
Abstract

A 44-year-old male with a history of chronic bronchitis and eosinophilic esophagitis presents with a 17-year history of intermittent nonpainful right parotid swelling. Notably, the mass wound regress when the patient was treated with systemic steroids for bronchitis. Examination revealed intact facial nerve function with 3 cm × 3 cm right parotid mass. Magnetic resonance imaging showed a well-circumscribed homogeneously enhancing mass with low T1 and intermediate T2 signal involving the superficial right parotid gland (Figure 1). Fine needle aspiration (FNA) showed a polymorphous population of lymphocytic cells . Given indeterminate cytology and concerning clinical and radiographic features, the patient underwent a right superficial parotidectomy.
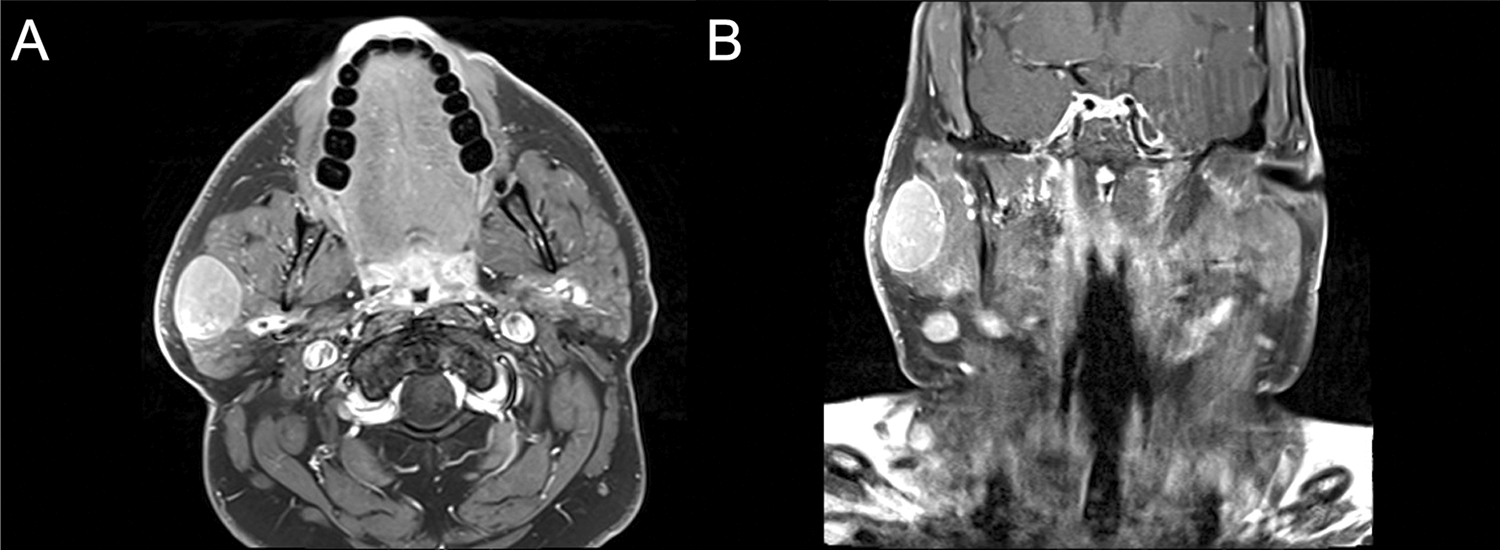
Magnetic resonance imaging (MRI) neck with contrast. (A) Axial and (B) coronal T1 MRI fat-saturated postgadolinium. Right parotid/periparotid 2.5 cm × 3.1 cm × 3.7 cm well-circumscribed homogeneously enhancing mass with low-T1 signal and right cervical chain lymphadenopathy. Adenopathy and possible extraparotid origin suggest a generalized process such as metastatic carcinoma or lymphoma.
Surgical pathology demonstrated an intraparotid lymph node with reactive follicular hyperplasia with progressive transformation of germinal centers and histologic features of immunoglobulin G4-related disease (IgG4-RD; Figure 2). Immunostaining for IgG and IgG4 demonstrated a clear IgG4:IgG ratio of greater than 40%. Laboratories revealed IgE 114 IU/mL (<100 IU/mL), IgG4 102.1 mg/dL (4-86 mg/dL), and total IgG 715 mg/dL (694-1618 mg/dL). The patient’s symptoms resolved after parotidectomy, and therefore, treatment with immunosuppression was forgone. He continues to be monitored closely.

The H&E stain of excised intraparotid lymph node. A, H&E, ×100, lymph nodes show follicular hyperplasia and fibrosis. B, H&E, ×100, shows lymphoid follicle. Inset square box shows magnified view (×200) of germinal center with increased plasma cells (white arrow). H&E indicates hematoxylin and eosin.
The parotid gland is composed of secretory units, intraparenchymal lymphoid tissue, and myoepithelial cells. Abnormalities of these components may present as a parotid mass. 1 A rare immune-mediated cause of a parotid mass is IgG4-RD. In 1995, Yoshida and colleagues described and coined the term autoimmune pancreatitis (AIP). 2 In 2003, Kamisawa described other autoimmune diseases in a large percentage of patients with AIP. Kamisawa concluded that AIP was a systemic autoimmune disease and coined it IgG4-related systemic disease. 3
The salivary glands are the second most common site of extrapancreatic organ involvement in IgG4-related AIP. Circumscribed lesions with a robust infiltrate of IgG4-positive cells and a histologic IgG4 to IgG ratio of at least 0.4 are seen. Historically, IgG4-related sialadenitis dates back to the description of Mikulicz disease in 1892 and Kuttner tumor in 1972. Today, Stone’s 2012 consensus statement helps categorize this disease. 4,5
Okazaki’s unifying hypothesis implicates autoantigens in the inhibition of regulatory T cells and the evolution of this disease. 6 Histopathology is the cornerstone for diagnosis with critical features including dense lymphoplasmacytic infiltrate, storiform fibrosis pattern, obliterative phlebitis, and eosinophilia. 7 Up to 40% of patients with IgG4-RD may have concomitant allergic disease. Treatment includes systemic glucocorticoids or steroid-sparing agents.
In this rare immune-mediated disease, it is critical to always rule out malignancy. The greatest histopathological mimickers of IgG4-RD are lymphomas. Quality and clonality of immune cell infiltrate help distinguish these entities. A thorough workup and long-term follow-up are critical even in very well-appearing patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.