
Abstract
In the head and neck region, myxomas occur rarely, and most of these lesions are odontogenic in origin and involve the facial bone. Myxoma in the larynx is extremely rare. There are about 10 cases of myxomas in the larynx cited in the English literature. Herein, we describe 3 cases of a laryngeal myxoma that presented as polypoid masses in the anterior commissure and anterior third of the vocal fold. Phonosurgery was performed with a microscope, and the masses were diagnosed as myxomas.
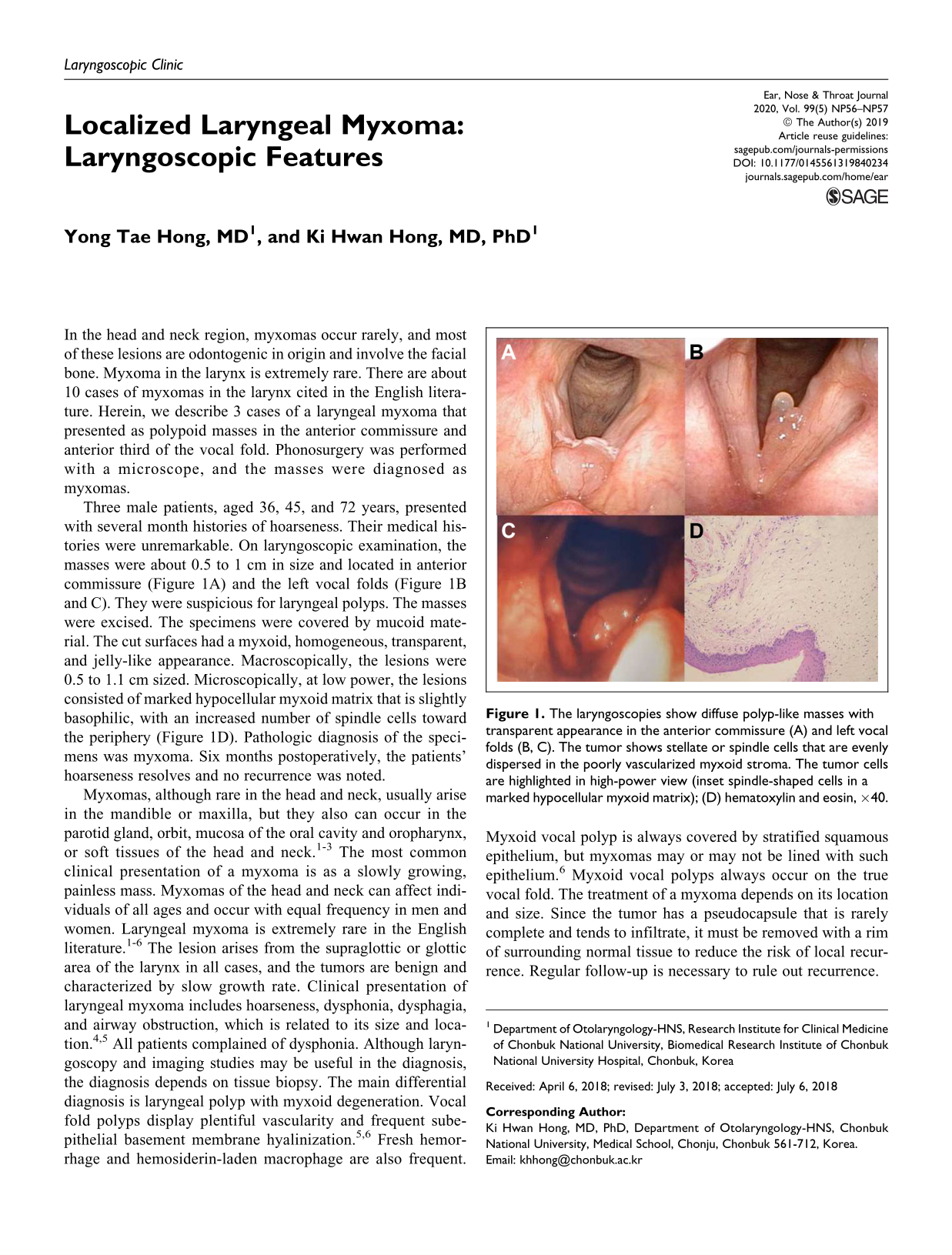
Three male patients, aged 36, 45, and 72 years, presented with several month histories of hoarseness. Their medical histories were unremarkable. On laryngoscopic examination, the masses were about 0.5 to 1 cm in size and located in anterior commissure (Figure 1A) and the left vocal folds (Figure 1B and C). They were suspicious for laryngeal polyps. The masses were excised. The specimens were covered by mucoid material. The cut surfaces had a myxoid, homogeneous, transparent, and jelly-like appearance. Macroscopically, the lesions were 0.5 to 1.1 cm sized. Microscopically, at low power, the lesions consisted of marked hypocellular myxoid matrix that is slightly basophilic, with an increased number of spindle cells toward the periphery (Figure 1D). Pathologic diagnosis of the specimens was myxoma. Six months postoperatively, the patients’ hoarseness resolves and no recurrence was noted.
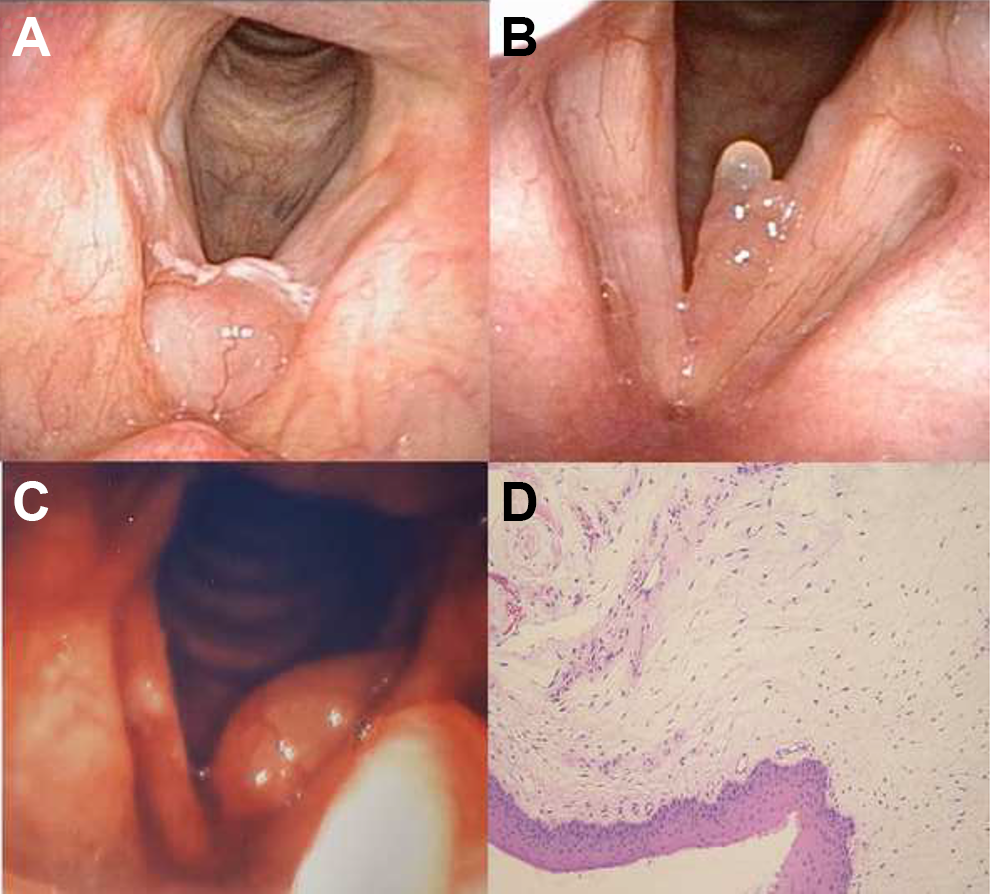
The laryngoscopies show diffuse polyp-like masses with transparent appearance in the anterior commissure (A) and left vocal folds (B, C). The tumor shows stellate or spindle cells that are evenly dispersed in the poorly vascularized myxoid stroma. The tumor cells are highlighted in high-power view (inset spindle-shaped cells in a marked hypocellular myxoid matrix); (D) hematoxylin and eosin, ×40.
Myxomas, although rare in the head and neck, usually arise in the mandible or maxilla, but they also can occur in the parotid gland, orbit, mucosa of the oral cavity and oropharynx, or soft tissues of the head and neck. 1 –3 The most common clinical presentation of a myxoma is as a slowly growing, painless mass. Myxomas of the head and neck can affect individuals of all ages and occur with equal frequency in men and women. Laryngeal myxoma is extremely rare in the English literature. 1 –6 The lesion arises from the supraglottic or glottic area of the larynx in all cases, and the tumors are benign and characterized by slow growth rate. Clinical presentation of laryngeal myxoma includes hoarseness, dysphonia, dysphagia, and airway obstruction, which is related to its size and location. 4,5 All patients complained of dysphonia. Although laryngoscopy and imaging studies may be useful in the diagnosis, the diagnosis depends on tissue biopsy. The main differential diagnosis is laryngeal polyp with myxoid degeneration. Vocal fold polyps display plentiful vascularity and frequent subepithelial basement membrane hyalinization. 5,6 Fresh hemorrhage and hemosiderin-laden macrophage are also frequent. Myxoid vocal polyp is always covered by stratified squamous epithelium, but myxomas may or may not be lined with such epithelium. 6 Myxoid vocal polyps always occur on the true vocal fold. The treatment of a myxoma depends on its location and size. Since the tumor has a pseudocapsule that is rarely complete and tends to infiltrate, it must be removed with a rim of surrounding normal tissue to reduce the risk of local recurrence. Regular follow-up is necessary to rule out recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.