
Abstract

Keywords
Secondary cleft lip deformities are common. Over time, primary surgical correction of a cleft lip can become distorted resulting in suboptimal long-term functional outcomes in areas such as feeding, speech, and breathing as well as negative psychosocial consequences including negative peer interactions and social isolation. For these reasons, it is imperative to perform secondary revision surgery to ensure proper functional and social development. 1
Reconstruction of secondary cleft lip deformities continues to be a challenge in plastic surgery. The Abbé flap has proven very versatile for the reconstruction of severe secondary cleft lip deformities. The original procedure designed by Abbe involved a flap based on the labial branches of facial artery with complete philtral reconstruction. 2
A 12-year-old Hispanic female with a history of bilateral cleft lip and palate presented with a secondary cleft lip deformity. The patient underwent repair of her cleft lip and palate at 8 months and 3 years of age, respectively. Subsequently, the patient developed a secondary lip deformity which was a centralized scar contracture of the upper lip with missing philtral elements (Figure 1). Her past medical history was significant for other midline defects including holoprosencephaly and hypopituitarism. Therefore, the decision was made to perform an Abbé flap to correct the deformity.

Preoperative photo of the patient with a secondary cleft lip deformity, characterized by a centralized scar contracture of the upper lip with missing philtral elements.
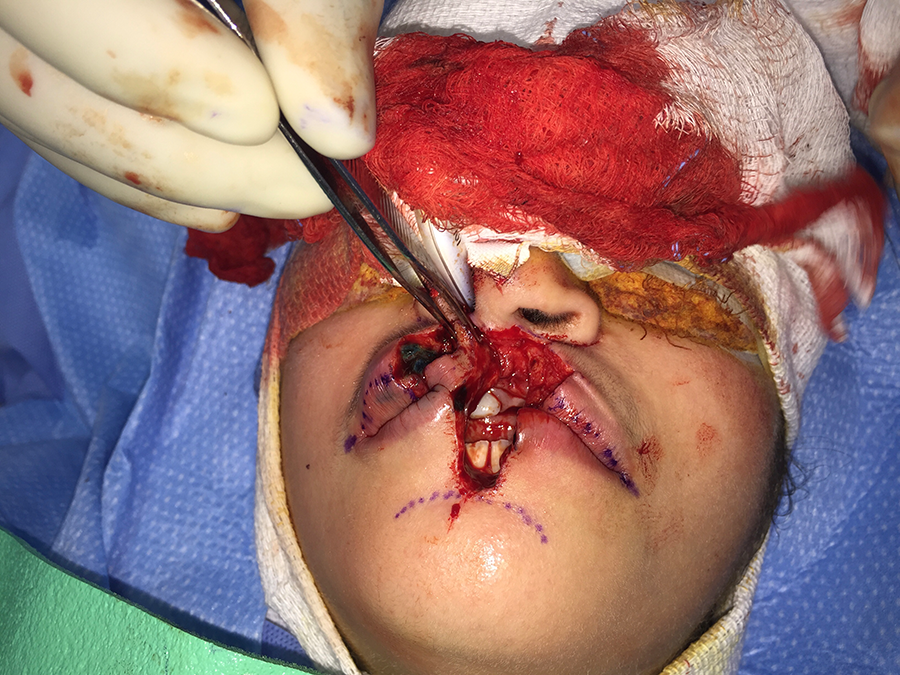
First, a philtral-shaped flap was marked out on the lower lip. Markings were then made for the planned excision and creation of the defect and scar excision on the upper lip that extended around the base of the nose. New lateral advancement flaps were marked for the pairing of the scar along the vermillion bilaterally (Figure 2). A scalpel was used to recreate the defect around the alar base, the centralized scar was excised and the orbicularis muscle was then identified laterally on both sides of the upper lip. After recreation of the defect, a buccal sulcus incision was made to allow for advancement of the lips to the midline bilaterally.

Abbe flap marked out for the planned excision.
After creation of the defect, attention was then directed at harvesting a lower lip flap, which was based centrally and a distal extent was just above the menton. This was accomplished by developing a full-thickness skin, muscle, and mucosal flap on the lower lip (Figure 3). A 4-0 Vicryl suture was placed to inset the philtral segment into the defect centrally. The inferior labial artery was identified upon division of the left side of the flap. It was left intact on the right side and adequate dissection was made to allow positioning of the flap into the defect, but with preservation of the arterial blood supply.
Harvest of a full-thickness skin, muscle, and mucosal flap on the lower lip.
A 4-0 Vicryl suture was placed to tack the Abbé flap centrally at the base of the nose. The lower lip defect was closed in layers with 5-0 Monocryl for the mucosal layer, 4-0 PDS for the muscle, and 4-0 Vicryl for the skin. Reconstruction of the upper lip was then closed in the same fashion. The flap was carefully positioned and shaped to the size of the defect for symmetry of the upper lip. A segment of the flap was left intact and there was a small opening at the base of the connection between the upper and lower lip. The 5-0 chromic sutures were placed in the skin as needed for approximation. Dermabond was applied to the upper and lower lip. Throughout the procedure, there was good vascularity of the flap. Five days postoperatively, the sutures were removed and the pedicle was noted to be viable.
Two weeks later, the patient was brought back to the operating room for the second-stage pedicle division. After the pedicle was divided, both lips were undermined, debulked, and closed with 5-0 Monocryl sutures. Postoperatively, the patient had aesthetically pleasing, well-healing upper and lower lips with clear philtral columns, Cupid’s bow, and vermillion border was present (Figure 4). The lips had adequate blood supply and there were no signs of infection. All photos depicted in this manuscript were used with verbal permission from the legal guardian of the patient.

Postoperative photo of the patient demonstrating aesthetically pleasing, well-healing upper and lower lips with clear philtral columns, Cupid’s bow, and vermillion border present.
The Abbé flap is a cross-lip, full-thickness composite flap involving the transfer of the skin, muscle, and mucosa of the central portion of the lower lip to the upper lip. Severe lip deformities, especially those involving the philtrum, can be repaired successfully with the Abbé flap. 3 Specifically, the Abbé flap can be helpful with a tight upper lip, deficiency or scarring of the central part of the upper lip, thinness, and color mismatch of the vermilion with a nonexistent lip tuberculum, whistle deformity or the absence of a Cupid’s bow. 3 –6
Although the Abbé flap can be a viable option for lip reconstruction, it can come with complications and undesirable results. These include wound infection, bleeding, flap necrosis, and unfavorable scarring including philtral dimpling or ridging. In addition, the lip is immobilized which can create patient discomfort and breathing difficulties with closed lips prior to the division of the pedicle. 3,4,7,8 The staged nature of this procedure necessitates multiple surgeries. 3
The Abbé flap is a reliable reconstructive option for managing secondary cleft lip deformities in both adults and children. In particular, this flap reconstructs philtral landmarks, reconstitutes oral competence of the orbicularis and recreates Cupid’s bow and the central pout.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.