
Abstract
The purpose of this article is to differentiate pediatric patients with chronic adenoiditis from those with chronic rhinosinusitis (CRS) based on presenting symptoms. A chart review from a tertiary care facility with pediatric patients who presented with suspected CRS from 2006 to 2014 was identified. We compared patient characteristics, clinical symptoms, duration of symptoms, and past medial history using univariate and multivariate logistic regression models. Based on recent literature, utilizing the computed tomography (CT) score, we identified those children with CRS versus those with chronic adenoiditis. Of the 99 pediatric patients included, 22 patients had diagnosis of adenoiditis and 77 had diagnosis of CRS. When purulent rhinorrhea was present with facial pain, CRS was statistically more prevalent than chronic adenoiditis (P = .017). Symptoms including cough (P = .022), rhinorrhea (P = .27), and facial pressure (P = .98) were not predictive of one diagnosis over the other. Past medical history of asthma or allergy was similar in both groups. Smoke exposure was associated with CT scores >5 (odds ratio 2.4, 95% confidence interval, 0.799-7.182). We conclude that purulent rhinorrhea in the presence of facial pain is more indicative of CRS versus chronic adenoiditis. For all other children, an adenoidectomy without the need for a CT scan can be entertained.
Introduction
Chronic rhinosinusitis (CRS) causes significant impact on quality of life and health of the pediatric population. 1 Chronic rhinosinusitis is defined as an inflammation of the paranasal sinuses lasting for at least 3 months. 2 Symptoms in children are not specific to CRS but often include nasal obstruction, facial pain, chronic cough, and purulent nasal drainage. Chronic rhinosinusitis remains primarily a clinical diagnosis. It is difficult to estimate how many children have true CRS and it is most likely misdiagnosed due to overlap with other diagnosis with similar symptoms. Although reliable epidemiological data regarding CRS in pediatric patients are limited, it is now estimated that pediatric CRS is responsible for over 5 million clinic visits per year in the United States alone. 3 The diagnosis of CRS in children based on symptoms has been shown to be variable.
Symptoms that cause CRS in children can be exactly the same as chronic adenoiditis, with some overlap with allergic rhinitis or viral upper respiratory illness. 4 Distinguishing CRS from adenoiditis can have significant ramifications concerning surgical treatment of these entities. A recent study noted that a sinus computed tomography (CT) scan can distinguish the 2 entities based on CT score. 5 Very few studies are available in children, but a recent study noted that the presence of nasal discharge to be the strongest predictor of CRS. 6
Current treatment of CRS consists of medical management, but for those patients who have failed maximal medical therapy, adenoidectomy or endoscopic sinus surgery has been shown to be effective. 7 –9 The objective of this study was to determine whether a symptom or combination of symptoms can distinguish CRS from chronic adenoiditis using the Lund-Mackay CT score based on recent publication. 5
Patients and Methods
We reviewed all children who presented to a tertiary pediatric otolaryngology department between 2006 and 2014 with suspected diagnosis of CRS. Inclusion criteria included children between the ages of 5 and 15 years who had CT scan of the sinuses that was performed at the end of a 3-week course of oral antibiotics as well as topical nasal steroid spray as a part of a presurgical planning. Patients with cystic fibrosis, primary ciliary dyskinesia, immunodeficiency, craniofacial abnormalities, past history of adenoidectomy or sinus surgery, or nasal polyps were excluded from the study. The study was approved through the WVU IRB (WVU KC protocol 1611347172).
Patient age, gender, duration of symptoms, allergy status, asthma status, and smoking exposure history were recorded. Patients with positive allergy testing were considered to be allergy positive. Patient with documented diagnosis of asthma were considered asthma positive. Charts were reviewed for complaints of nasal obstruction, cough, headache/facial pressure, and purulent rhinorrhea. All clinic visits up to the time of the CT scan were reviewed.
The CT scans were reviewed using standard Lund-MacKay scoring parameters. 10 All scans were scored by the senior author. Those patients with CT scores greater than 5 were considered positive for CRS, whereas those with CT score less than or equal to 5 were considered to be chronic adenoiditis only. 5
Analysis
Chi-square test was used to compare variables between those with CT scores less than or equal to 5 to those greater than 5. t Tests were used to compare quantitative variables between the groups (age, duration of symptoms). χ2, t tests, and multiple logistic regression analysis were calculated using R software. 11 Results include odds ratios (ORs), confidence intervals, and P values of symptoms (SXS) nasal obstruction, rhinorrhea, cough, and facial pain, as well as any significant interaction effects.
Results
Ninety-nine pediatric patients aged 5 to 15 years were included. Demographic data, related medical history, and symptoms are shown in Table 1. The diagnosis of CRS was confirmed based on CT score of >5 in 77 children (77%), whereas 22 children (22%) with CT scores ≤5 were diagnosed as having chronic adenoiditis. There was no statistical difference in gender or mean age of the patients. (Mean age for all patients was 8.7 years.) There was no significant association of allergy, asthma, or smoke exposure with CRS in this patient population; however, 48.8% of the patients with CRS did have allergic history.
Characteristics of the Pediatric Patients Included in the Study.
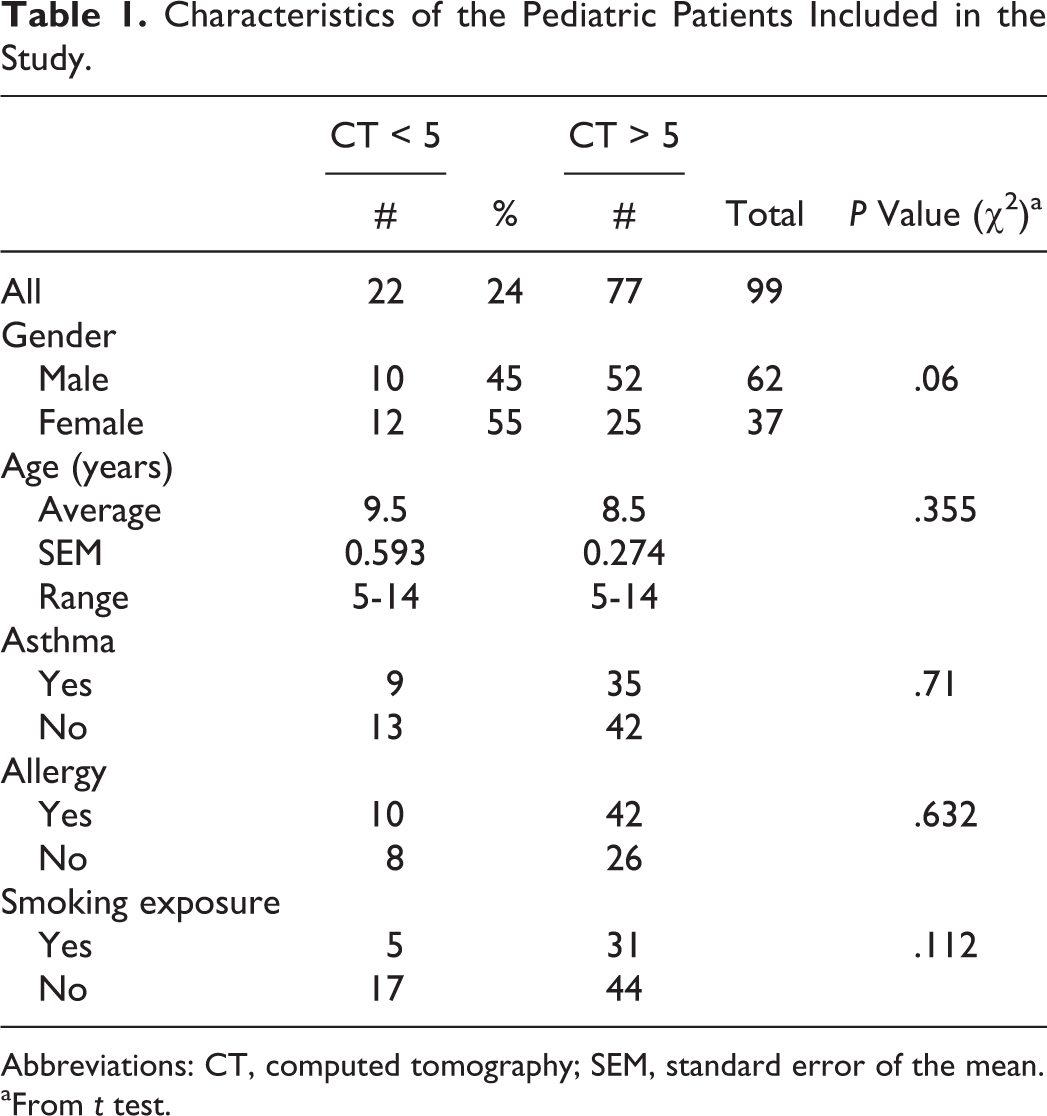
Abbreviations: CT, computed tomography; SEM, standard error of the mean.
aFrom t test.
Analysis of the data shows that symptom of nasal obstruction was present in all patients (both groups). Upon analyzing the rest of the symptoms separately, we found no statistical difference between the 2 groups. 11 As shown in Table 2, logistic regression using only nasal obstruction (SXS 1) as a predictor was observed to provide an “adequate” fit (P = .049).
All Collected Data Multiple Linear Regression Coefficients, χ2, and Odd Ratios With 95% Confidence Intervals.a,b
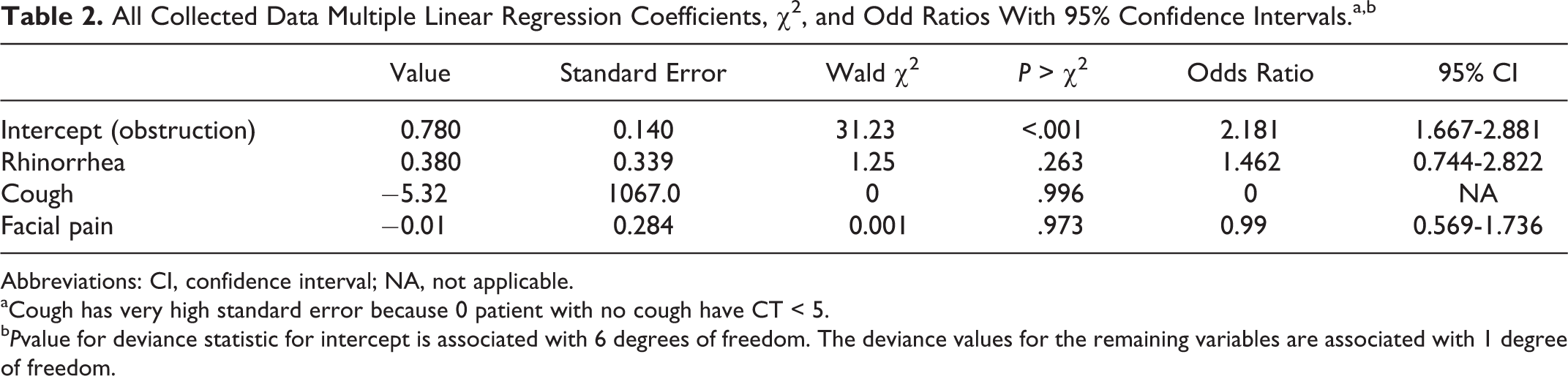
Abbreviations: CI, confidence interval; NA, not applicable.
aCough has very high standard error because 0 patient with no cough have CT < 5.
b Pvalue for deviance statistic for intercept is associated with 6 degrees of freedom. The deviance values for the remaining variables are associated with 1 degree of freedom.
Addition of symptom cough (SXS 3) into the model provided a significant amount of information (P = .022). Purulent rhinorrhea (SXS 2) had a P value of .267 and facial pain (SXS 4) had a P value of .975.
Some interaction effects between the SXS predictors may be present. Since nasal obstruction (SXS 1) is the “intercept” term in this regression analysis (it is present in all patients), its interaction effect is not considered. So there are 3 possible interactions: between SXS 2 and SXS 3, between SXS 2 and SXS 4, and between SXS 3 and SXS 4. Including them in the regression model through a “stepwise” manner shows that the interaction term between purulent rhinorrhea (SXS 2) and facial pain (SXS 4) significantly provides more information (P = .0174). As seen in Table 3, it is clear that the presence of purulent rhinorrhea (SXS 2) and facial pain (SXS 4) always results in a CT score that is greater than 5. 12
Summary of Combination of SXS, 2, SXS 3, and SXS 4 and Probability of CT > 5.a
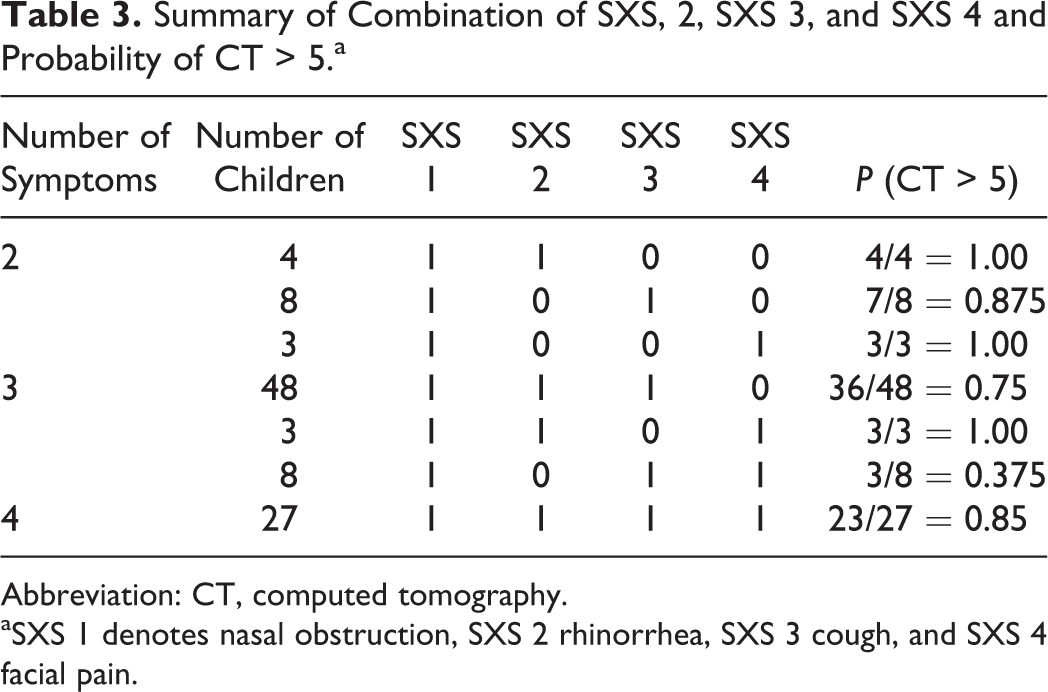
Abbreviation: CT, computed tomography.
aSXS 1 denotes nasal obstruction, SXS 2 rhinorrhea, SXS 3 cough, and SXS 4 facial pain.
Discussion
A recent study by Leo et al concluded that the presence of 3 symptoms, nasal obstruction, cough, and facial pain without rhinorrhea, leads to the diagnosis of CRS in 91% of the children. 6 They did use, however, nasal endoscopy to make the diagnosis of CRS. The aim of this study was to examine those most common symptoms of pediatric rhinosinusitis, but instead use CT scan as gold standard, rather than nasal endoscopy. Adult CRS has been widely addressed and symptoms have been correlated with imaging and endoscopic findings. The diagnosis of CRS based on symptoms as described by the clinical consensus on CRS, purulent rhinorrhea, nasal obstruction, facial pressure, and cough remains difficult. 7 Based on the EPOS recommendation and consensus statement, once 2 symptoms are present, a CT scan may be needed to confirm diagnosis, since all 4 symptoms can be present in one combination or another in both CRS and chronic adenoiditis. 2,7 Our study has shown that the presence of purulent nasal discharge and facial pressure is significantly more characteristic of CRS rather than chronic adenoiditis. In the study by Leo et al, cough, facial pain, rhinorrhea, and nasal obstruction were all significantly increased in pediatric patients with CRS diagnosed with nasal endoscopy. 6 What complicates matters more is the fact that children can have these symptoms with chronic adenoiditis without rhinosinusitis, and the only way one can distinguish between the 2 is a CT scan of the sinuses. Our aim in this review was to find a symptom or a combination of symptoms that can allow the care provider to discern one from the other. This may not be important as far as medical treatment, since the treatment medically is basically the same. However, this can have significant implications as far as surgical treatment. For children with chronic adenoiditis without rhinosinusitis, an adenoidectomy will be sufficient surgical treatment; however for children with CRS, a sinus wash or sinus surgery may be needed rather than just an adenoidectomy alone. 9
Although no difference was seen in asthma or allergy incidence in these patients with CRS, there was an increased risk of CRS with tobacco smoke exposure (OR: 2.4). Work by Sedaghat et al has demonstrated a strong association of tobacco smoke exposure with CRS (OR: 3.9) in an older pediatric patient population similar to our results. 13 The descriptions of the pathophysiology of the smoking-associated CRS continue to advance. Groups have shown changes in the upper airway with smoking exposure, including altered mucociliary clearance, decreased innate immune response, and alterations of olfactory respiratory epithelial differentiation. 14
There are several limitations of the study that need to be noted. All patients were from a single author’s clinic, which may limit the generalizability of the data. All CT scores were rated by the senior author at the time scan was obtained. Based on the results of this study, nasal obstruction was found in both groups and facial pressure/pain is not frequently reported by children. If symptoms of purulent nasal discharge in the presence of facial pain can suggest CRS rather than adenoiditis, then a CT scan may be beneficial to confirm the diagnosis, especially if surgery is being entertained. On the other hand, if these 2 symptoms are not present, then patients can be considered for adenoidectomy without a CT scan being needed.
Conclusions
Diagnosis of CRS in children based on symptoms only is difficult. It is even more difficult based on symptoms alone to distinguish between CRS versus chronic adenoiditis except if a CT scan is used. Based on the 99 children whom we reviewed, we have found that purulent nasal discharge in the presence of facial pressure/pain can statistically differentiate those children with CRS. Nasal obstruction is present in all children with CRS and adenoiditis, making this very common symptom a nonfactor in both those disease entities. If symptoms of purulent nasal discharge in the presence of facial pain can suggest CRS rather than adenoiditis, hence, for presurgical planning, a CT scan may be beneficial to confirm the diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.