
Abstract
A 54-year-old woman with a 25 pack-year smoking history and chronic obstructive pulmonary disease presented with a large right neck mass. Flexible laryngoscopy showed an enlarged right false vocal fold with unremarkable overlying mucosa. The mass changed in size with Valsalva maneuver. The patient underwent computed tomography (CT) imaging (Figure 1), which revealed a large air-filled mass of the right neck that was diagnosed as a combined laryngocele.
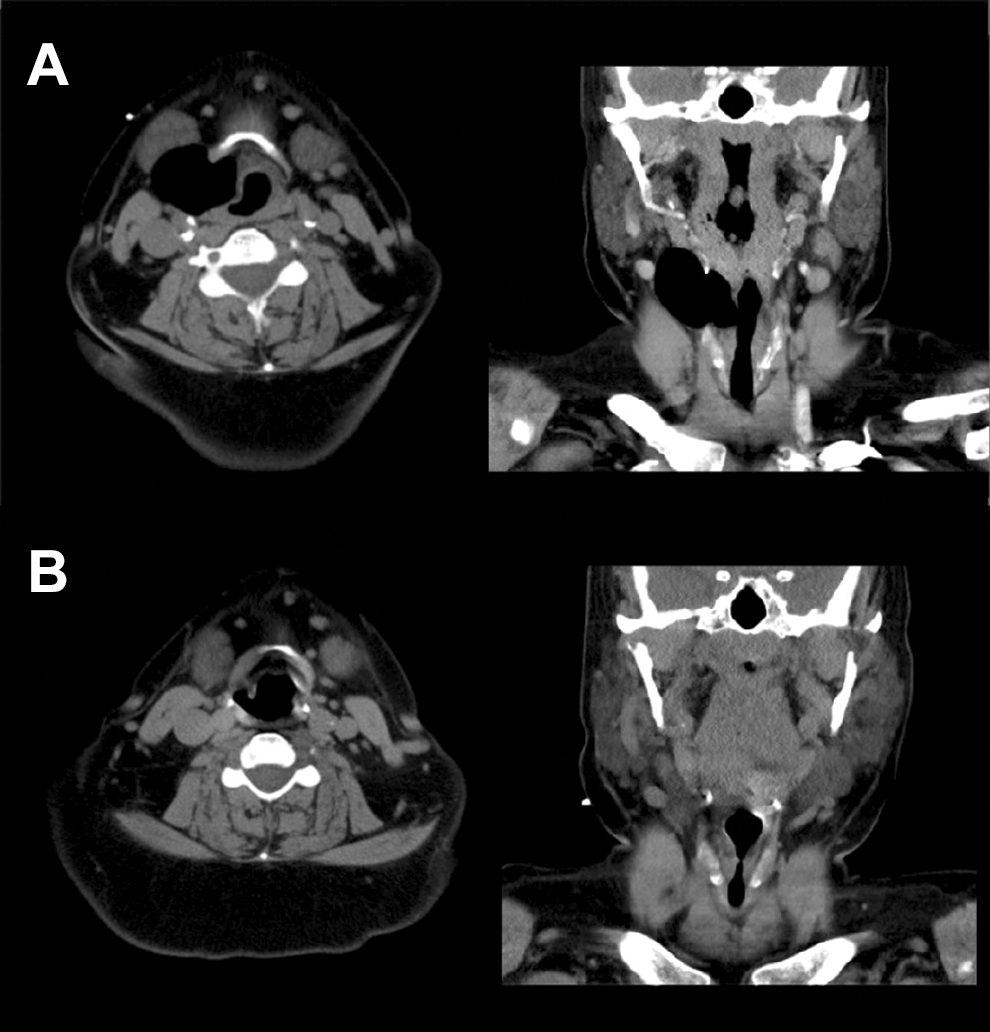
A, Preoperative axial and coronal computed tomography (CT) images demonstrating extensive right combined laryngocele and (B) postoperative images showing resolution of pathology.
The patient was consented for endoscopic excision of a right combined laryngocele with the possibility of requiring an open transcervical procedure. The patient was taken to the operating room, placed in the supine position, and intubated using a 6.0 laser-safe endotracheal tube. A Storz anterior commissure rigid laryngoscope was used to visualize the glottis, and the patient was placed in suspension. A CO2 laser on 5 W super pulse was used to make a mucosal incision over the right false vocal fold. A microlaryngeal heart-shaped forceps was used to grasp the laryngocele wall to provide traction. Using the CO2 laser and microlaryngeal spatula, the mass was dissected out of the larynx en bloc. The laser was defocused to achieve optimal hemostasis. The procedural steps are summarized in Figure 2. The specimen, measuring 6 cm in its largest dimension, was sent to pathology (Figure 3). No neoplastic tissue was identified.
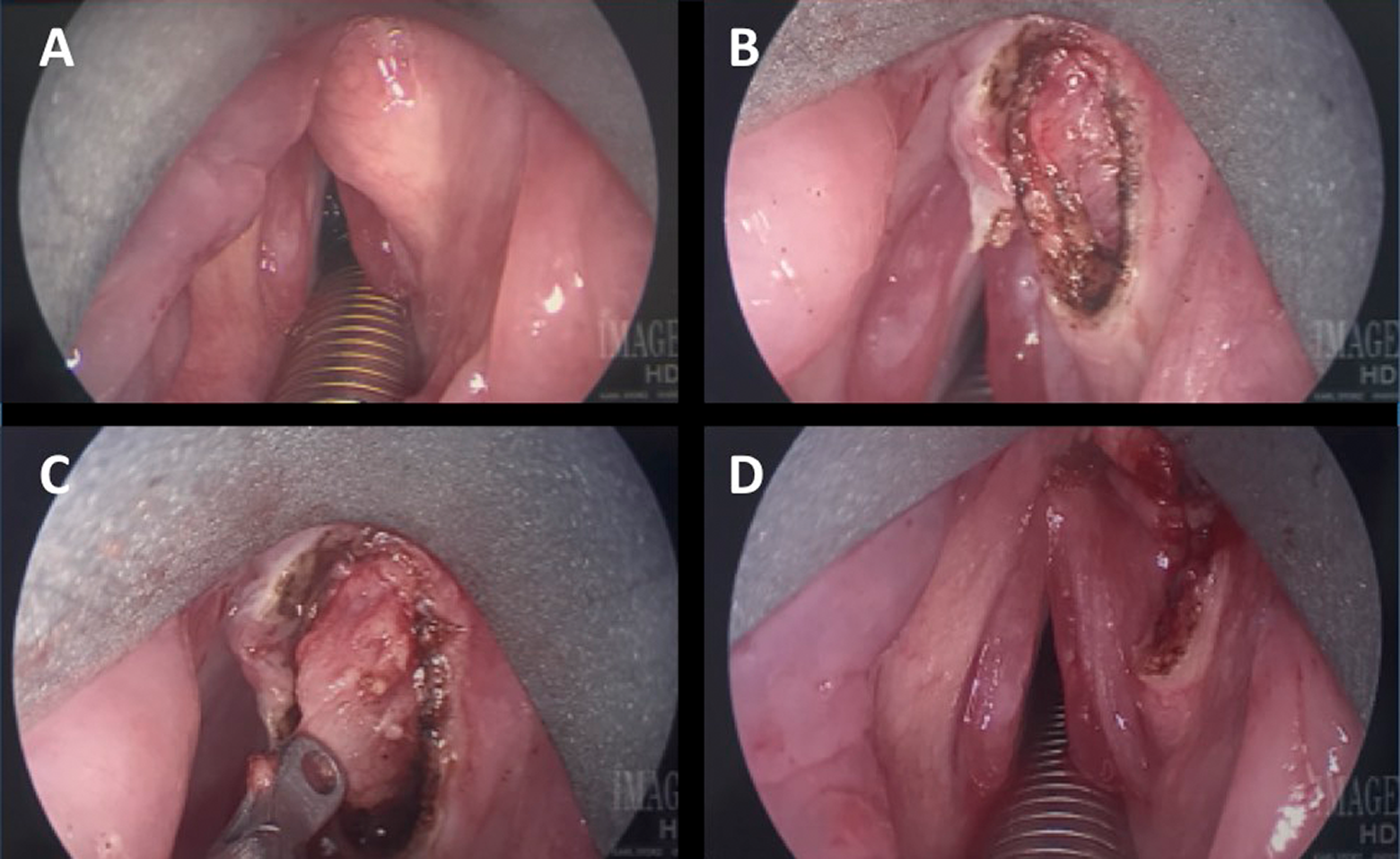
A, Swelling over the right false vocal fold caused by the internal component of right combined laryngocele, (B) mucosal incision over laryngocele, (C) traction on laryngocele wall, and (D) right false vocal fold after laryngocele excision.

Right combined laryngocele.
Follow-up examination revealed no palpable neck mass, and flexible laryngoscopy showed a well-healing scar over the right false vocal fold. The patient was satisfied with her voice quality and swallow function. A head and neck CT at 2 months showed no residual disease.
Historically, external laryngoceles were treated with 1 of 3 external approaches: lateral thyrotomy, lateral laryngotomy, or laryngofissure. Although anatomic exposure is certainly a benefit, drawbacks must be considered. Al-Yahya et al noted that over half of their patients treated for combined laryngoceles using a transcervical approach required a tracheotomy. 1 Additionally, this approach leaves the patient with a scar and places vital structures at risk. 2,3
More recently, with the advent of advanced microsurgical instruments and the CO2 laser, endolaryngeal surgery offers patients substantially decreased morbidity with excellent results. 4 This technique may be more challenging for large internal or combined laryngoceles; however, our case illustrates the possibility of excellent outcomes with few potential complications.
Laryngocele is a rare entity that can pose a challenge to the otolaryngologist. Newer, less invasive surgery offers advantages over traditional, open transcervical surgery. Endoscopic approach to both internal and combined laryngoceles with CO2 laser assistance is an excellent, effective surgical technique. Patients do not require tracheotomy, long hospital stays, or significant pain control making endoscopic excision an excellent option.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.