded as an important and intrinsic part of mastoid surgery. However, the concept of hearing improvement in cholesteatoma is a contentious issue. All aspects of this surgery, such as type of tympanoplasty, timing of surgery, and nature of material to be used for ossiculoplasty, are debatable. It has been argued that tympanoplasty should be a second-stage operation in cholesteatoma ear surgery after evaluating the success of initial mastoid surgery. However, there has been improvement in mastoid surgery over a period of time with sophisticated microscopic and endoscopic aids. Hence, one-stage mastoid surgery with tympanoplasty is being performed worldwide with good results. 2 -4
However, it would be important to note that there is limited role of ossiculoplasty in cholesteatoma ear disease. Cholesteatoma is an erosive disease, most of the times there is destruction of ossicles especially incus and stapes suprastructure. At times, there is even partial necrosis of handle of malleus. Further, in the subcontinent, most of the patients due to lack of good and efficient primary health-care facilities for detection of early cholesteatoma retraction pocket present with extensive cholesteatoma disease at the tertiary care centers. In addition, in order to remove cholesteatoma from the middle ear cavity, incus and malleus head are routinely removed. Thus, in most of the cases, a type III tympanoplasty is only possible. This reestablishes the sound continuity between the grafted tympanic membrane at the ossicular remnant, but its hearing results are unpredictable. Varying results have been reported in the medical literature for type III tympanoplasty: postoperative air–bone gap (ABG) of anywhere between 10 and 60 dB. 5 -8
We performed an in-depth analysis of the sparse literature on the subject of hearing reconstruction in cholesteatoma. 4,5,9 -12 These studies have variable parameters. Most of these studies are retrospective analyses, which include both canal wall up and down surgeries and have used many types of prosthesis such as cartilage, autologous remnant ossicles, and biomaterials. Hence, it becomes difficult to reach a definitive conclusion on the best technique and prosthesis for cholesteatoma surgery. There is a prospective study by Quaranta et al on the cited subject with costal cartilage, but it too includes many variable parameters: both canal wall up and down surgery, second-stage tympanoplasty, and recurrent cholesteatoma surgery. 13 In a massive Internet search using PubMed/MEDLINE services, authors could find no study examining the role of cartilage ossiculoplasty in cholesteatoma ear surgery as defined here in. With this background, we present our hearing results of type III tympanoplasty in cholesteatoma ear surgery done in the same sitting using conchal cartilage, in a prospective study design.
Materials and Methods
A prospective study was conducted in the department of ear, nose and throat (ENT) of our tertiary care teaching hospital. The cohort comprised of 40 consecutive cases of cholesteatoma ear disease in the specified time period: September 2015 to April 2017. This study was approved by the medical division of the university board of studies. An informed consent was mandatory. Previously operated patients of ear surgery were excluded from the study design. There were 24 males and 16 females in the age-group of 7 to 42 years. All the patients underwent a detailed clinical evaluation, computed tomography (CT) scan, and pure tone audiometry (PTA).
After requisite investigations and anesthetic clearance, patients underwent mastoid surgery under general anesthesia operated by a single surgeon, the principal investigator—first author. Due to the extensive nature of the cholesteatoma, all the patients underwent canal wall down mastoid surgery. A type III tympanoplasty was done in all the cases in the same sitting, using temporalis fascia graft and conchal cartilage. Depending upon the remnant ossicular status in each case, following variations in tympanoplasty type III were done: Type III tympanoplasty stapes columella (myringostapediopexy): Temporalis fascia graft was placed directly on stapes, Type III tympanoplasty minor columella (tympano-cartilago-stapediopexy): A conchal graft was interposed between intact stapes and temporalis fascia graft, and Type III tympanoplasty major columella: Stapes suprastructure was absent and the conchal cartilage was put in the stapes footplate supporting the temporalis fascia graft.
Subsequently, stitch and pack removal was done on 10th postoperative day. Patients were kept on a regular monthly follow-up in ENT out-patient department, and mastoid cavity was duly examined for a period of 6 months. A final evaluation with PTA was done at the end of the sixth month. An intact graft at the end of 6 months with dry mastoid cavity was considered a surgical success. Hearing results were recorded in accordance with the guidelines of the Committee of hearing and equilibrium of the American Academy of Otolaryngology Head and Neck Surgery. 14 The postoperative ABG and the number of decibels of ABG closure were assessed for 6 months.
All the above data were tabulated and statistically analyzed using Wilcoxon-signed rank test and Student t test. SPSS version 20 was used for the statistical analysis. As there were small sample sizes in each subgroup of tympanoplasty type III, the validation of the data was done by 2 statistical tests.
Results
In this study, 3 cases had failed tympanoplasty at the end of 6 months and these were excluded from the study. The results in the remaining 37 cases are presented here. The authors would also like to point out that no case was lost in follow-up. An overall ABG of 33 dB was seen at the end of 6 months as compared to a preoperative ABG of 36 dB. This was found to be statistically significant (Table 1). Of these 37 cases, 7 and 17 cases underwent myringostapediopexy and major columella tympanoplasty, respectively. In the remaining 13 cases, minor columella tympanoplasty was done. The detailed hearing evaluation in the subgroups with statistical analyses is presented in Table 2.
Overall Hearing Evaluation in Tympanoplasty Type III (37 Cases).
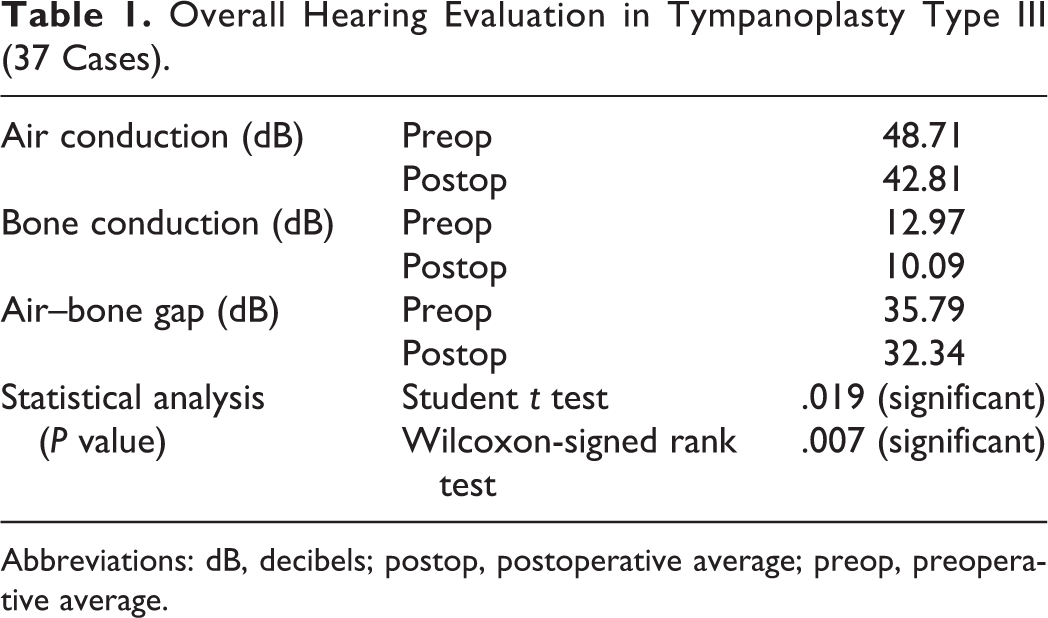
Abbreviations: dB, decibels; postop, postoperative average; preop, preoperative average.
Hearing Evaluation: Subtype of Tympanoplasty Type III.
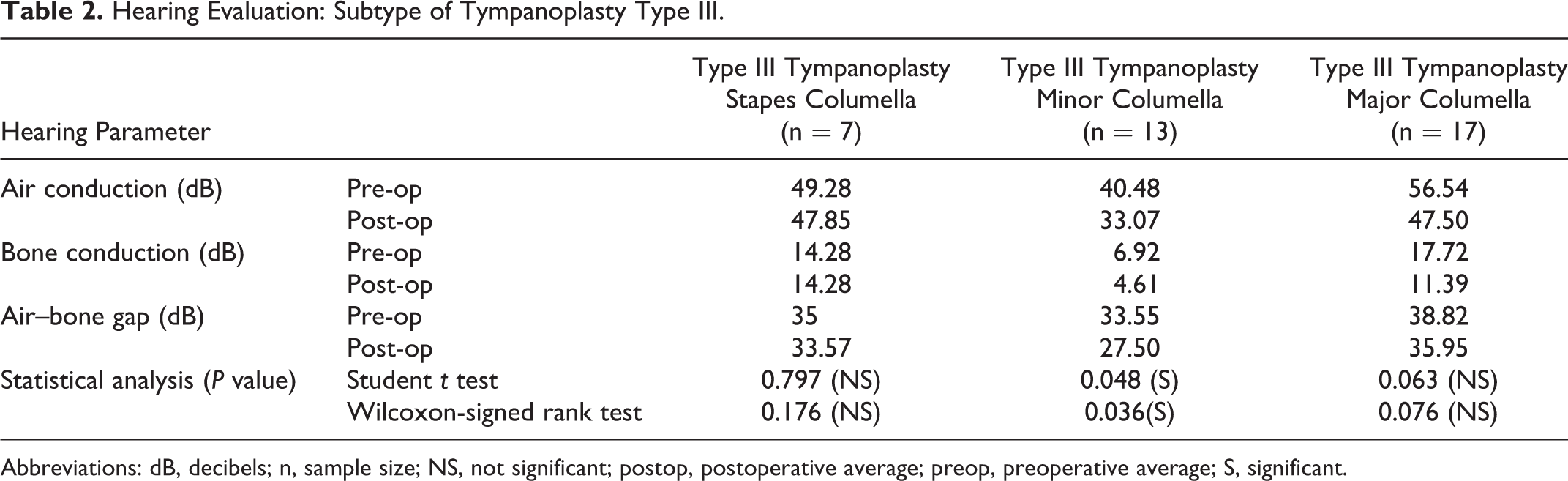
Abbreviations: dB, decibels; n, sample size; NS, not significant; postop, postoperative average; preop, preoperative average; S, significant.
From Table 2, it is clearly evident that the preoperative ABG in myringostapediopexy patients was 35 dB, which was reduced to 33.57 dB postoperatively. However, this was not found to be statistically significant. Similarly, for major columella type III tympanoplasty, no statistically significant improvement in hearing was observed, although the ABG declined to 35.95 dB after surgery from 38.82 dB.
However, for minor columella tympanoplasty type III, a significant hearing gain was observed. The postoperative ABG was reduced to 27.5 dB from 33.55 dB.
In the context of above results, the authors would like to emphasize that no complication of mastoid surgery was recorded in this case series.
Discussion
At the outset, authors would like to point out that this study evaluates short-term hearing gain after cholesteatoma ear surgery. The short-term results are an accurate reflection of the actual reconstruction. Long-term success of ossiculoplasty is influenced by factors which are beyond the control of surgeon, such as patient follow-up, Eustachian tube function, and middle ear environment. We had an overall significant improvement in hearing using tympanoplasty type III in cholesteatoma surgery. Our results of postoperative ABG of 33 dB augurs well with the varied result of 10 to 60 dB reported in the medical literature for tympanoplasty type III. 5 -8 We now present the hearing analyses in each subtype of tympanoplasty type III.
Hearing Gain in Type III Stapes Columella (Myringostapediopexy)
Seven of our cases underwent myringostapediopexy (type III, stapes columella) where the graft was directly placed on the stapes. We recorded a postoperative ABG of 33.57 as compared to a preoperative gap of 35. The statistical evaluation of these data revealed no significant hearing gain (Table 2). Our results confirm the postoperative ABG of 10 to 60 dB reported in the world medical literature for type III tympanoplasty. 5 -8
Hearing Gain in Type III Tympanoplasty Minor Columella (Tympano-Cartilago-Stapediopexy)
Thirteen of our cases underwent tympano-cartilago-stapediopexy (type III, minor columella) where a conchal cartilage graft was interposed between the intact stapes and temporalis fascia graft. Our indication for doing this was when the stapes suprastructure/head failed to reach the height of the tympanic segment of facial canal in Canal wall down surgeries. 6 The height of the stapes was augmented by this cartilage piece. By this, we recorded an ABG of 27.5 dB postoperatively as compared to a preoperative value of 33.5. The statistical evaluation of the data revealed a significant hearing improvement postoperatively (Table 2). Studies across the world have also endorsed our view. Studies by Moustafa and Khalifa and Artuso et al have all shown improved hearing results after tympano-cartilago-stapediopexy. 7,8 In various other clinical studies, this modification translates to ABG of 10 to 25 dB. 15,16 A recent study by Cheang et al did myringolenticulopexy in their series of patients (graft was put on a remnant of lenticular process attached to stapes head) and also recorded an improved hearing as compared to myringostapediopexy. 5 In type III minor columella technique, middle ear space is maintained. Moreover, the placement of cartilage on stapes head prevents the collapse of the graft on the middle ear.
Hearing Gain in Type III Tympanoplasty Major Columella
Seventeen of our patients underwent type III major columella operation, that is, stapes suprastructure was absent and the conchal cartilage was put on the stapes footplate and temporalis fascia graft. This simple procedure gave us an improved postoperative ABG (preoperative ABG was 38.82 and postop ABG was 35.95), but on statistical analyses, no significant improvement in hearing was noted. There is marked paucity of literature on the audiological results of type III major columella in mastoid surgery. The text quotes a postoperative ABG of 30 to 40 dB or less for this type of tympanoplasty. 6 Recent study by Gostian et al reports a mean reduction in ABG from 32 dB to 22 dB for this kind of tympanoplasty. 17 Yet another study by Iniguez-Cuadra et al recorded an ABG <20 dB in 66% of cases. 18 However, any comparison with this study must be made with caution, as in the aforementioned studies, ossicular prosthesis was used, but not cartilage.
From our results, it is clearly evident that in the case of tympanoplasty type III, an intact stapes and the anatomical height of the facial canal with respect to stapes head, that is, the height of the facial recess, are 2 important determinants for a good hearing gain postoperatively in cholesteatoma ear surgery. Importance of an intact stapes superstructure for good hearing results in cholesteatoma surgery has also been mentioned by Chang and Chen, De Corso et al, and Uyar et al. 11,12,19 However, it would be important to note that these factors are difficult to assess preoperatively. Even the role of CT scan of temporal bone is disputed in resolution for stapes in cholesteatoma disease 20,21 In addition, the indications for type III tympanoplasty minor columella are not clearly defined in the literature. It is thus difficult to predict the hearing gain for the patient prior to surgery.
To circumvent the problem of poor follow-up in India, we did all our tympanoplasty in the same sitting with the mastoid surgery. New Delhi is a tertiary care health center and most of our cases belong to distant places and do not turn-up for second-stage surgery. It has been suggested that single-stage mastoid surgery with ossiculoplasty on the stapes may mask clinical evidence of residual cholesteatoma in oval window area. However, it would be pertinent to note that no residual cholesteatoma was seen in our operated cases at the end of 6 months. We thus recommend same-stage ossiculoplasty in all cases of mastoid surgery for cholesteatoma as it would be highly cost-effective, especially in developing countries. This algorithm of management not only eliminates repeated hospital admissions and bed occupancy but also abolishes the hidden costs to patient’s attendants of time off from work and time away from home.
In addition, we would like to emphasize that conchal cartilage was used in all our cases for ossiculoplasty. Ossicles of the patients were not used as autografts. These ossicles were necrosed and unfit for sculpting as they were engulfed in cholesteatoma. Moreover, with such ossicles, there is always a chance of seeding of cholesteatoma in the middle ear. 22 We believe that conchal cartilage has some inherent advantages. It is readily available during surgery free of cost (as compared to an ossicular prosthesis) and has a natural curve which aids in their snug fitting during surgery. Further, they do not require time for sculpting and do not extrude. Unlike ossicles, they do not fix to the promontory or facial nerve with subsequent worsening of hearing. However, histological studies have shown that they develop chondromalacia and do have a tendency to undergo resorption over a period of time, but some studies have also shown that cartilage gets calcified as a result of vascularization. 23,24
It would be important to note that Gooda and Nishara have reported that ideal tympanoplasty should have the following characteristics
25
: Prosthesis mass <40 mg, Proper tension of the prosthesis, Angle between tympanic membrane and stapes <45°, and Prosthesis with a head angulated at 30° to increase the surface area of tympanic membrane.
Interestingly, apart from head angulation at 30°, a conchal cartilage fulfills all other aforementioned criteria. The conchal cartilage prosthesis has a mass less than 40 mg and proper tension can be obtained by trimming the shaft. The angle with the stapes footplate or stapes superstructure often approximates 0° when the conchal cartilage is placed under tympanic membrane. All these factors make conchal cartilage an ideal graft for ossiculoplasty.
In summary, we have demonstrated the clinical usefulness of type III tympanoplasty in cholesteatoma ear surgery using conchal cartilage. However, there are caveats to our study. There could be selection bias in the cohort. The study was not blinded, and the results might have been influenced by the expertise of the operating surgeon (first author, an experienced otologist). Some may regard the follow-up period to be short; it would indeed be interesting to evaluate the long-term results in these cases. The study thus reports only the short-time results. Furthermore, in an observational study, confounding cannot be ruled out as a potential explanation of the observed results. It would also be pertinent to note that the results were not compared to partial ossicular replacement prosthesis/Total ossicular replacement prosthesis, which also gives excellent results in ossiculoplasty. Economic constrains in subcontinent led us to use cartilage as an effective ossiculoplasty material. Nevertheless, the strength of this study lies in its prospective nature mitigating the shortcomings of a retrospective analysis of data. Our data are unique, as independent statistical validation has been presented for select subtypes of tympanoplasty type III (stapes, minor and major columella). The true value of this study in the context of existing literature is the exclusive evaluation of type III tympanoplasty in cholesteatoma ear surgery done in the same sitting, in a prospective study design, hitherto unreported. This study amalgamates the realities of clinical practice with rigors of scientific analysis of data and thus would provide impetus for future research on the cited subject.
Conclusions
Several implications for both policy and practice related to hearing improvement in cholesteatoma ear surgery emerge from this study: Same-sitting tympanoplasty along with mastoid surgery for cholesteatoma gives satisfactory hearing results: An ABG of 33 dB can be assured to the patient postoperatively with tympanoplasty type III. The best hearing results are obtained for type III tympanoplasty minor columella subtype. Intact stapes is an important factor to get a good hearing result in cholesteatoma ear surgery. Conchal cartilage is an excellent ossiculoplasty material.
It would however be prudent to note that it is difficult to predict the type of tympanoplasty type III in a patient prior to surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.