
Abstract
Coblation is a novel technology and has a wide application in the field of otorhinolaryngology. We conducted a randomized, noncontrolled study to compare the effectiveness of 2 types of wands used for turbinoplasty for nasal obstruction due to inferior turbinate hypertrophy. Reflex Ultra and Turbinator wands were compared on a total of 150 patients. These patients were divided into a group of 75 patients each in a randomized manner. Results were compared based on the visual analog scale, and objective assessment was done on the basis of endoscopic assessment, that is, Nasal Endoscopic Score (NES). Assessment was done on postoperative day 7, first month, third month, and first year. Both groups demonstrated significant and similar results in long term, but an immediate improvement at 1 week was seen in the Turbinator group. Hence, we conclude that coblation turbinoplasty is an effective technique for turbinate reduction and both wands are equally effective in long term. However, Reflex Ultra has the advantage of mucosal preservation and minimal morbidity, and Turbinator has the advantage of immediate relief in nasal symptoms.
Introduction
Nasal obstruction (NO) is a commonly encountered symptom in otorhinolaryngology clinics and it can be due to various causes such as deviated nasal septum, turbinate hypertrophy, chronic rhinosinusitis with or without polyposis, adenoid hypertrophy, and so on. Inferior turbinate hypertrophy is a very common finding seen as a part of allergic rhinitis, vasomotor rhinitis, and in conjunction with deviated nasal septum as a compensatory phenomenon. Dealing with the turbinate and the associated symptom constitutes an important form of management. Turbinate hypertrophy can be managed in 2 ways either medically or surgically. Patients not responding to medical management are the candidates for surgical intervention.
Surgical management can be broadly grouped as radical procedures and conservative procedures. Radical procedures in the form of turbinectomy can be further grouped as total and partial. Turbinoplasty can grouped as conventional procedures, such as chemical cauterization, electrical cauterization, and submucosal resection with cold steel instruments, and the latest techniques, such as laser-assisted turbinoplasty, microdebrider-assisted turbinoplasty, and coblation turbinoplasty. Although these methods may provide better results than medical treatment alone, adverse effects such as bleeding, crust formation, postoperative pain, synechia, or atrophy of the inferior turbinate are common. 1 -3 Coblation is a relatively novel technique and a minimally invasive procedure. It is a non-heat-driven process and works at a lower temperature, that is, 40°C to 70°C. Energy produced is used to excite electrolytes in a conductive medium to create precisely focused plasma that has a cutting as well as coagulation action. Two basic wands are used for turbinoplasty in the form of Reflex Ultra 45 (Figure 1A) and Turbinator (Figure 1B). Reflex Ultra is a fine-tipped wand and it works like a laser, and Turbinator has a wide tip and it works more or less like a microdebrider. There have been not many studies in the literature as yet regarding the coblation turbinoplasty. The aim of the present study is to determine the efficacy of coblation as a technique for turbinoplasty and to make a comparison between Reflex Ultra and Turbinator.
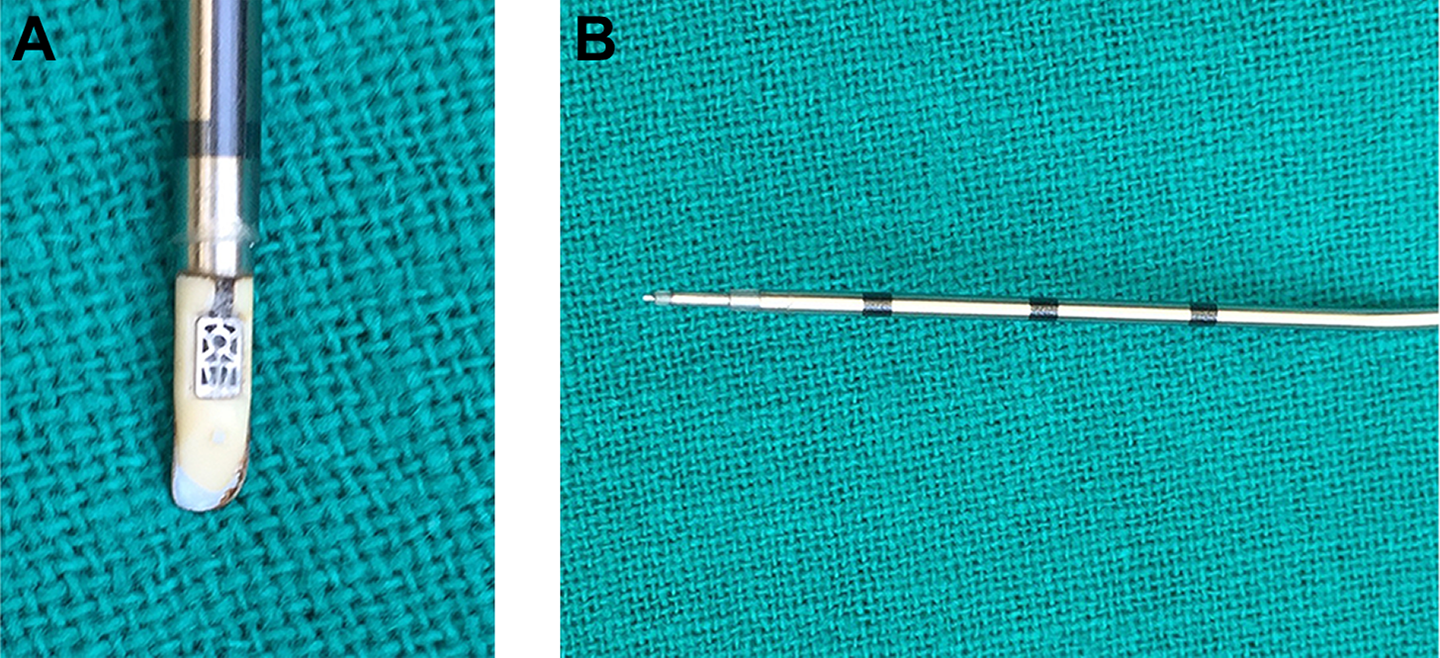
(A) Turbinator coblation wand. (B) Reflex Ultra coblation wand.
Patients and Methods
We conducted a prospective study on 150 patients from a period of January 2015 to February 2016. We decided the sample size using the formula for random sampling:
Inclusion and Exclusion Criteria
Patients were included if they met the following criteria: (1) patients who presented with NO due to turbinate hypertrophy, (2) patients who have enlarged turbinate on nasal examination, and (3) patients refractory to medical management.
Patients who had associated septal deviation and nasal polyposis or had undergone nasal surgery for other causes were excluded from the study.
All patients underwent complete clinical nasal examination, endoscopic evaluation of nose, and nasal cavity computed tomography of the paranasal sinuses to evaluate for associated sinusitis. Patients diagnosed with mucosal hypertrophy of the turbinates were only undertaken for coblation turbinoplasty. Mucosal hypertrophy of turbinates was confirmed by performing decongestant test with 1:100 000 adrenaline cotton pledgets. Patients with evident shrinkage are considered for surgery.
Informed consent was obtained from all the patients, and 75 patients underwent turbinoplasty with Turbinator (group 1) and 75 patients with Reflex Ultra (group 2). These patients were randomized into 2 homogenous groups using random number tables.
Surgical Procedure
The procedure was performed under general anesthesia/local anesthesia according to patient’s preference. Nose was prepared preoperatively with cotton pledgets soaked with 1:100 000 adrenaline, and patients planned for surgery under local anesthesia were given sedation. They were also injected with 2% xylocaine and 1:100 000 adrenaline at 3 parts, the anterior, middle, and posterior end of inferior turbinate, while patients undergoing surgery under general anesthesia were injected with 1:100 000 plain adrenaline.
After achieving adequate anesthesia and decongestion of nasal cavity, plain saline was injected in the turbinates. Coblation device (Smith & Nephew Arthrocarecoblation device, London, United Kingdom) was introduced into the nasal cavity of the patient. The device was inserted at 3 levels, that is, anterior, middle, and posterior end of turbinates. In group 1, we inserted Turbinator, and in group 2, we inserted Reflex Ultra.
Merocel nasal packs were placed in both the nasal cavities of the patient postoperatively for 48 hours. We assessed both the group of patients on postoperative day 7, 1 month, 3 months, and 1 year.
Assessments
Patients were assessed based on the visual analog scale (VAS), with 0 representing no symptoms and 10 the most severe symptoms (severity of nasal discharge [ND], headache [Head], hyposmia [Hyp], and NO); objective assessment was done on the basis of endoscopic assessment, that is, Nasal Endoscopic Score (NES). We scored the size of the turbinate as 1 = small turbinate with no contact with septum and nasal floor, 2 = mild hypertrophic turbinate with slight contact with septum and nasal floor, 3 = moderate hypertrophic turbinate with contact with septum and nasal floor but endoscope could be negotiated through the floor, and 4 = severe hypertrophic turbinate with complete NO with complete contact with septum and floor.
Patients were scored with VAS and NES preoperatively and postoperatively (at postoperative day 7, 1 month, and 3 months). Mean values of both the groups (Turbinator vs Reflex Ultra group) were compared.
Data Analysis
Pre- and postoperative data were collected, tabulated, and analyzed. We used Student t test and χ2 test. We used the IBM software SPSS version 16.0.
Ethical Considerations
The study was approved by the Ascoms Hospital’s ethics committee.
Results
Of the 150 patients, 75 underwent turbinoplasty using the Turbinator wand (group 1) and the remaining 75 underwent turbinoplasty using the Reflex Ultra (group 2). Of these patients, 92 were males and 58 were females.
The mean score of NO, ND, Hyp, and Head for group 1 (Turbinator) at postoperative week 1 was 1.36, 2.43, 2.05, and 5.08, respectively. The mean score NO, ND, Hyp, and Head for group 2 (Reflex Ultra) at postoperative week 1 was 7.75, 4.19, 4.12, and 4.85, respectively.
The P value was <.001 calculated by Student t test. Comparison was done at the end of 1 month, 3 months, and 1 year as well.
At the end of 1 month, the mean score of NO, ND, Hyp, and Head for group 1 was 0.19, 1.16, 0.85, and 4.63 compared to group 2 with a mean of 5.71, 2.68, 2.51, and 3.99, respectively. The P value was <.001 for NO, ND, and Hyp.
At the end of 3 months and 1 year, the P value for NO was <.001 (group 1 mean 0 and group 2 mean 0.19). The mean of ND and Hyp was not significant (Table 1).
Intergroup Comparisons of VAS Scores (Group 1: Turbinator Group, Group 2: Reflex Ultra Group).
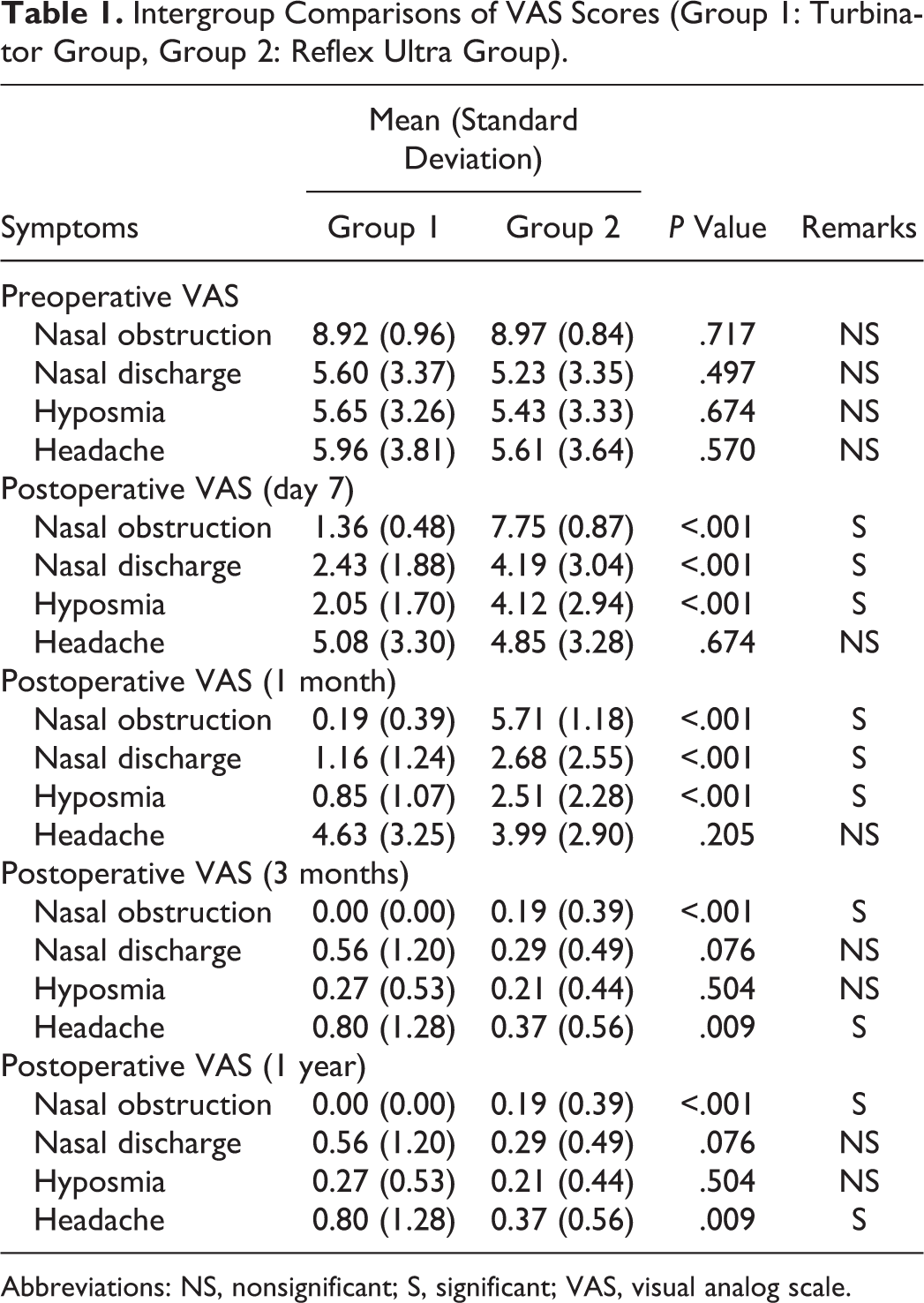
Abbreviations: NS, nonsignificant; S, significant; VAS, visual analog scale.
In case of NES (nasal endoscopic findings) at the end of the first week, in group 1 (Turbinator) patients, there was marked reduction in turbinate size (P < .001) with 100% of patients having grade 2 turbinate according to the grading. In group 1, 80% of patients had grade 2 turbinate at the end of the first week (Table 2 and Figure 2).
Intergroup Comparisons of NES: Nasal Endoscopic Findings (Group 1: Turbinator Group, Group 2: Reflex Ultra group).
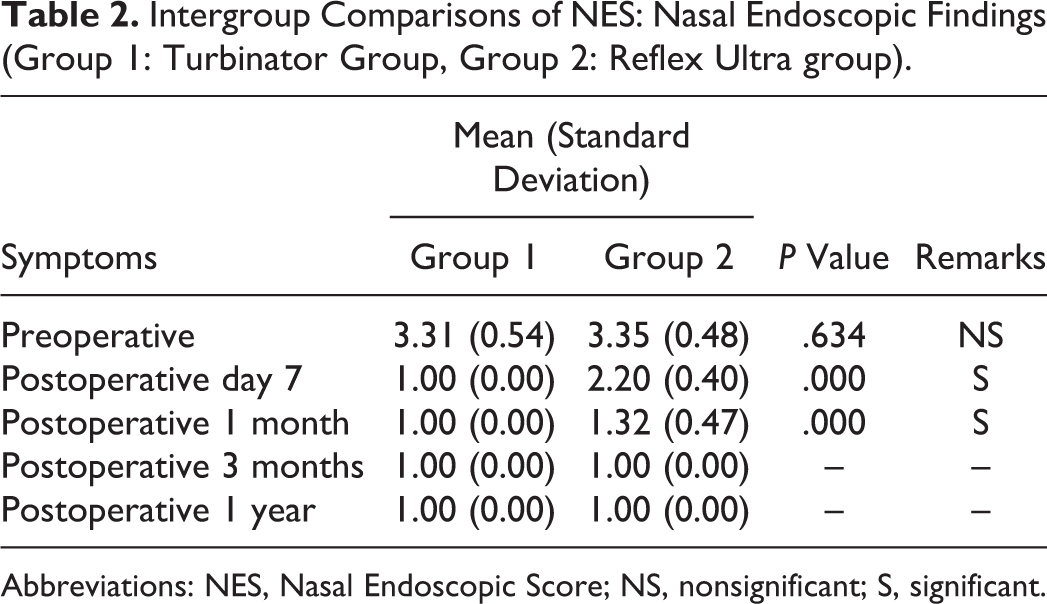
Abbreviations: NES, Nasal Endoscopic Score; NS, nonsignificant; S, significant.
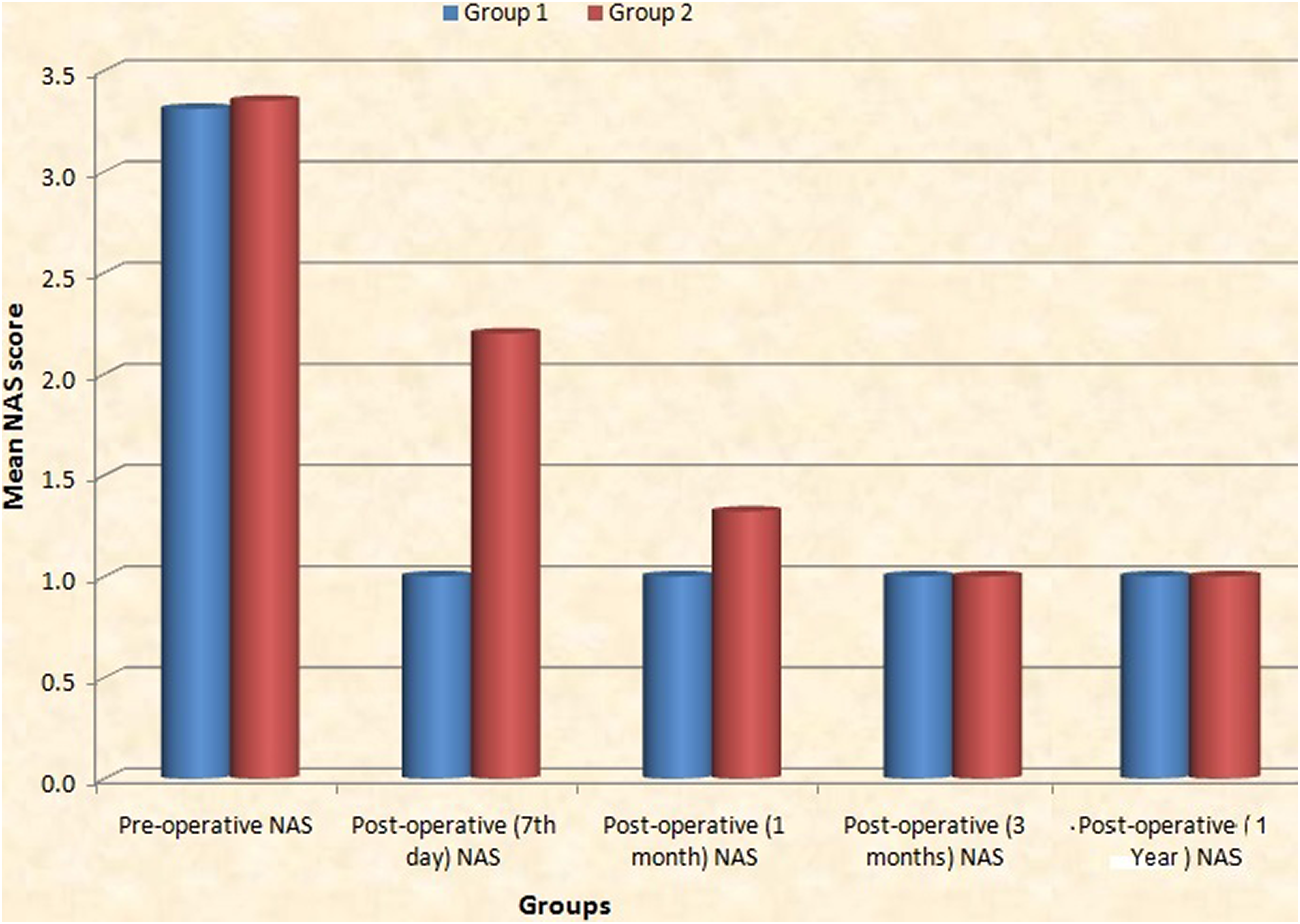
Intergroup comparisons for Nasal Endoscopic Scores (NAS) in group 1 (Turbinator) and group 2 (Reflex Ultra) patients.
At the end of 1 month, 3 months, and 1 year, 100% of patients in group 1 persisted with grade 1 turbinate (small) and 68% of patients in group 2 had grade 1 turbinate, and by the end of 3 months and 1 year, 100% of patients had grade 1 turbinate.
Subjective Symptom Improvements
Severity of NO grades improved significantly during the first week after the operation, in the Turbinator group, and persisted 3 months after the operation. However, a statistically significant improvement in NO grades was only observed during the third month after the surgery in the Reflex Ultra group.
Severity of NO grades improved significantly in the Turbinator group in the first week, the first month, and the third month postoperatively, compared with the Reflex Ultra group (P < .001; Figure 3). At the end of 1 year, the results for NO were similar to the results mentioned at the end of the third month.
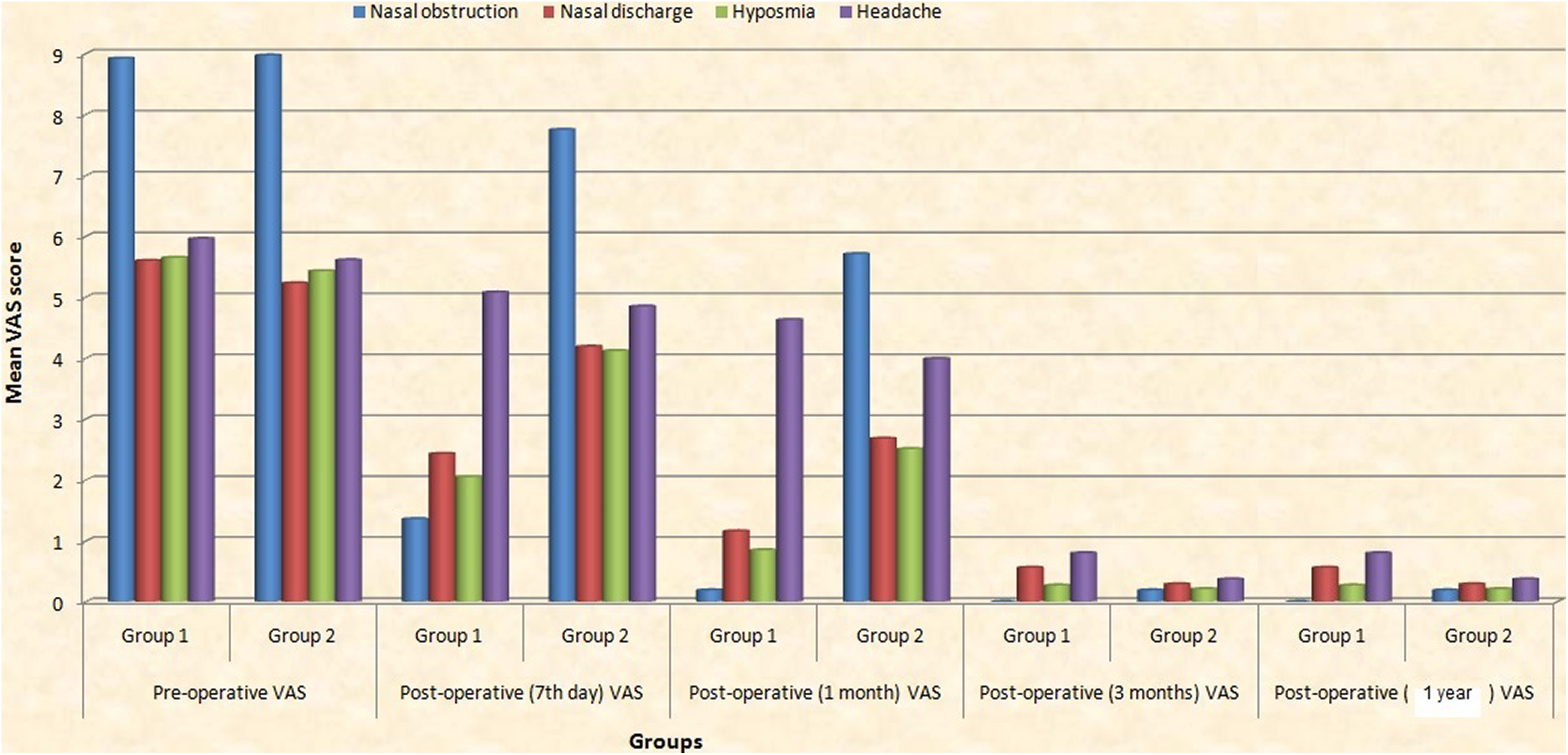
Comparison of visual analog scores (VAS) in group 1 and group 2 patients.
Similarly, severity of ND and Hyp grades improved significantly in the first week of the surgery in the Turbinator group, and there were significant improvements in the same at the end of the first month in the Reflex Ultra Group and persisted at the end of the third month and 1 year.
In case of Head score, there was not much improvement seen in case of both the groups at the end of the first week and the first month. At the end of the third month, group 2 (Reflex Ultra group) showed marked improvement in Head score as compared to group 1 with a P value of .009 (highly significant).
Intergroup comparisons revealed significant differences between the 2 methods in the first week and at the end of the first month (P < .05). The results are summarized in Figures 2 and 3.
Postoperative Complications
Crusting, bleeding, and postoperative pain score were better in cases of Reflex Ultra. In group 1 (Turbinator group), postoperative crusting was noticed in few patients, while pain and bleeding were also seen frequently in group 1 patients.
Objective Symptom Improvements
The mean total NES measured with nasal endoscopy was better in Turbinator group at the end of the first week and persisted at the end of 1 month, 3 months, and 1 year in comparison to Reflex Ultra group where there was significant improvement seen at the end of 1 and 3 months.
Discussion
Inferior turbinate hypertrophy is one of the numerous causes of NO. Medical management is the first-line treatment for turbinate hypertrophy, and turbinates refractory to medical management are then taken up for surgical management. Surgical management can be broadly grouped as radical procedures and conservative procedures. Radical procedures are in the form of total or partial turbinectomy, and conservative procedures are grouped as submucosal resection, coblation-, laser-, and microdebrider-assisted turbinoplasty. With radical procedures, NO decreases sufficiently; bleeding and mucosal damage are 2 major disadvantages related to this method. A better approach may be the “submucosal turbinoplasty,” as preferred by some surgeons, in order to preserve mucosal functions of the inferior turbinate article. 2,4 Conservative procedures have the advantage of preserving the mucosa over the radical procedures and causing minimal morbidity.
In our study, we studied the use of coblation as a technique for turbinoplasty and compared the efficacy of 2 wands—the Turbinator (group 1; Figure 4) and Reflex Ultra (group 2; Figure 5). Turbinator works very similar to microdebrider in that it has more of a cutting action. Reflex Ultra works like a radiofrequency laser in that it causes shrinkage of turbinate with thermal effects. Little is known in the literature about the 2 wands; to the best of our knowledge, we could not find any reference in the literature comparing the 2 wands.
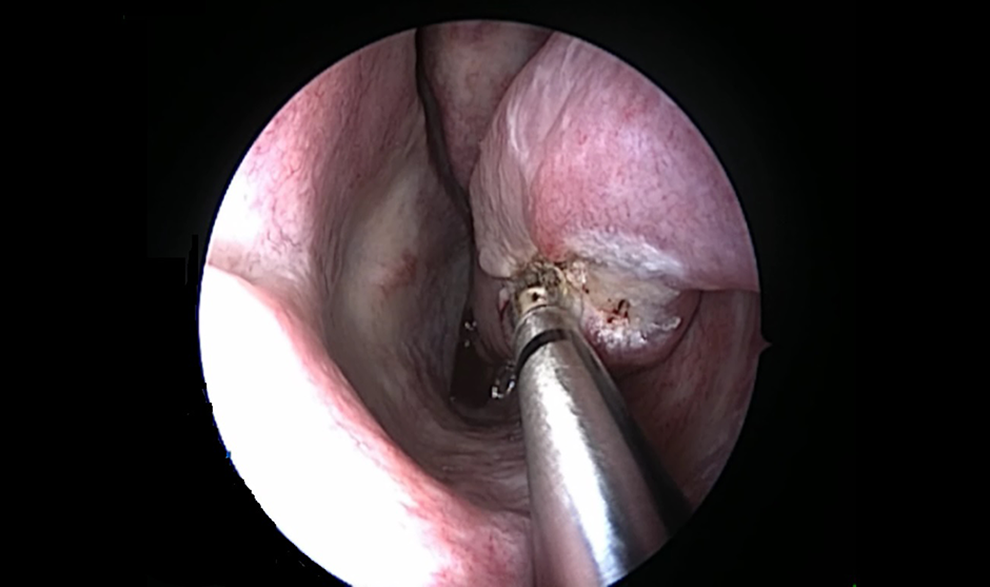
Turbinator wand in the left nasal cavity.
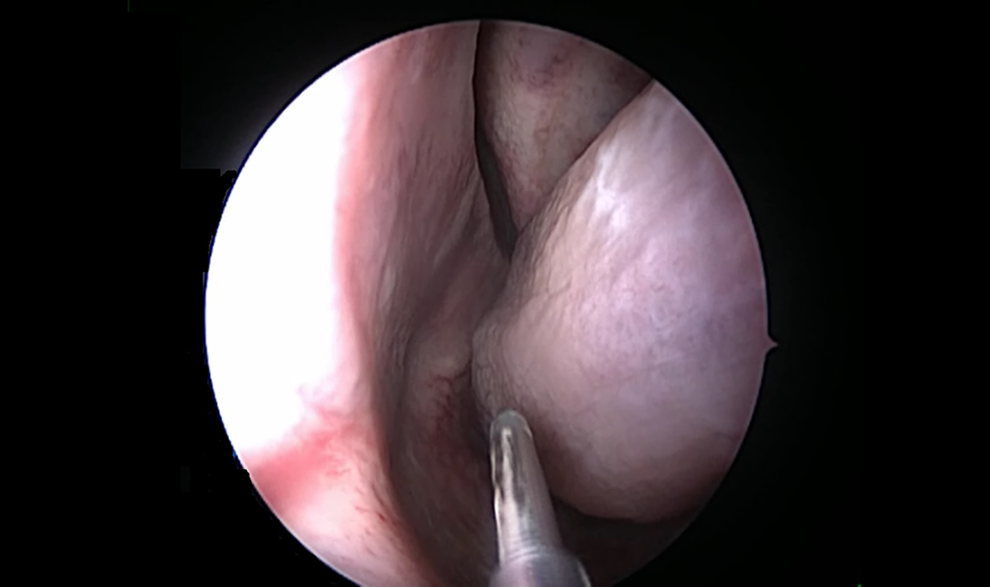
Reflex Ultra wand in the left nasal cavity.
Hence, we took up this pilot study to compare the 2 wands and come to a consensus which is better to perform turbinoplasty. In a recent study, Cingi et al applied radiofrequency and microdebrider-assisted turbinoplasty in a group of 268 patients and their findings were similar to our study. In radiofrequency group, improvements in NO were only observed during the first month after the surgery. Significant improvement was seen in the first week and the first month in NO, Hyp, and ND scores in microdebrider group (P <.05) as seen in our Turbinator group (group 1, P < .001); hence, they concluded the efficacy of microdebrider to be better in terms of cost factor and short- and long-term effects. 5
On the contrary, different results were obtained in another study by Kizilkaya et al where similar comparison was done between microdebrider and radiofrequency group. They found worsening of symptoms such as NO and Hyp in initial first few days and improvement at the end of the first postoperative week in the microdebrider group and that persisted for long term. 6 In comparison to radiofrequency group where there was improvement seen in the initial first few days and it persisted long term. In our study an immediate improvement was seen in Turbinator group compared to Reflex Ultra group. In intergroup comparisons, they found results to be similar for both the groups, which was similar to our results.
Effects of radiofrequency alone were evaluated in a study with a long-term follow-up of 2 years by Akdag et al on symptoms such as nasal itching, Head, Hyp, snoring, sneezing, and crusting. They found delayed onset of improvement in symptoms, that is, at least 3 months postoperative but long-term persistence of improvement in symptoms, which was similar to our results in Reflex Ultra group of patients of our study. 7
Vijay Kumar et al recommended microdebrider-assisted inferior turbinoplasty in comparison to radiofrequency-assisted turbinoplasty due to faster relief in various nasal symptoms and zero recurrence rate. 8 Lee and Lee evaluated 60 patients with inferior turbinate hypertrophy, 30 underwent microdebrider-assisted turbinoplasty and 30 were treated with radiofrequency-assisted turbinoplasty. They followed up patients at 3, 6, and 12 months after surgery. They also performed acoustic rhinomanometry at 12 months after the operation. They found results to better in the microdebrider group. 9 In the present study, we compared Turbinator group (group 1) and Reflex Ultra group (group 2) and found in the Turbinator group that there was early relief in symptoms associated with turbinate hypertrophy and that the relief was long term. In patients of Reflex Ultra, the improvement in symptoms appeared later at the end of the first month, but it was persistent.
The improvement in patency of airway at the end of 1 month, 3 months, and 1 year was similar in both the groups but was immediate in the Turbinator group, that is, at the first week. Individual group analysis revealed that in Turbinator group, there was marked improvement in symptoms such NO, ND, Hyp, and Head at the end of the first week, first month, and third month, and a similar trend was seen in Reflex Ultra (group 2) patients, except that the onset of improvement was a bit delayed, that is, at the end of the first month. At the end of 1-year follow-up, we noticed that the score for VAS and NES remained persistent as seen at the end of the third month.
The immediate relief of symptoms in the Turbinator group can be attributed to its cutting action on the submucosal tissue and bony tissue, which leads to an instant reduction in size of the turbinate. The delayed onset of improvement in Reflex Ultra group is because it causes a tissue reaction of fibrosis that has a latency period to set in, hence leading to a slow yet sustainable improvement. The constant improvement in scores at every follow-up in both the groups is due to a tissue reaction that sets in, after the use of both the wands, leading to shrinkage in the size of the turbinate at every interval. With Reflex Ultra wand, the fibrosis caused by its thermal action is slow in onset but has a long-term effect, that is, it is persistent at the end of 1 year, which is an advantage over the radiofrequency probe that acts on same principle of Reflex Ultra but has a short-term effect. 5 Even Turbinator wand used in our study had a long-term effect on the turbinate.
When comparing the 2 wands in terms of results, they are equally efficacious, with a few advantages of one wand over the other.
In terms of mucosal action, Reflex Ultra was better, but in case of bone cutting, Turbinator was more efficacious. So when working at the anterior and middle part of turbinate that is bony, Turbinator should be used, and when working at the posterior part of turbinate that constitutes of mucosa mainly, Reflex Ultra is better.
Another disadvantage of Turbinator was that it caused more postoperative crusting and bleeding compared to Reflex Ultra with nil postoperative crusting and bleeding. The procedure satisfaction at the end of the first month and 1 year was similar with both the wands.
Some studies advocate the use of radiofrequency (Reflex Ultra) as it has a mucosal action and preserves the integrity of nasal mucosa, hence preserving the mucociliary function of nose. The only disadvantage of Reflex Ultra is that it will not act at bony areas and many patients require radical approach, so in such group of patients, the use of Reflex Ultra will lead to unsatisfactory results. 6
“Partial success” of both procedures, on symptoms such headache, led us hypothesize that cause of headache could not be turbinate hypertrophy alone but there might be other attributing causes as well.
Conclusions
We found both the wands to be effective when comparing the postoperative procedure satisfaction and NES, though there were some advantages and disadvantages of both the wands. Turbinator was effective at bony part of turbinates where Reflex Ultra was ineffective; it also gave immediate relief to patients as compared to Reflex Ultra. Reflex Ultra had the advantage of minimal mucosal trauma and minimal postoperative crusting as seen in Figure 6, though the onset of relief in symptoms was much later with it.
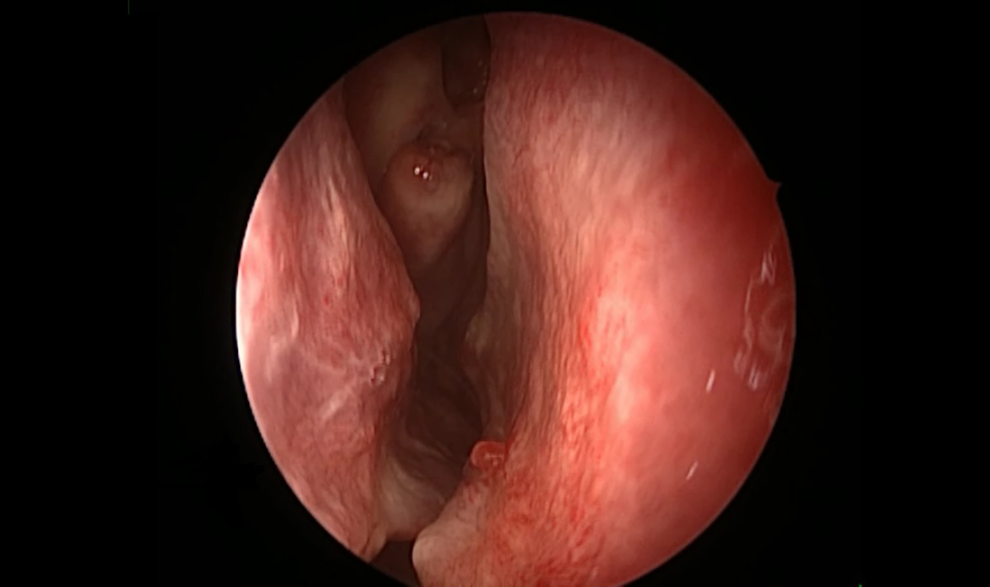
Postoperative appearance of right inferior turbinate using Turbinator wand.
Footnotes
Authors’ Note
Paper presented at 28th Annual conference of All India Rhinology Society National Conference, “RHINOCON 2015” at Bareilly, November 29, 2015. Awarded First prize for the presentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentation
Paper presented at 28th Annual conference of All India Rhinology Society National conference, “RHINOCON 2015” at Bareilly, November 29, 2015. Awarded First prize for the presentation.