
Abstract
Sinonasal adenoid cystic carcinoma is a rare malignant epithelial tumor characterized by slow growth, multiple local recurrences, and perineural invasion; surgery followed by radiotherapy provides the best overall survival by means of an endoscopic, craniofacial, or combined approach. We present a previously undescribed case of frontal sinus adenoid cystic carcinoma involving the subcutaneous tissue and the dura mater treated with an open technique, free flap reconstruction, and hadron therapy together with a summary of the state of the art.
Keywords
Introduction
Adenoid cystic carcinoma (ACC) is an uncommon malignant epithelial tumor of the upper aerodigestive tract generally characterized by a slow growth, multiple local recurrences, and perineural invasion. 1,2 Among sinonasal ACCs (SnACCs), the maxillary sinus appears to be the most frequently interested site (46%-63%), followed by the nasal cavity (20%), ethmoidal complex (10%), sphenoid sinus (5%), and nasopharynx (20%). To our knowledge, no ACC of the frontal sinus has been reported before. 3
Surgery followed by radiotherapy (RT) provides the best overall survival to patients with ACC, including the sinonasal presentation. An endoscopic, craniofacial, or combined approach is chosen preoperatively based on radiologic imaging. Concerning frontal sinus ACC, endoscopic surgery is indicated unless an infiltration of the surrounding structures is suspected or if free margins cannot be obtained. 4
Our aim is to present a case of ACC of the frontal sinus involving the subcutaneous tissue and the dura mater treated with an open technique together with a summary of the state of the art.
Case Report
A 45-year-old male, professional diver presented to our institution complaining of worsening headache. He reported a history of recurrent barotraumatic sinusitis and increasing difficulty to equalize during his job. The patient denied any chronic illness or sudden weight loss and reported a 20 pack-year smoking history. On examination, the patient appeared to be alert and oriented, he reported facial pressure, moderate nasal obstruction, and hyposmia, but no nasal discharge was noted. No signs of cranial nerves impairment or neurological deficit were observed. The nasal endoscopic examination showed a grayish mass filling the left frontal recess. Computed tomography (CT) scan revealed a solid productive lesion with inhomogeneous enhancement localized in the upper proximal sectors of the nasal bones that presented signs of advanced osteolysis. The lesion in the upper part eroded the anterior table of the frontal sinus. No signs of involvement of the orbits, the anterior ethmoid cells, or the cribriform plate of the ethmoid were observed. Magnetic resonance imaging (MRI) confirmed the presence of a solid lesion (24 × 20 × 16 mm) centered on the nasal bones, providing infiltrative osteolysis of the latter. The formation also eroded the inferior wall of the frontal sinus, in its right paramedian portion, and subsequently overflowed in the frontal sinus, where it reached a retention cyst. This additional formation seemed to act as a buffer between the solid lesion and the posterior wall of the frontal sinus. Magnetic resonance imaging also hinted at a possible infiltration of the subcutaneous soft tissues in the frontal region (Figure 1). Both open and endoscopic biopsies were performed. Histological examination reported the presence of an ACC and confirmed the subcutaneous involvement. A positron emission tomography-CT was performed, which ruled out distant metastases or lymph node involvement.

Magnetic resonance imaging (MRI) appearance of the tumor (red arrows).
Operative Procedure
The tumor was treated with an open surgical technique. The incision was made by tracing an inverted trapezoid whose base coincided with the first frontal wrinkle, the lateral sides followed the supra-lateral arches passing medially to the medial canthi, and the top corresponded to the insertion of the nasal bones on the frontal bone (Figure 2).

Drawing of the incision.
The nasal bones and the anterior table of frontal sinus appeared eroded and were removed along with the uncovered lesion. Frozen section procedure was performed on all the surgical field margins: The pathologist reported a positivity on the cribriform plate, prompting a resection of the anterior skull base. The reconstruction plan consisted of one underlay layer of fascia lata, one overlay layer of fascia lata, and the subsequent apposition of an anterolateral thigh (ALT) free flap, anastomosed with the neck vessels through a subcutaneous tunnel (Figure 3). Postoperative proton therapy was administrated.

Postoperative result.
Postoperative Course
The patient was discharged after 8 days of uneventful hospital course except for diplopia, which was successfully treated with corrective lenses. After a postoperative visit 2 weeks after discharge, the patient has been attending close outpatient follow-up every month for 1 year and then every 2 months. The patient is now in his second year of follow-up without recurrence.
Discussion
Adenoid cystic carcinoma is a rare epithelial tumor originating from mucus-secreting glands of the upper aerodigestive tract. It accounts for <2% of head and neck malignancies and can also involve the nasal cavity and paranasal sinuses, accounting for 5% to 15% of malignancies of this subdistrict. 1 Adenoid cystic carcinoma is characterized by slow growth, multiple local recurrences, and perineural invasion. 2 Despite the fact that locoregional lymph nodes are rarely interested, ACC is associated with a poor prognosis due to the high frequency of distant metastases, especially to lung, bone, and liver 5 ; furthermore, diagnosis is often made in the advanced stages of the disease. 6 No distinct risk factors, including smoke, have been identified. 5 Histologically, ACC can be categorized into 3 growth patterns, cribriform, tubular, and solid, with the latter associated with a worse prognosis. 7 Mixed patterns have also been reported: In these cases, the histological grading should be based on the percentage of solid pattern, according to Szanto et al. 6,8
Recent studies have shown that c-Kit mutations are associated with a poorer prognosis, while Epidermal growth factor receptor expression appears to be associated with a better survival. 9 Presence of c-Kit mutations may also be useful to distinguish true ACC from adenocarcinomas. 6
Sinonasal ACC
Among SnACCs, the maxillary sinus appears to be the most frequently interested site (46%-63%), followed by the nasal cavity (20%), ethmoidal complex (10%), sphenoid sinus (5%), and nasopharynx (20%). 3 Sinonasal ACC is usually paucisymptomatic, more commonly with nasal obstruction or pain as presenting symptoms. Sinonasal ACC locally invades by destruction of adjacent bone, submucosal infiltration, and/or through perineural/perivascular spread, with diffusion to the skull base and the cavernous sinus. 1
Sinonasal ACCs is associated with an increased incidence of local recurrence compared to other head and neck sites and poor long-term survival rates due to the development of distant metastases. The 5-year survival rates range from 17% to 53%, with local recurrence occurring in 50%, regional recurrence in 20%, and distant metastasis in 30%. Perineural invasion is a hallmark of this tumor but does not correlate with local control for sinonasal disease. 10
Michel et al reported their 13 years’ experience of 25 cases of ACC of the paranasal sinuses, and 72% of those had a clinical staging at diagnosis of T3-T4. American joint committee on cancer only includes maxillary and ethmoid sinus as a possible paranasal origin of a primary carcinoma. Frontal sinus involvement is implied to be a sign of advanced disease from the nasal cavity and the ethmoid and maxillary sinuses; therefore, the staging is immediately upscaled to T4a. 11 Since the mass jutted into the nasal cavity just above the frontal recess, and all the endoscopic biopsies turned out to be negative, we can assume that our case originated most likely from the frontal sinus mucosa.
Frontal Sinus Malignancies and Frontal Sinus ACC
Primary malignancies originating in the frontal sinus are rare, accounting for approximately 1% of cases of sinonasal malignancies; squamous cell carcinoma remains the leading cause; however, cases of melanoma, adenocarcinoma, sarcoma, lymphoma, and carcinoid tumors have been historically reported. 12 Presentation symptoms of all sinonasal tumors are usually aspecific and may mimic an inflammatory disease; facial pain, epistaxis, nasal obstruction, swelling, and visual disturbances may be overlooked, delaying the diagnostic workup. Our patient experienced pain in the frontal region as the chief symptom, in line with larger case series in previous works 1,6 ; early diagnosis was largely due to his diving habits, which exacerbated the symptomatology. Bhojwani et al reported a case series from the Surveillance, Epidemiolog and End Results 18 database from 1973 to 2012; the group isolated 171 patients, accounting for 28% of the registry grouping. Results of data analysis showed a male Odds ratio of 1.59, no race predilection, and peak age between 60 and 69 years of age; the most common histological type of cancer was Squamous Cell Carcinoma, followed by mature B-cell Non-Hodgkin Lymphoma, epithelial neoplasms not otherwise specified (NOS), and adenocarcinomas. It is worth noting that, while no ACC or minor salivary gland tumor case was described, the NOS carcinomas might include those histotypes. 12 Adenoid cystic carcinoma is described by Gourin and Terris as a possible malignancy arising from the paranasal sinuses even when talking exquisitely about the frontal sinus, but the latter is not considered or reported as a possible site of origin. 10
TNM and Staging
Because of the inherent rarity of the disease and the subsequent scarcity of published works (mostly case reports and small institutional studies), prognostic implications of these malignant neoplasms are difficult to deduce, and a widely accepted tumor classification specific to the frontal sinus still does not exist. 13 Frontal sinus lesions are not included in the American Joint Committee on Cancer staging system; in the National Comprehensive Cancer Network , guidelines are not meant as a standalone entity rather only as a spread site from the other sinuses, immediately upscaling the stage to T4a. The University of Florida staging system is the most commonly used staging system for frontal sinus malignancies (Figure 4). Our case should be classified as stage III because of the intracranic diffusion (dura mater infiltration).
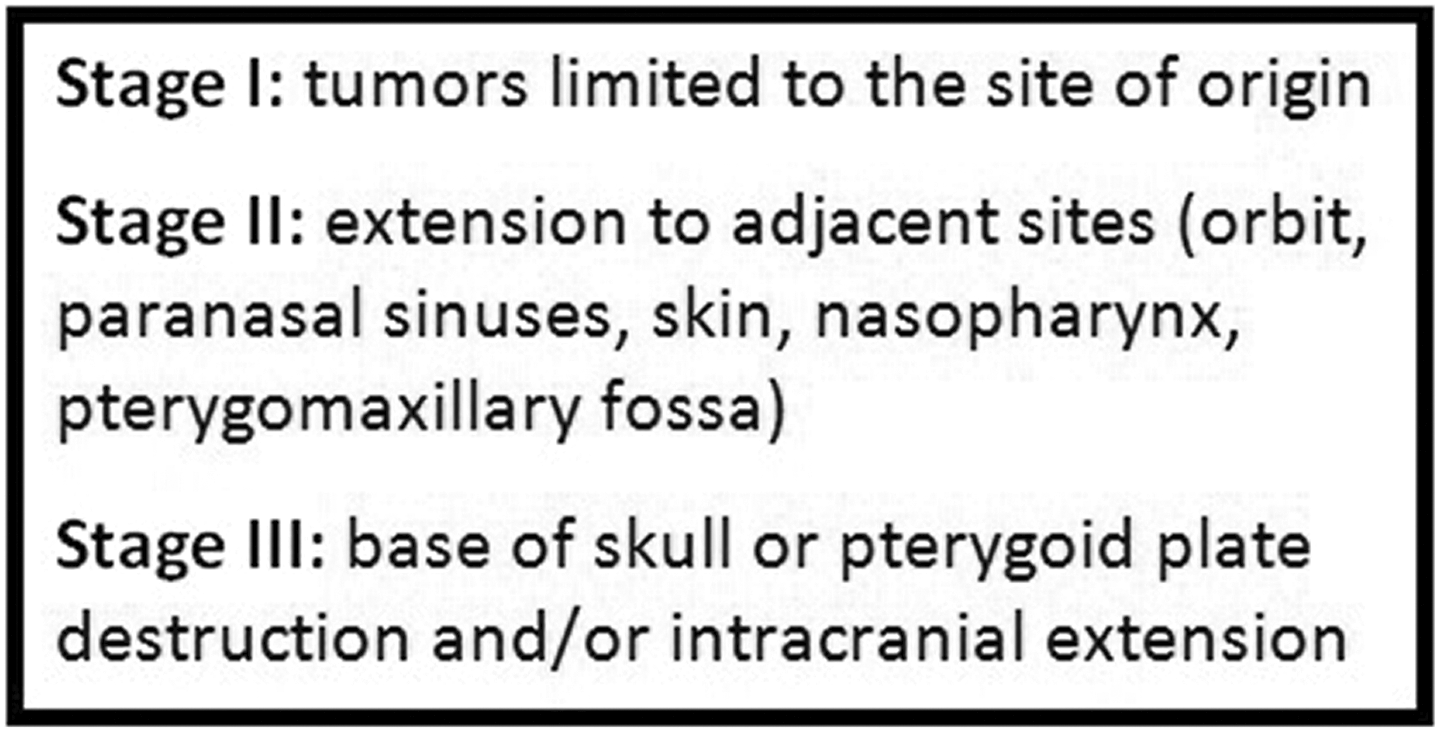
The University of Florida staging for frontal sinus malignancies.
Treatment
Surgery followed by RT provides the best overall survival to patients with ACC, including the sinonasal presentation; RT with a curative intent or gamma-knife radiosurgery is reserved for untreatable lesions. 1,14 An endoscopic, craniofacial, or combined approach is chosen preoperatively based on radiologic imaging.
Since its inception in the 1960s, the craniofacial resection (CFR) has been the mainstay of anterior skull base surgery for sinonasal malignancies. In a retrospective review by the International collaborative study group, patients treated with CFR had overall, disease-specific as well as recurrence-free survival rates between 45.8% and 53.3%. Histology, margins status, and intracranial extent all appeared to be independent prognostic predictors; although patients with ACC showed the best overall survival during the 5-year observation time, this was likely biased by its very late recurrence tendency. 15 Craniofacial resection is marred by significant postoperative complications (32.9%) and mortality rates (4.5%), which are more likely to happen after larger resections and when multiple skull base sites are involved. 16
The advent of endoscopic surgery has restricted CFR indications, ensuring a lower morbidity with comparable oncologic outcomes. 2 Concerning frontal sinus cancer, endoscopic surgery is advised when the medial portion is involved, while CFR or a combined approach is indicated in case of infiltration of the anterior or lateral wall, orbit content, nasal bones, soft tissues, skin, massive infiltration of the dura over the orbital roof or brain parenchyma, or when free margins cannot be achieved. 4 Thus, CT-scan and MRI must investigate disease extension and relationship with major vessels; 4 although we performed both examinations in our case, early involvement of adjacent sites, such as the orbit, the cribriform plate and the dura, proved to be hard to evaluate. Because of the inherent difficulty of preoperative assessment, and the known tendency to local and neural invasion, frozen section procedure should always be performed as previously stated by Ramakrishna et al. 17
Craniofacial resection is a modular procedure depending on the subsites involved by the lesion as described by Cheesman et al; while craniotomy is usually performed with a bicoronal skull resection led anteriorly to the coronal suture, subfrontal approach is a valid alternative when the resection should include the superior orbit, glabella, nasal root, and nasal bones. 18,19 Orbital exenteration is indicated in case of orbital involvement, such as the infiltration of the intraconal fat, extraconal muscles, globe, and orbital apex. 20 While our patient’s eye was spared, a transfacial exposure of the nasal bones, nasal cavity, and the ethmoid was deemed necessary.
Reconstruction
The first aim of cranial reconstruction after CFR is to seal the dura, in order to prevent cerebrospinal fluid leak and meningitis; large dural defects often require patches provided by fascia lata, temporal fascia, or dural substitutes. Anterior cranial fossa floor gaps are best repaired with a pedicle pericranium flap; free bone flap placement is not only unnecessary, but it can also increase the risk of osteoradionecrosis when adjuvant RT is required. 21 Sinus cranialization is mandatory to prevent mucocele formation; accurate demucosalization of the frontal sinus and nasofrontal ducts must be performed, followed by fat or free muscle obliteration of the resulting dead space. 22 Concerning the skin, cutaneous defects up to 2 cm can be closed with a forehead-brow rotation advancement flap; eyelid defects up to 1 cm can be repaired with a tarsal advancement; when the gap is bigger, the surgeon can resort to a scalp rotation flap or a free flap, such as the radial forearm free flap. 23 Our team opted for a ALT free flap, a rarely cited solution that grants of a considerable amount of cutaneous and muscular tissue with low donor site morbidity.
Radiotherapy
As previously stated, exclusive RT is reserved only for surgically infeasible sinonasal malignancies 10 : This is true for SnACC too, as RT alone shows worse results compared to surgery or combined approach. Due to high risk of local invasion, adjuvant RT is advised in SnACC, especially when skull base invasion is present; however, its efficacy on local recurrence and long-term prognosis is yet to be proven. 24 Due to the rarity of ACC and the scarcity of available hadron therapy centers, most of the data on ACCs treated with this therapeutic modality is published within heterogeneous groups. Besides, since the prognosis of ACC is mainly defined by local control, it is legitimate to assume that hadron therapy could play a role in increasing survival. However, randomized studies comparing hadron therapy with other forms of RT in the ACCs have not yet been conducted. 11 In our case, its usage was deemed beneficial when considering the recurrence-free survival and the absence of adverse events.
Conclusions
Frontal sinus ACC is an ill-described entity in the literature, and in that regard the TNM staging system is severely lacking; surgical planning must take into account any possible involvement of the adjacent sites and the anterior skull base, even with a negative imaging. Therefore, intraoperative consultation with the pathologist using frozen section procedure is mandatory in order to guide the resection. Hadron therapy might be a valid postoperative aid for local control, considering the neighboring noble structures. Reconstructive flaps may be necessary, and therefore the surgical team must have this expertise when facing a highly demolitive CFR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.