
Abstract

A 79-year-old man presented with a 3-week history of odynophagia and foreign body sensation in the throat. He had smoked 20 cigarettes a day for almost 40 years, but he had stopped about 30 years ago.
Videolaryngoscopy revealed a red, pedicled lesion, <1.5 cm in diameter, on the laryngeal aspect of the epiglottis, with intact, smooth covering mucosa. Vocal fold and arytenoid mobility were preserved, and no cervical lymph nodes were palpable (Figure 1).
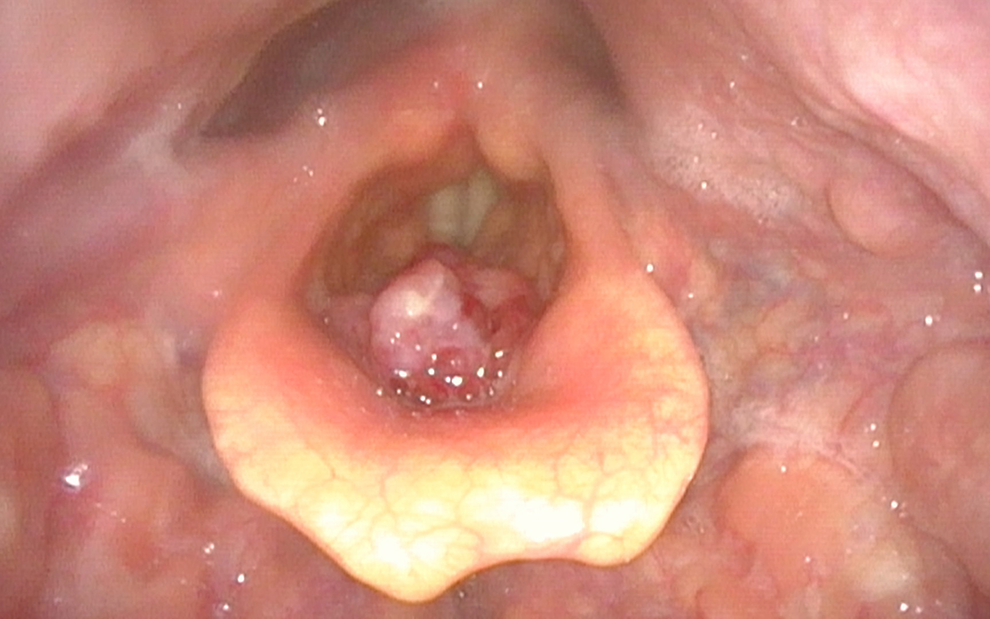
Videolaryngoscopy reveals a red, pedicled lesion on the laryngeal aspect of the epiglottis of <1.5 cm in diameter, with intact, smooth covering mucosa. Vocal fold and arytenoid motility are preserved.
Neck computed tomography (CT) scan showed a small mass, not infiltrating the laryngeal aspect of the epiglottis, without involvement of the pre-epiglottic space and superior/inferior paraglottic space (Figure 2). Positron emission tomography (PET)/CT scan confirmed the CT findings and also revealed no evidence of distant metastasis.
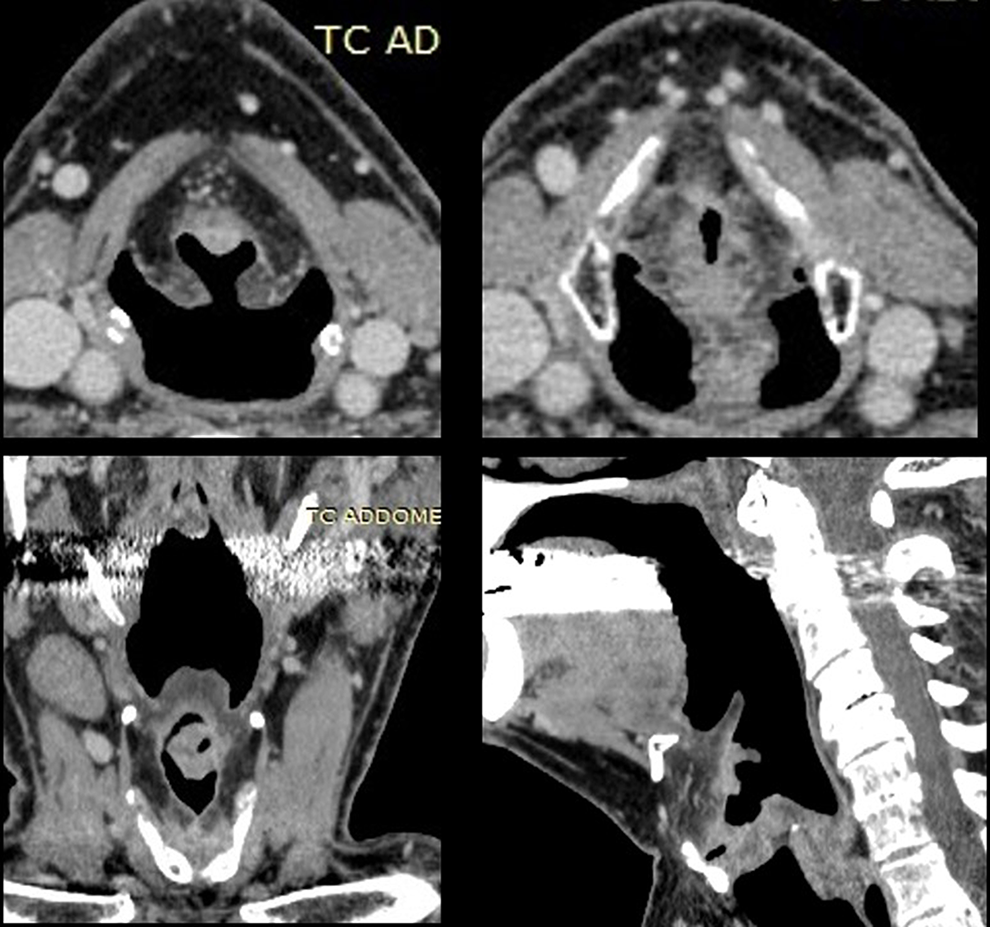
Neck computed tomography (CT) scan shows the presence of a small mass, not infiltrating the laryngeal aspect of the epiglottis, without involvement of the pre-epiglottic space and superior/inferior paraglottic space.
Direct laryngoscopy and biopsy were carried out. Microscopic examination was compatible with an atypical carcinoma of the larynx.
Laser CO2 supraglottic type II laryngectomy, bilateral selective neck dissection (IIa-III levels), and a temporary tracheotomy were performed. The postoperative period was uneventful. Definitive microscopic examination confirmed an ulcerated, atypical carcinoid tumor. Lymph node metastases were present in 3 of 10 cervical nodes on the right side, without extracapsular spread. Three-year clinical follow-up revealed no local or regional recurrence or distant metastasis. The patient underwent a Gallium 68Ga-DOTATOC PET-TC scan that showed no distant metastasis.
Laryngeal neuroendocrine carcinomas (NECs) are rare (<1% laryngeal tumors), they occur mostly in supraglottic larynx. There are 3 subcategories: typical carcinoid tumor, atypical carcinoid tumor, and small-cell NEC. Atypical carcinoma is quite aggressive and could develop metastases (survival rate at 5 years is 48%). 1 –3 It affects males, 33 to 83 years old, typically heavy smokers.
Presenting symptoms include dysphagia, odynophagia, hoarseness, earache, sore throat, and haemoptysis. Secondary systemic symptoms such as “carcinoid syndrome” are rare. The tumor is aggressive, and cervical lymph node metastases are often present. Metastases to bones, skin, subcutaneous tissues, distant lymph nodes, lung, mediastinum, and liver can occur.
Diagnosis is based on biopsy with immunohistochemical studies and electron microscopic investigation. Specific pathologic identification is important in order to determine correct treatment and prognosis.
They are not responsive to chemotherapy, and the role of radiotherapy is controversial. Surgery is the only effective therapy. Selective bilateral neck dissection (II-IV levels vs IIa-III levels) should be performed even in N0 case, considering the high likelihood of cervical lymph node metastases and of occult metastases. 4,5 The clinician should always suspect an NEC in a case of small laryngeal tumor with metastases and when investigating lymph nodes or cutaneous metastases from an unknown primary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article