
Abstract
Tyrosine kinase inhibitors (TKIs) aid in prolonging life in patients with advanced locoregional thyroid malignancy. Such patients may undergo total laryngectomy for local disease control and tracheoesophageal puncture (TEP) for speech rehabilitation. Enlargement of TEP fistulas is usually attributed to wound healing issues and leads to major complications. Four laryngectomies with TEP were performed between 2015 and 2016 and subsequently placed on a TKI. Three patients developed a complication after TKI treatment, and 2 patients had a tracheoesophageal fistula. Patients should be counseled about possible wound healing risks associated with TKIs.
Keywords
Introduction
The incidence of thyroid malignancy in the United States has increased on average 3.6% per year since 1974, and advanced stage thyroid malignancy has increased 3.5% per year. 1,2 Additionally, thyroid cancer incidence-based mortality has increased by 1.1% per year over the last 20 years, which has fueled the need for additional adjuvant therapy to treat patients with advanced disease. 1 As advances in adjuvant therapy improve, survival rates for patients with poorly differentiated thyroid malignancy and advanced locoregional thyroid malignancy are increasing. 3 Biologics, specifically, tyrosine kinase inhibitors (TKIs), have aided in prolonging life in these patients. 4,5 However, as with other biologics, these medications are relatively new and, while generally well tolerated, can have serious and even life-threatening side effect profiles that are poorly understood. 6 As patients continue to do well on these medications and their use increases over time, these side effect profiles become more evident. 6
In selected cases, patients with advanced thyroid malignancy undergo total laryngectomy for local disease control. Several options for speech post-laryngectomy are available for these patients, including tracheoesophageal puncture (TEP) prostheses. 7 In this instance, a prosthesis is placed in a fistula between the trachea and esophagus allowing air to travel through the esophagus into the oral cavity for resonant speech. 7 However, enlargement of TEP fistulas can cause esophageal leakage into the airway causing complications and is usually attributed to wound healing issues related to prior radiation or patient-related comorbidities. 8,9 In this case series, we present 4 patients who have undergone total laryngectomy with TEP for either poorly differentiated or locally invasive thyroid malignancy and for speech rehabilitation, who were subsequently treated with TKI.
Case Report
Patient 1 (Table 1) is a 64-year-old male who underwent a total thyroidectomy and total laryngectomy for recurrent follicular thyroid cancer in December 2015 with primary TEP with negative margins. He was subsequently discharged after an unremarkable postoperative course. He then underwent radiation therapy for local control ending in April 2016 and was started on lenvatinib therapy beginning September 2016. In May 2017, he began to have leakage from TEP site and required packing of TEP site and removal of TEP. Lenvatinib was stopped at this time. He required jejunostomy tube placement in June 2017. An attempted repair of his fistula took place in October 2017; however, this was aborted as the fistula was too large extending into the thoracic cavity. Subsequently, he underwent repair in January 2018 that required resection of the left clavicular head and mini-sternotomy for access to the fistula site and a deltopectoral flap, which was delayed. His fistula closed, and he resumed oral intake in April 2018. He remains euthyroid on replacement. He has remained off lenvatinib with lung nodule enlargement suggestive of possible remote disease progression.
Patient Demographics and Treatment Information.
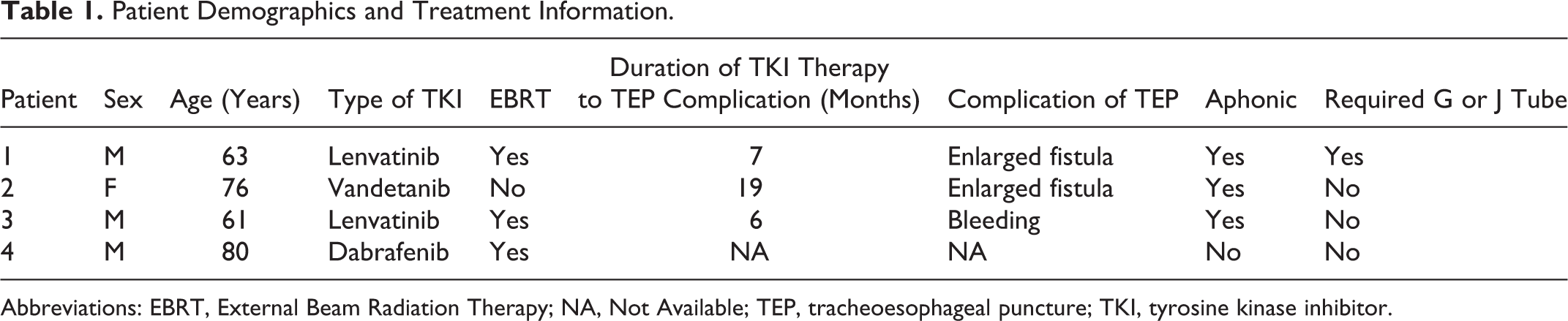
Abbreviations: EBRT, External Beam Radiation Therapy; NA, Not Available; TEP, tracheoesophageal puncture; TKI, tyrosine kinase inhibitor.
Patient 2 is a 76-year-old female with a distant history of total thyroidectomy for papillary thyroid carcinoma who underwent total laryngectomy with primary TEP in May 2016 for cricoid and tracheal involvement of poorly differentiated carcinoma with negative margins. She started vandetanib in July 2016. In January 2018, she developed breakdown around the TEP with bleeding and a fistula formation. Her vandetanib was stopped in January 2018. An endogastric feeding tube was placed in April 2018. Currently, she is undergoing TEP fistula repair.
Patient 3 is a 62-year-old who underwent total laryngectomy with primary TEP for rapidly progressive, poorly differentiated thyroid carcinoma with negative margins in January 2016. He was treated with external beam radiation postoperatively, ending in April 2016. He started lenvatinib in July 2017. In December 2017, he started to have bleeding around his TEP and was unable to use the TEP. This continued and his lenvatinib was stopped in February 2017 secondary to bleeding. He currently had dramatic progression of distant disease and is on hospice care.
Patient 4 is an 80-year-old male who underwent total laryngectomy in August 2016 for advanced locoregional papillary thyroid cancer with primary TEP placement with negative margins. He began dabrafenib therapy in November 2016 which was briefly held for external beam radiation in December 2017; he has had no more treatment breaks. He continues to use his TEP and has had no major complications and only occasional leakage after several months of use which resolves with replacement of prosthesis.
Discussion
In this article, all total laryngectomies and TEP were performed by the senior author over a 1-year period from 2015 to 2016. Three of 4 patients who underwent primary puncture with total laryngectomy developed a complication after treatment with a TKI despite excellent initial results, and 2 of 4 patients had a tracheoesophageal fistula (TEF) associated with their TEP. In 2 patients, radiation therapy was performed, a well-known risk factor for impaired healing; however, radiation has not directly correlated with an increased rate of TEP fistula enlargement. 10,11 These complications were delayed and occurred only after the initiation of TKI therapy. The potential for TKI as a potentiator of TEF enlargement is plausible and we believe this is the first time in the literature that this has been proposed. In the practice of the senior surgeon, TEP is no longer routinely performed for patients with thyroid carcinoma and distant disease who will likely require TKI therapy in the future.
Tracheoesophageal punctures can be placed primarily at the time of surgery or secondarily in a delayed fashion sometime after laryngectomy. All TEPs at our institution were placed primarily. There is mixed evidence regarding whether there are higher rates of fistula enlargement in primary versus secondary TEP. One meta-analysis found a higher rate of fistula enlargement in primary TEP versus secondary TEP (odds ratio: 1.99; 95% confidence interval: 1.07-3.70; P = .003). 12 Two other systematic reviews showed no difference in fistula enlargement rates. 13,14 Three studies saw similar rates of other complications (wound infection, bleeding, stomal stenosis, leakage), but no reviewed study showed a complication rate higher than 49% or a TEF rate higher than 39%. 12 –14 In this study, all 4 patients had primary TEPs that may have contributed to the higher rate of fistula.
Postsurgical wound healing complications associated with TKIs are poorly described. 6 Most literature on the subject describes poor wound healing related to intra-abdominal adhesions. 6,15 There is evidence that VEGF expression increases with skin injury and that reduced expression leads to impaired angiogenesis and granulation tissue formation. 16,17 In addition, EGFR inhibition has also been shown to inhibit angiogenesis. 18 These factors may lead to the uncommon side effects of TEF and stomach perforation (1%-3%) associated with these agents. 6 Decreased angiogenesis could also explain why TEF is more common after radiation with VEGF inhibitor use. 19 Ultimately, the patients in this report did not develop fistula enlargement until after the initiation of the TKI, even though they had the TEP for months or years without evidence of recurrence. Interestingly, the only patient in our study who did not develop significant TEP complications was treated with dabrafenib, a BRAF inhibitor.
Conclusion
We have presented 3 patients with TEP complications after initiation of TKI for advanced thyroid malignancy in the setting of prior TEP. Two of these patients underwent permanent removal of the TEP and subsequent closure of the fistula. The rates of fistula enlargement are higher than those reported in the literature. We recommend that all patients with a TEP who are considering therapy with a TKI or all patients who are on a TKI considering a TEP be counseled about high complication risks associated with wound healing and fistula enlargement and possibly undergo secondary TEP or avoid a TEP altogether. In our practice, we advise against TEP in patients who are likely to require therapy with TKI in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.