
Abstract
Case Description
A 60-year-old male was transferred to University of Illinois Health Services for further evaluation and management of stridor and dyspnea. He had been followed by his primary care provider and pulmonologist, but deteriorated clinically. He smoked 5 cigars annually and denied any illicit drug use, alcohol use, or occupational exposure to inhaled carcinogens. He had no history of asthma, allergies, or respiratory disorders, but he had been treated for gastroesophagela reflux disease and hypertension.
Physical examination was notable for fixed, expiratory, nonpositional stridor, and mild respiratory distress. Computerized tomography with contrast of the neck showed a contrast-enhancing, midline 2.7 × 2.1 × 3.5 cm endotracheal soft tissue mass causing greater than 90% obstruction of the tracheal lumen. It did not span to adjacent structures. No associated lymphadenopathy was noted.
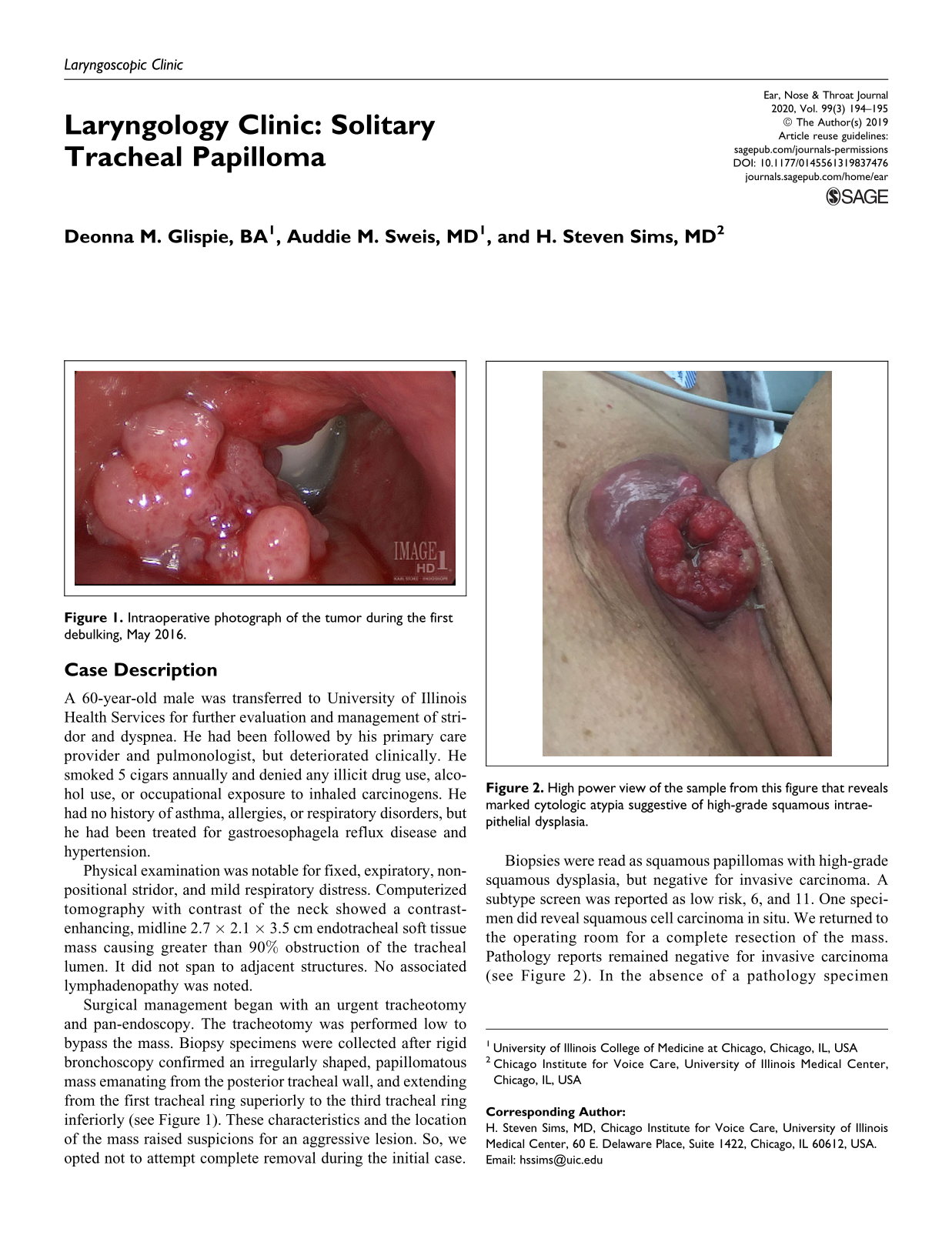
Surgical management began with an urgent tracheotomy and pan-endoscopy. The tracheotomy was performed low to bypass the mass. Biopsy specimens were collected after rigid bronchoscopy confirmed an irregularly shaped, papillomatous mass emanating from the posterior tracheal wall, and extending from the first tracheal ring superiorly to the third tracheal ring inferiorly (see Figure 1). These characteristics and the location of the mass raised suspicions for an aggressive lesion. So, we opted not to attempt complete removal during the initial case.
Intraoperative photograph of the tumor during the first debulking, May 2016.
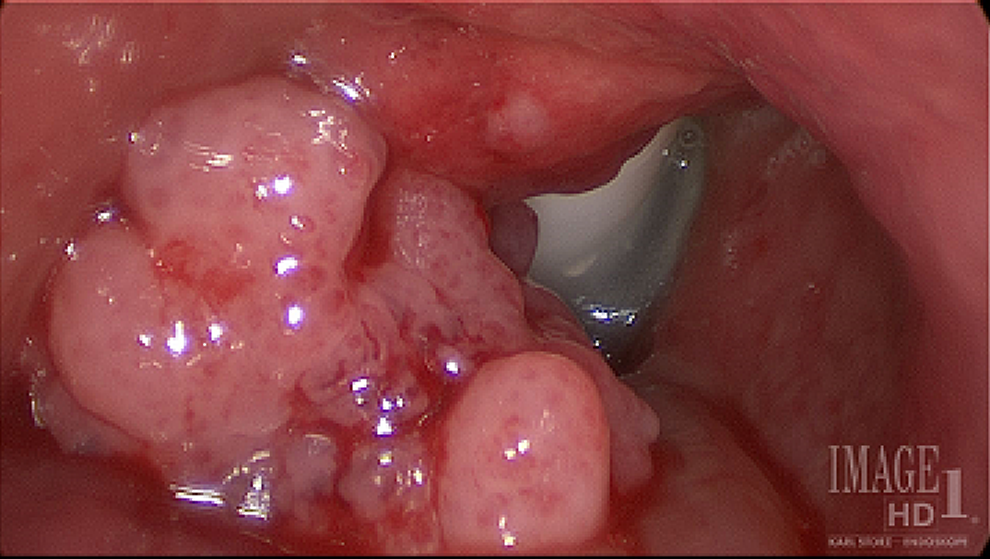
Biopsies were read as squamous papillomas with high-grade squamous dysplasia, but negative for invasive carcinoma. A subtype screen was reported as low risk, 6, and 11. One specimen did reveal squamous cell carcinoma in situ. We returned to the operating room for a complete resection of the mass. Pathology reports remained negative for invasive carcinoma (see Figure 2). In the absence of a pathology specimen confirming invasive squamous cell carcinoma, the patient was decannulated.

High power view of the sample from this figure that reveals marked cytologic atypia suggestive of high-grade squamous intraepithelial dysplasia.
Three months later, we removed recurrent papillomas obstructing 75% of the lumen. Two months after that the patient complained of soft tissue swelling near his tracheotomy scar. In-office excisional biopsy of the neck mass confirmed an intradermal papilloma with a high-grade squamous intraepithelial lesion. Suspicion for transformation remained high. We referred the patient to the head and neck surgical oncology service where he underwent additional biopsies which were all negative for malignancy.
The patient returned with a mass in the anterior neck that was “coming through the skin” (Figure 3). Wide surgical excision was performed, and the final pathology report ultimately confirmed the long-held suspicion for invasive squamous cell carcinoma with only HPV type 6 identified.
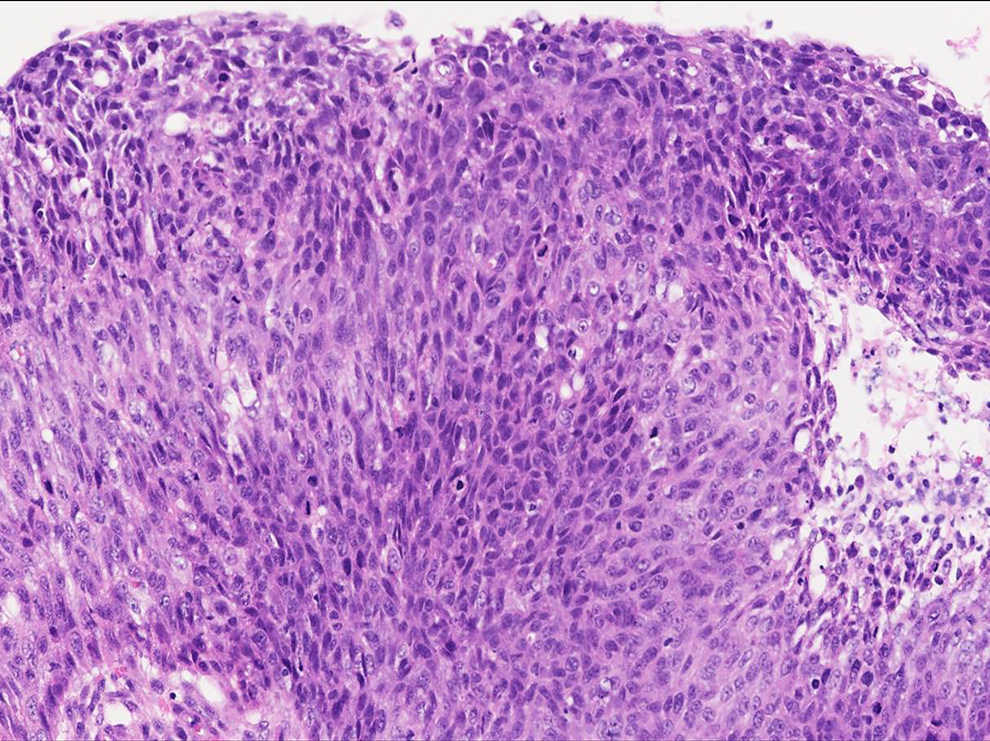
Preoperative view of dermal lesion/invasive squamous cell carcinoma.
Often the diagnosis of tracheal tumors is delayed because of their slow-growing nature and nonspecific symptoms. Gaissert et al demonstrated that the mean duration of symptoms prior to diagnosis is 12.2 months. 1 Delay of diagnosis can be greater than 20 months from initial onset of symptoms. 2 Clinicians often treat presumed asthma, COPD, and pneumonia first. If the tumor has invaded surrounding structures, symptoms such as dysphagia and hoarseness also may be noted. 2 This patient’s tracheal mass was determined to be squamous papilloma. However, his disease recurred quickly and progressed to SCCA in only a few months.
Recurrent respiratory papillomatosis (RRP) is commonly attributed to persistent infection of the respiratory mucosal epithelium by low-risk strains HPV 6 or 11. HPV-11 positive RRP tends to present with a more aggressive clinical course, but progression is often slow. 3,4 HPV 11 RRP is also more commonly associated with extralaryngeal spread of the disease as compared with HPV 6 RRP. 3,4 Still, the overall risk of RRP malignant transformation is only 3% to 7%. 4
We report this exceptional case to raise awareness on the signs and symptoms associated with isolated tracheal masses as well as the unique intradermal involvement and progression to invasive squamous cell carcinoma. It is common to have a patient present with nonspecific signs and symptoms associated with isolated tracheal masses. The RRP should be included in the differential diagnosis. For isolated tracheal RRP progressing to cancer with dermal involvement, literature is scarce regarding optimal medical and surgical management. We recommend remaining vigilant and highly suspicious of a malignancy for rapidly recurring, locally extensive lesions. This is important even if pathology specimens do not confirm serious disease and even if the HPV isolated from the specimen is considered low risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.