
Abstract
Background:
Horner syndrome caused by metastatic squamous cell carcinoma of the head and neck is not common, and when diagnosed, may have serious clinical implications. We aim at highlighting the clinical significance of this finding.
Methods:
We retrospectively reviewed charts of 6 patients with Horner syndrome secondary to metastatic head and neck squamous cell carcinoma (HNSCC) in the neck.
Results:
All 6 patients had pathologically confirmed nodal metastatic HNSCC. There was one unknown primary and in the remaining 5 patients the primary tumor was identified in the oropharynx, larynx, and oral cavity. Three patients died within 1 month of diagnosis, before initiation of any treatment. One patient received radiation only while 2 patients received chemoradiation with cisplatin as the tumors were unresectable given carotid sheath involvement. Median survival was 4.5 months. Only 1 out of the 6 patients survived and had complete resolution of Horner syndrome after treatment.
Conclusion:
This is the first case series of neck metastasis from mucosal HNSCC as an unusual cause of Horner syndrome and is usually associated with very poor prognosis.
Introduction
Horner syndrome is characterized by ipsilateral miosis, ptosis, and anhidrosis secondary to disruption of the oculo-sympathetic nerve fibers present in the sympathetic chain. Within the neck, tumors, trauma, iatrogenic injury during neck surgery, and internal carotid artery pathology (dissection, aneurysm) are common causes. Interestingly, even with the close proximity of the sympathetic chain to the carotid vessels and the propensity of cervical nodal metastases to develop extracapsular spread with subsequent carotid involvement, Horner syndrome is not a typical manifestation. Only one previous case of Horner syndrome secondary to metastatic squamous cell carcinoma involvement of the carotid sheath has been reported. 1 To our knowledge, no other cases of metastatic oral, oropharyngeal, or laryngeal cancers to the cervical nodes have been identified as the cause of Horner syndrome.
We present a case series of 6 patients with Horner syndrome secondary to metastatic squamous cell carcinoma in the neck. We performed a retrospective review of these 6 patients who presented between 2014 and 2017. Each patient was histologically diagnosed with metastatic head and neck squamous cell carcinoma (HNSCC) via biopsy of the primary site (5 patients) or cervical node FNA for the unknown primary (1 patient). The charts were reviewed for patient demographics, tumor characteristics, radiological findings, treatment, and outcomes.
We highlight the importance of radiological imaging of the carotid sheath and prognosis of this group of patients who present with unusual neurological signs.
Illustrative Cases
All 6 patients (5 males and 1 female) were diagnosed with pathologically confirmed metastatic HNSCC (Table 1). There was 1 unknown primary and in the remaining 5 patients the primary tumor was identified in the oropharynx (n = 3), larynx (n = 1), and oral cavity (n = 1). The neck disease was staged as N2 in 5 patients and N3 in 1 patient with radiological imaging showing nodal disease involving the carotid sheath. The site of sympathetic chain involvement was below the carotid bifurcation in 5 patients and both above and below the bifurcation in 1 patient. The degree of carotid sheath encasement ranged from 70°-360°. The etiology of the Horner syndrome was either nodal disease (n = 5) or direct extension of the primary tumor (n = 1) as visible on computed tomography (CT) images (Figure 1). History of a neck mass, hoarseness, and dysphagia at initial presentation were common to all cases. Two patients presented with shoulder pain and numbness ipsilateral to the Horner syndrome, and were found to have concurrent brachial plexus involvement. Three patients were dead within 1 month of diagnosis, before the initiation of any treatment. One patient received radiation only while 2 patients received chemoradiation with cisplatin as the tumors were unresectable given carotid sheath involvement. The median follow-up for these 3 patients was 14 months. Overall median survival was 4.5 months (range 4 weeks to 40 months). Only 1 out of the 6 patients survived after undergoing a salvage neck dissection for persistent disease following chemoradiation and showed complete resolution of Horner syndrome after surgery. This patient had human papillomavirus–positive disease and has been disease free for 40 months. The clinical and radiological presentations along with the clinical course of the 6 patients in this series are represented in Table 2. We are discussing only the 2 patients who had an unexpected clinical course. The rest of the 4 patients presented with advanced stage disease, and were referred for palliative chemoradiation, out of which 3 died before initiation of treatment and 1 died after completion of treatment due to residual disease.
Demographics of Patient Group.
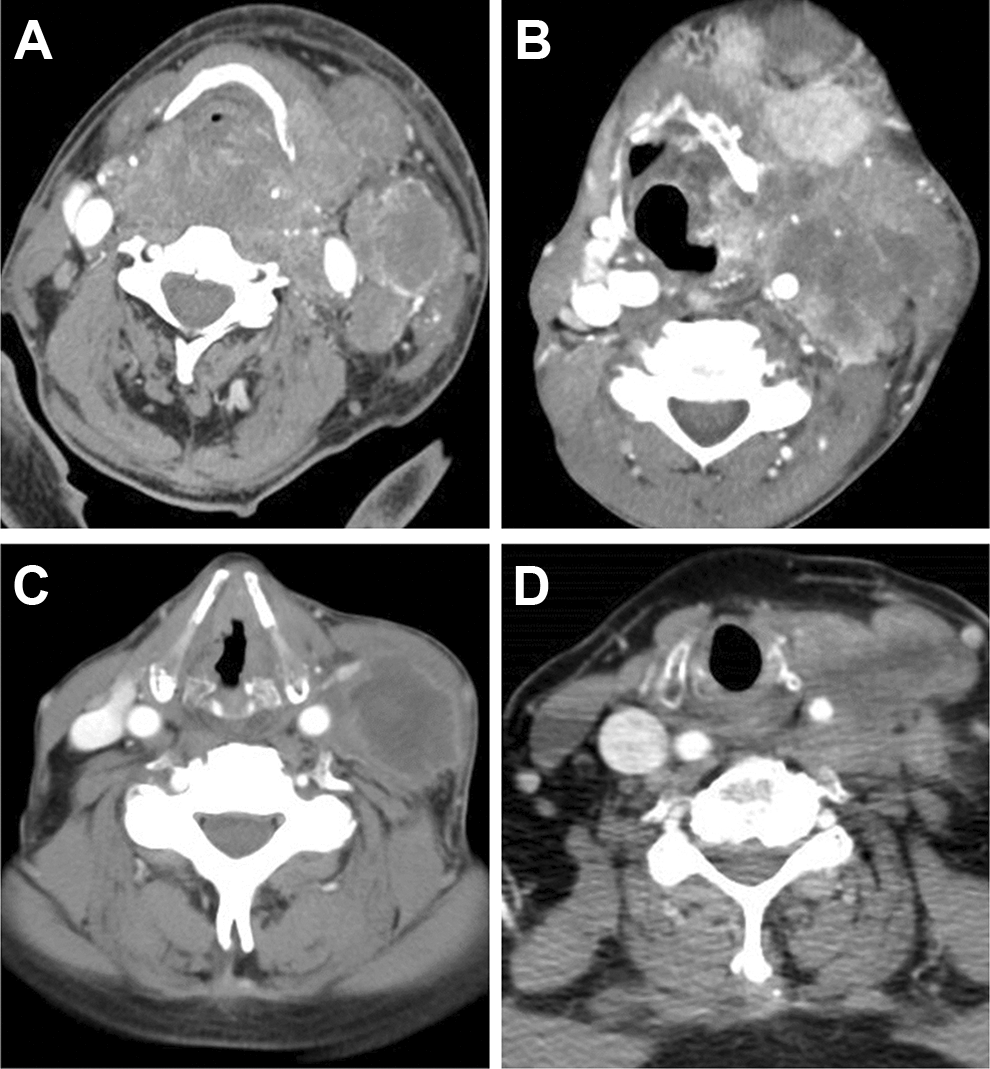
Examples of carotid encasement by primary disease (A) and nodal disease (B-D).
Summary of Clinical and Radiological Presentation and Outcome of the Patient Group.
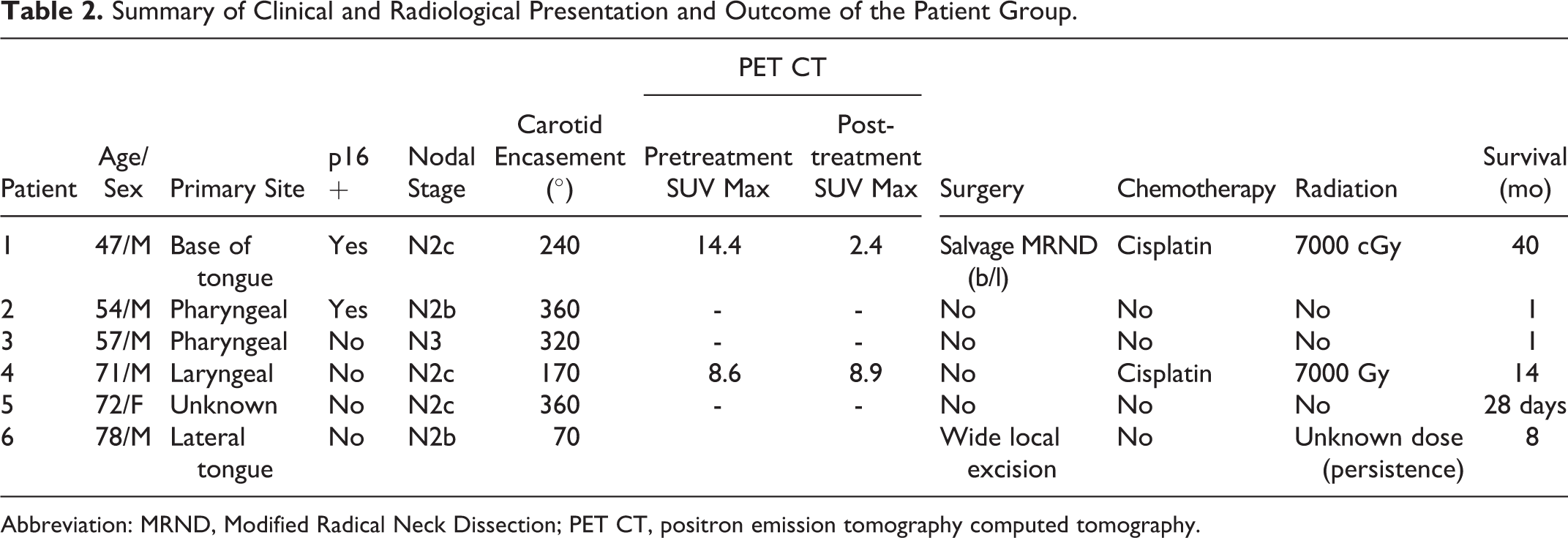
Abbreviation: MRND, Modified Radical Neck Dissection; PET CT, positron emission tomography computed tomography.
Case 1
A 47-year-old male with a 20-pack year smoking history presented with a 7-month history of enlarging neck mass and dysphagia. On examination, left base of tongue firmness, bilateral 2 cm lymph nodes in level 1b, and a large conglomerated lymph node mass in left levels 2 and 3 that were approximately 5 cm in size were noted. Neurological examination was positive for left-sided Horner syndrome without any other neurological deficits. Patient subsequently underwent FNA and panendoscopy with biopsy which returned as p16 positive squamous cell carcinoma. The patient was staged as T4aN2cM0 oropharyngeal cancer and underwent primary chemoradiation with cisplatin (Figure 2). Post-treatment positron emission tomography scan showed residual disease in the neck and patient subsequently underwent modified radical neck dissection (Figure 3). Interestingly, his Horner syndrome resolved completely 3 months following surgery. The patient is alive and has been disease free for 40 months.
The CT showing pretreatment carotid sheath involvement in surviving patient. CT indicates computed tomography.
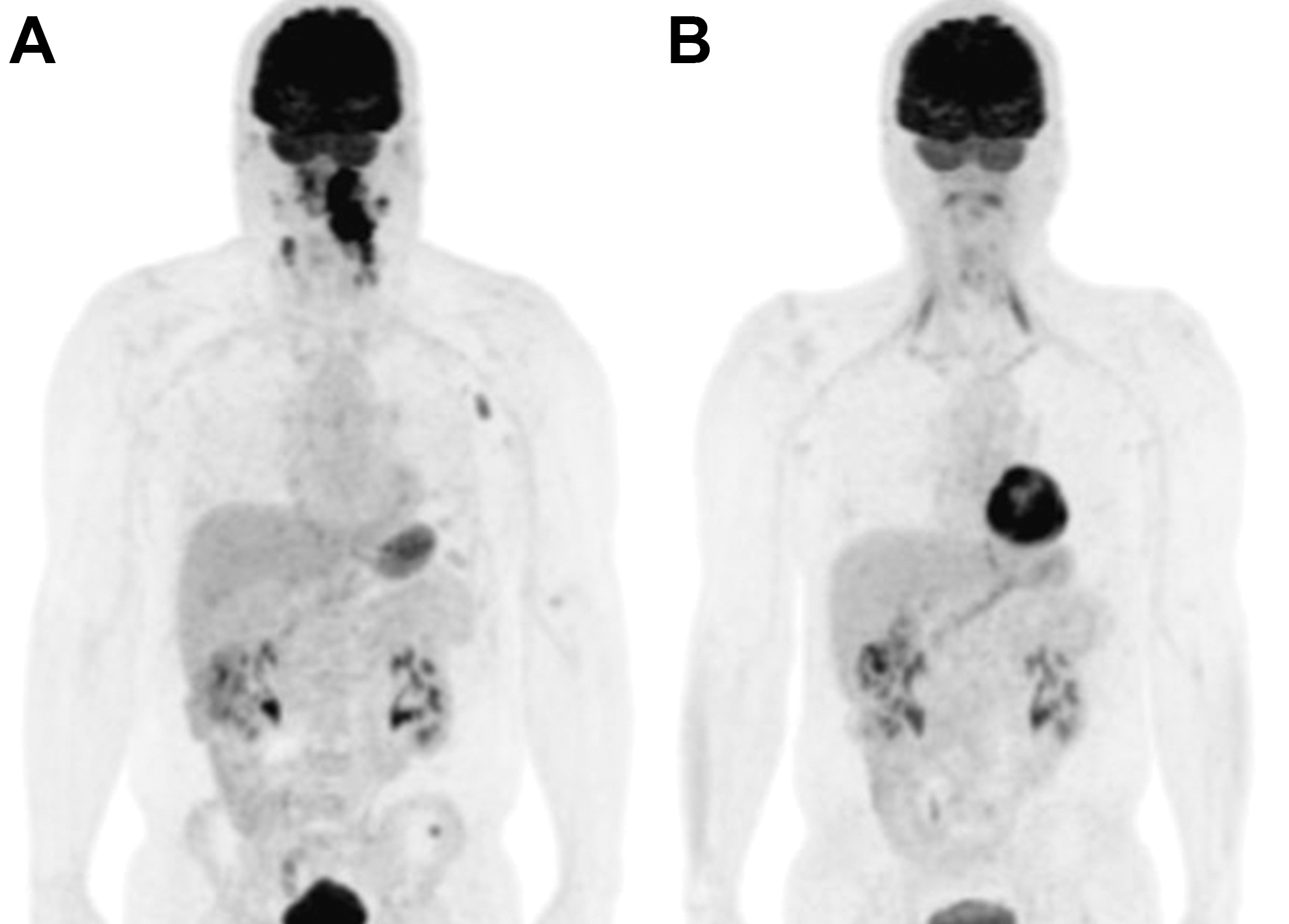
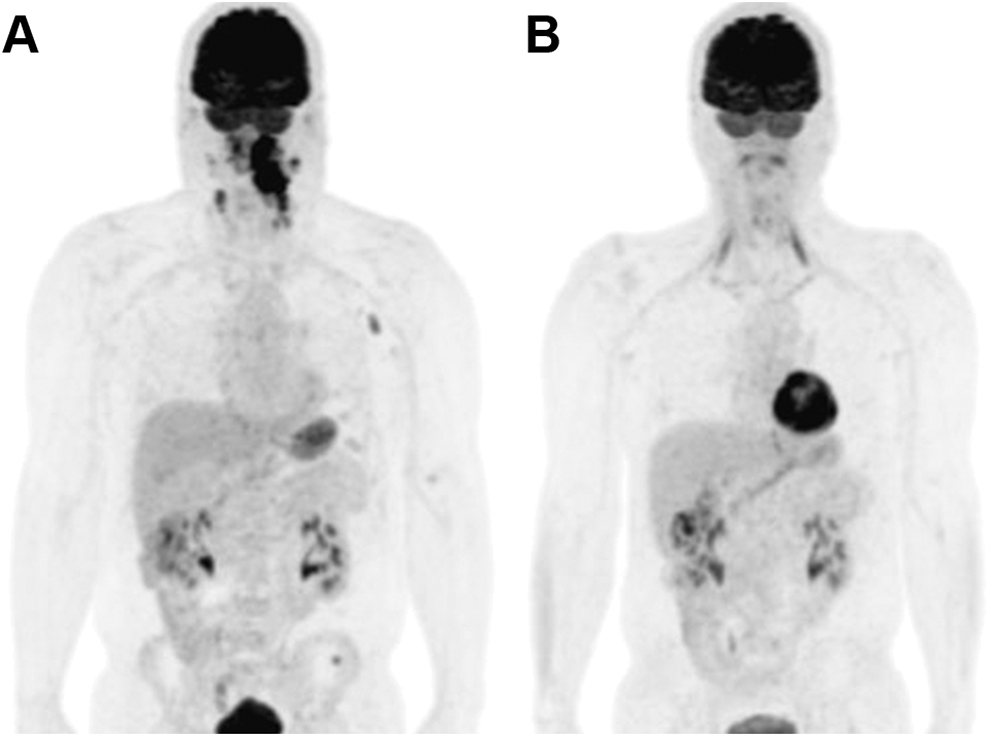
The PET before (A) and after (B) salvage Modified Radical Neck Dissection .
Case 2
A 78-year-old male with a T1N1M0 squamous cell carcinoma of the right lateral tongue presented to us status post wide local excision of the tongue lesion and external beam radiation for the neck node at an outside facility. On examination, the tongue showed no lesion but the neck had multiple, fixed right level 2 and 3 lymph nodes none larger than 6 cm. He was also found to have right-sided Horner syndrome. Patient was evaluated further to assess resectability of the neck nodes. The CT neck showed an encased carotid with no fat planes around it, and hence, the disease was deemed unresectable and referred for palliative chemotherapy. Patient had an overall survival of 8 months from diagnosis.
Discussion
Horner syndrome is characterized by ipsilateral miosis, ptosis, and anhidrosis secondary to disruption of the sympathetic innervation of the orbit and face. The degree of anhidrosis varies depending on the location of the insult. 2 This syndrome can be caused due to insults that affect any level of the complex 3 neuron arc of the oculo-sympathetic reflex. The first-order neurons originate in the dorsolateral hypothalamus and descend caudally to synapse in the cervical spinal cord C8-T4. The second order (preganglionic) neuron exits the spinal cord through the anterior horn, passes over the apex of the lungs and enters the sympathetic chain in the neck, synapsing with the superior cervical ganglion located near the bifurcation of the common carotid artery. The third-order neurons then give rise to axons that course to the orbit with the internal carotid artery through the cavernous sinus and join the first division of the trigeminal nerve to enter the orbit.
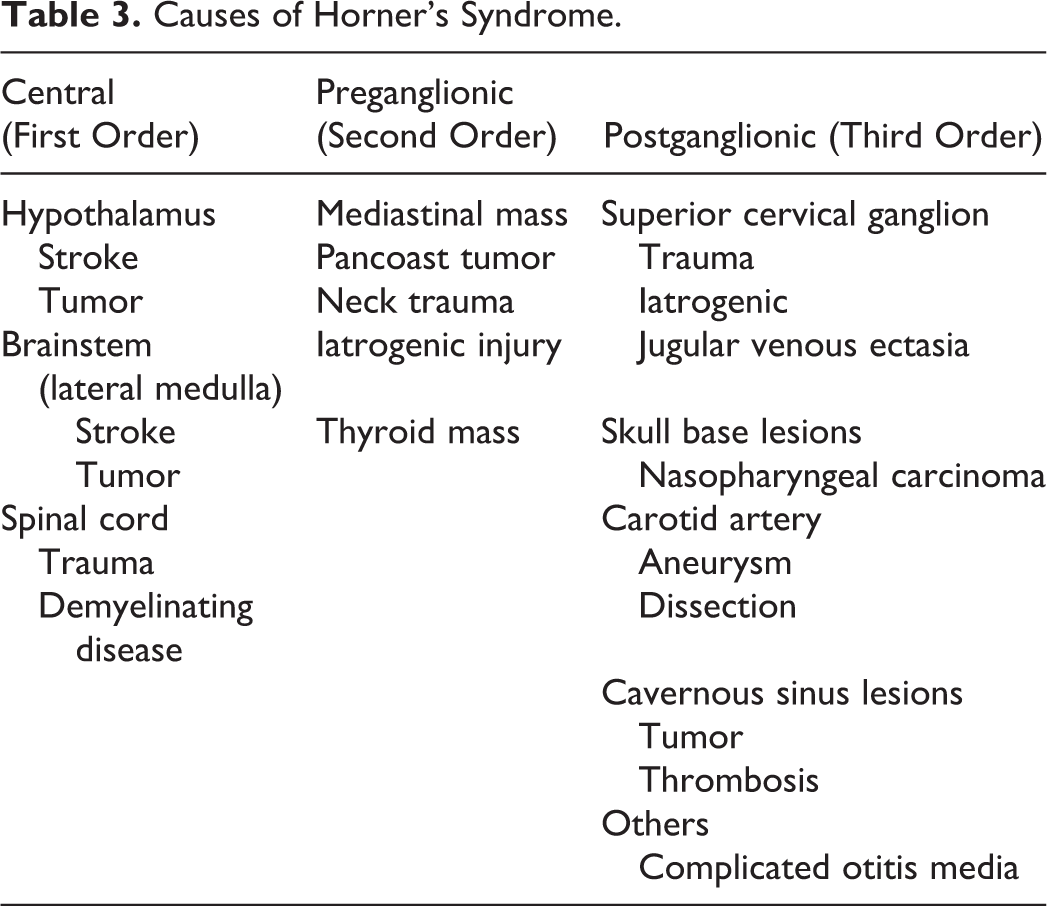
Various etiologies have been described to cause Horner syndrome (Table 3). 3,4 Tumors, trauma, iatrogenic injury during neck surgery, and internal carotid artery pathology (dissection, aneurysm) are common causes in relation to neck structures. Most of these cases result from insult to the cervical sympathetic chain.
Causes of Horner’s Syndrome.
The sympathetic trunk maintains a posteromedial relationship to the carotid sheath throughout its course in the neck. The superior cervical ganglion is most commonly at the level of the fourth cervical vertebrae. 5 Based on the review of the imaging, we hypothesize that the neurological insult in all of our patients occurred above the level of the superior cervical ganglion.
The oculosympathetic symptoms in these patients could either be a result of tumor invasion into the sympathetic chain or from compression. In the one surviving patient, we speculate that a pressure effect is the most likely cause since the Horner syndrome completely resolved after a salvage neck dissection. For the remaining cases, the mechanism cannot be differentiated with imaging. One of the most significant findings in this report is the poor prognosis associated with Horner syndrome as a result of carotid sheath involvement. None of the patients presented with symptoms related to Horner’s syndrome. This was found during examination and led to detailed evaluation of the scans to look for carotid sheath involvement. Invasion into the carotid sheath is an important factor in determining prognosis and typically represents malignancies of high stage and grade. Death occurred in 5 (83%) of 6 of our patients within 2 years of presentation. This survival is poor in comparison to the overall 5-year survival rates of 26.5% and 19.4% for stage 4 oral cavity and pharyngeal cancers and 29.9% for stage 4 laryngeal cancers, 6 and correlates to advanced disease at time of presentation.
Conclusion
This is the first case series of neck metastasis from a mucosal HNSCC as an unusual cause of Horner syndrome and generally indicates carotid sheath encasement with very poor prognosis. However, recognition of Horner syndrome in a patient with a neck mass should not be considered a sign of unresectability. A holistic approach should be used to plan further treatment.
Footnotes
Authors’ Note
This article has been presented as a poster at the Triological Society 2018 Combined Sections Meeting held at Scottsdale, AZ, USA from January 18, 2018 to January 20, 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.