
Abstract
The study objective was to assess if the extent of neck dissection among patients who receive adjuvant radiotherapy affects regional recurrence and survival. This was a retrospective study of patients who had clinical metastatic mucosal primary squamous cell carcinoma (SCC) to cervical lymph nodes done at Roswell Park Comprehensive Cancer Center, Buffalo, New York from 2004 to 2015. Patients with previous radiotherapy and/or chemotherapy were excluded. All patients had surgery to the primary tumor and the neck followed by adjuvant (chemo) radiation. Patients have been divided into 2 groups according to type of neck dissection as either selective neck dissection (SND) or comprehensive neck dissection (CND). The extent of neck dissection was determined by surgeon preference. All patients received postoperative radiotherapy to the primary tumor bed and to the neck with or without chemotherapy. Main outcomes were measured in regional recurrence and overall survival. In our study, 74 patients were included. Among the 2 groups of patients, 3-year outcomes for regional recurrence occurred in 4 (7.1%) of 56 patients in the SND group and 2 (11.1%) of 18 patients in the CND group. Overall survival was 29 (51.8%) of 56 patients in the SND group and 11 (61.1%) of 18 patients in the CND group (P = .497). Among patients who died in each cohort, disease-specific death was 20 (74.1%) of 27 patients in the SND group and 5 (71.4%) of 7 patients in the CND group (P = .79).The overall and disease-specific survival differences between the SND and CND cohorts were not statistically significant. In conclusion, SND, combined with proper adjuvant treatment, achieved regional control and survival rates comparable to CND.
Keywords
Introduction
Cervical metastasis in head and neck squamous cell carcinoma (HNSCC) is an important prognostic factor. Thus, adequate treatment of neck disease is crucial in achieving the best survival outcomes. When multimodality treatment of the neck is needed, the extent of neck surgery is controversial. One approach for surgical management for node-positive disease involves comprehensive neck dissection (CND; levels I-V). 1 -6 At our institution, we have moved away from CND when the patient will also get adjuvant (chemo) radiation. Instead, a therapeutic selective neck dissection (SND) is done.
Application of neck dissection in control of regional disease in patients with SCC of the upper aerodigestive tract has evolved considerably over the past 3 decades. Since radical neck dissection was first described by Crile in 1906 and popularized by Martin in 1951, 7 it has served as the gold standard for surgical management of regional disease in the neck until the last third of the 20th century. Because RND often results in high morbidities, such as neck deformities and impairment of shoulder function, modifications have been devised in order to improve the functional outcome while preserving oncological efficacy. This led to the use of the modified radical neck dissection. 7,8
The use of SND in patients with clinically node-negative disease has been associated with improved functional outcome. SND is widely used and accepted for staging cases of SCC of the upper aerodigestive tract that are clinically node-negative. However, approximately 10% to 40% of patients who underwent SND were found to harbor occult disease. 9 -13 In these patients with clinically negative neck and occult disease, the use of postoperative irradiation after SND affords results similar to those obtained with RND. 14,15 However, the use of SND as part of the treatment for clinically node-positive necks remains controversial. The purpose of this article was to determine whether SND versus CND in clinically node-positive patients at a single institution gives equivalent survival and recurrence outcomes when followed by adjuvant treatment.
Methods
We performed a retrospective chart review study on patients who underwent neck dissection for mucosal primary head and neck HNSCC followed by postoperative adjuvant (Chemo) radiotherapy (RT) at Roswell Park Comprehensive Cancer Center, Buffalo, New York, from 2004 to 2015. Patients who had prior RT or chemotherapy were excluded from the study. Of all, 74 patients met these selection criteria.
The decision to give adjuvant radiation or chemoradiation was given based on the NCCN guidelines. All patients under the age of 70 who had extracapsular extension or positive surgical margins were recommended to have adjuvant chemoradiation. Patients with T3 or T4 disease were considered for chemoradiation. 16 Patients who did not have these factors but had 2 or more positive lymph nodes, perineural invasion, or a single lymph node with lymph-vascular space invasion were offered adjuvant radiation alone. The total radiation dose, delivered in 2 Gy fractions, was 60 Gy for radiation alone and 66 Gy for chemoradiation.
The major variables examined were age, sex, smoking status, alcohol use, tumor stage, and chemotherapy after surgery. Neck dissection was classified as selective (fewer than 5 levels) or comprehensive (levels I-V).
The endpoints evaluated included time to recurrence (using date of surgery and date of first recurrence) and survival (using date of surgery until the date of last contact or death). All patients were followed up for recurrence and survival. Clinical characteristics were compared between those with selective and CND using the χ2 test/Fisher exact tests for categorical responses, and the t test/Wilcoxon/Kruskal-Wallis Tests for continuous variables. The OS/DSS were estimated by the Kaplan-Meier method. The association between neck dissection type and each outcome (ie, DSS and OS) were evaluated with Cox proportional hazards analysis. The SAS version 9.4 (SAS Institute, Cary, North Carolina) was used for statistical analyses. All tests were 2 sided and performed at a nominal significance level of .05.
Results
Descriptive characteristics of patients divided by neck dissection type (Table 1) were summarized. The groups of patients receiving SND and CND were similar in terms of age, sex, smoking status, and alcohol use. Postoperative chemotherapy was given in 41 (73.2%) of 56 patients who underwent SND and in 15 (83.3%) of 18 patients who underwent CND (P = .53).
Demographics and Characteristics of Patients by Neck Dissection Type.
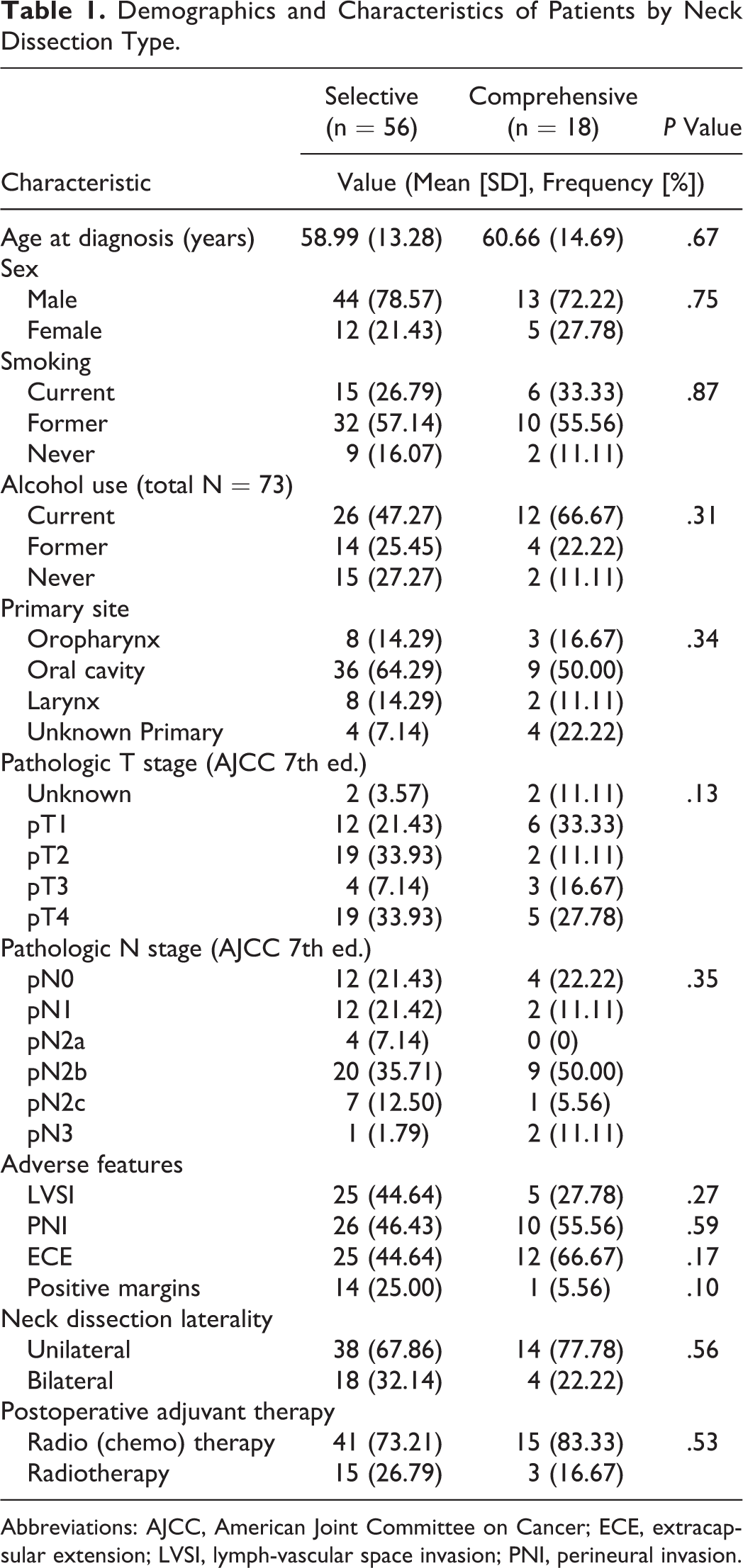
Abbreviations: AJCC, American Joint Committee on Cancer; ECE, extracapsular extension; LVSI, lymph-vascular space invasion; PNI, perineural invasion.
Median time to regional recurrence (months, n = 6) was 6.4 (range 3.9-8.5) months for the SND group and 5.4 (range 5.1-5.7) months for the CND group (P = .57). Overall regional recurrence at 3 years was encountered in 6 (8.1%) of 74 patients. Among those patients, 4 (7.1%) of 56 had recurrences after SND versus 2 (11.1%) of 18 who underwent CND (P = .63). Median overall survival time was undefined for the SND group versus 7.4 years for the CND group (P = .45). Overall survival at 3 years was 29 (51.8%) of 56 patients in the SND group and 11 (61.1%) of 18 patients in the CND group (P = .497). Thirty-four (46%) of the 74 patients expired. Among the 34 deaths, 20 (74.1%) patients in the SND group and 5 (71.4%) patients in the CND were disease-related, and 7 (25.9%) patients in the SND and 2 (28.6) patients in the CND were not.
Statistical analysis at the 3-year time point, with SND as reference (Table 2), showed an overall survival hazard ratio of 0.80 for CND (0.35, 2.00, P = .63) and disease-specific survival hazard ratio of 0.73 for CND (0.31, 1.68, P = .45) for model 1 adjusted for age and smoking status. Similarly, model 2, analysis adjusted for age, stage and smoking status, gave hazard ratios of 0.98 (0.33, 2.87, P = .96), and 0.98 (0.38, 2.50, P = .96). Thus, both models indicate the absence of statistically significant differences between these SND and CND cohorts for both overall survival and disease specific survival. Figures 1 and 2 demonstrate Kaplan-Meier curves for SND versus CND for overall survival and disease-specific survival, respectively.
Cox Proportional Hazard Models of Comprehensive Versus Selective Neck Dissection Patients.
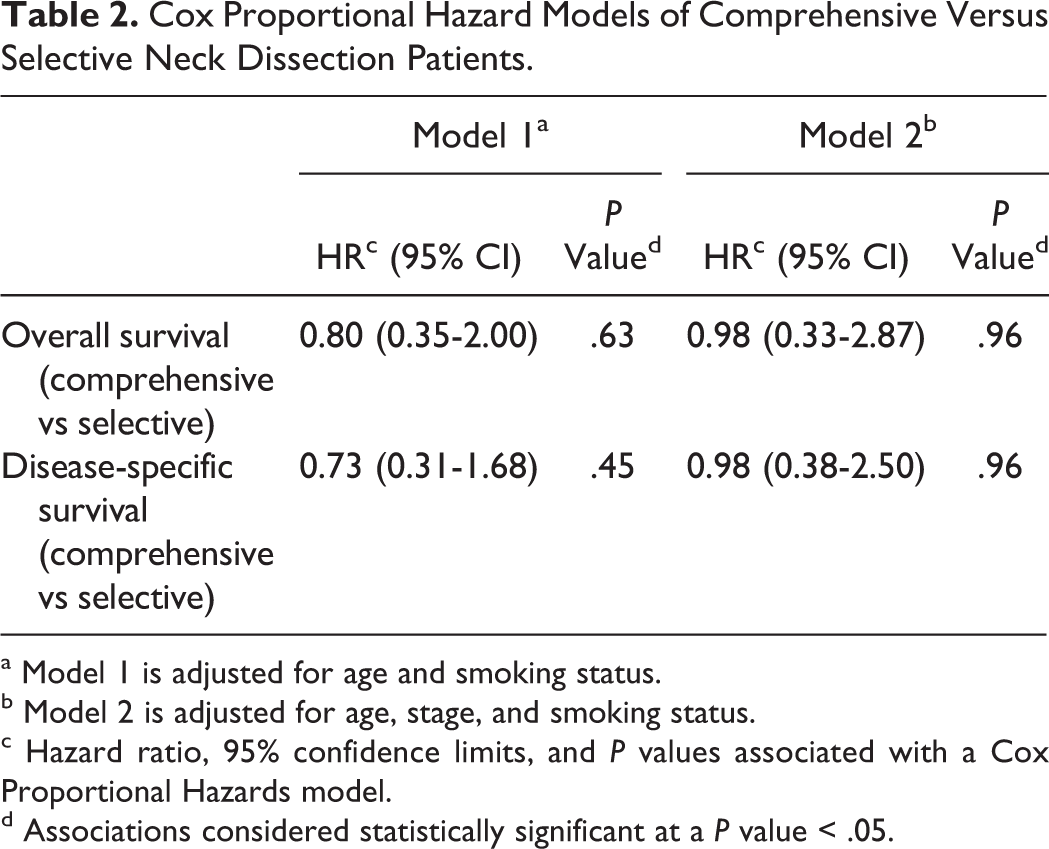
a Model 1 is adjusted for age and smoking status.
b Model 2 is adjusted for age, stage, and smoking status.
c Hazard ratio, 95% confidence limits, and P values associated with a Cox Proportional Hazards model.
d Associations considered statistically significant at a P value < .05.
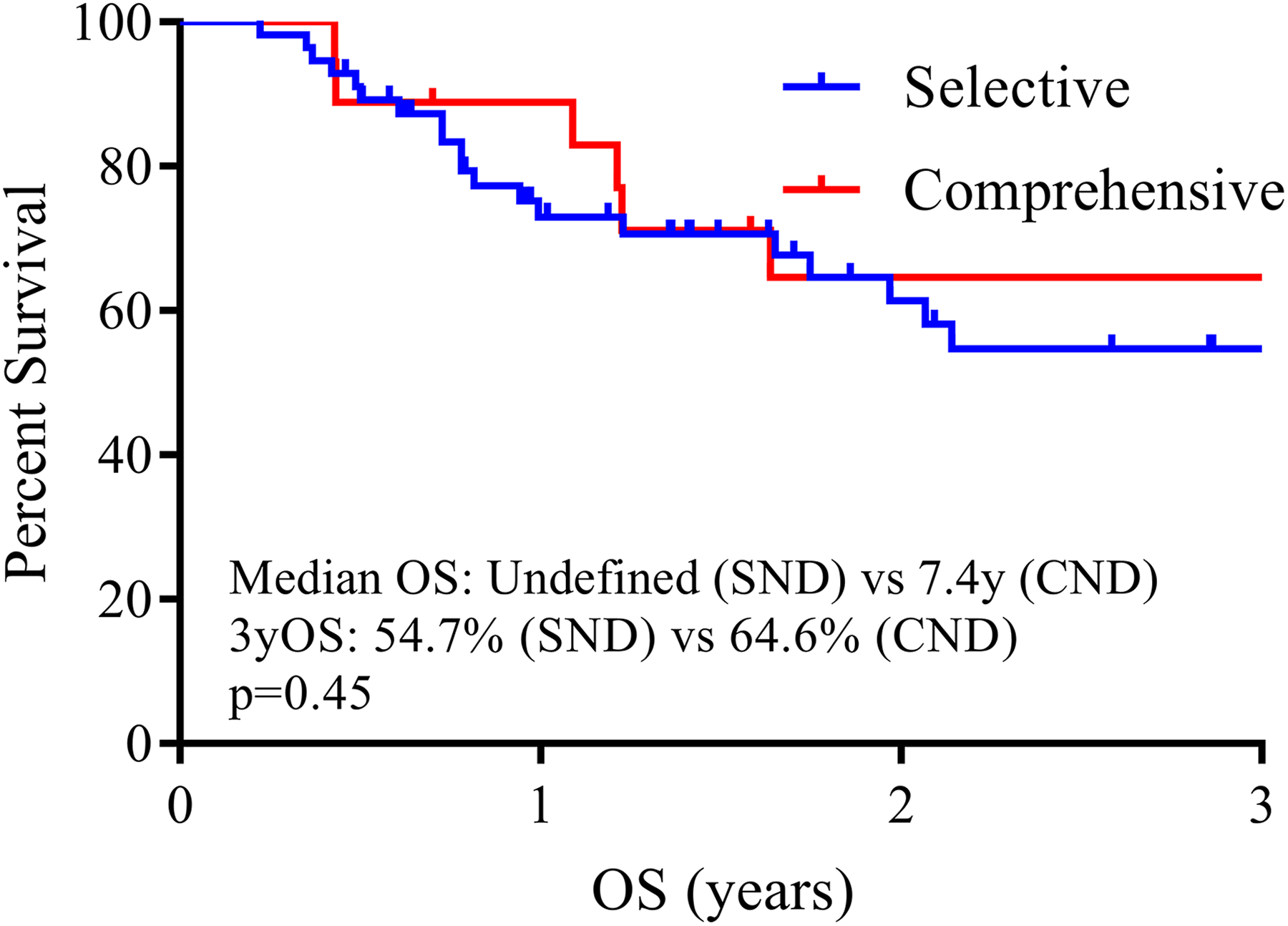
Kaplan Meier curve for overall survival of patients with selective versus comprehensive neck dissection.
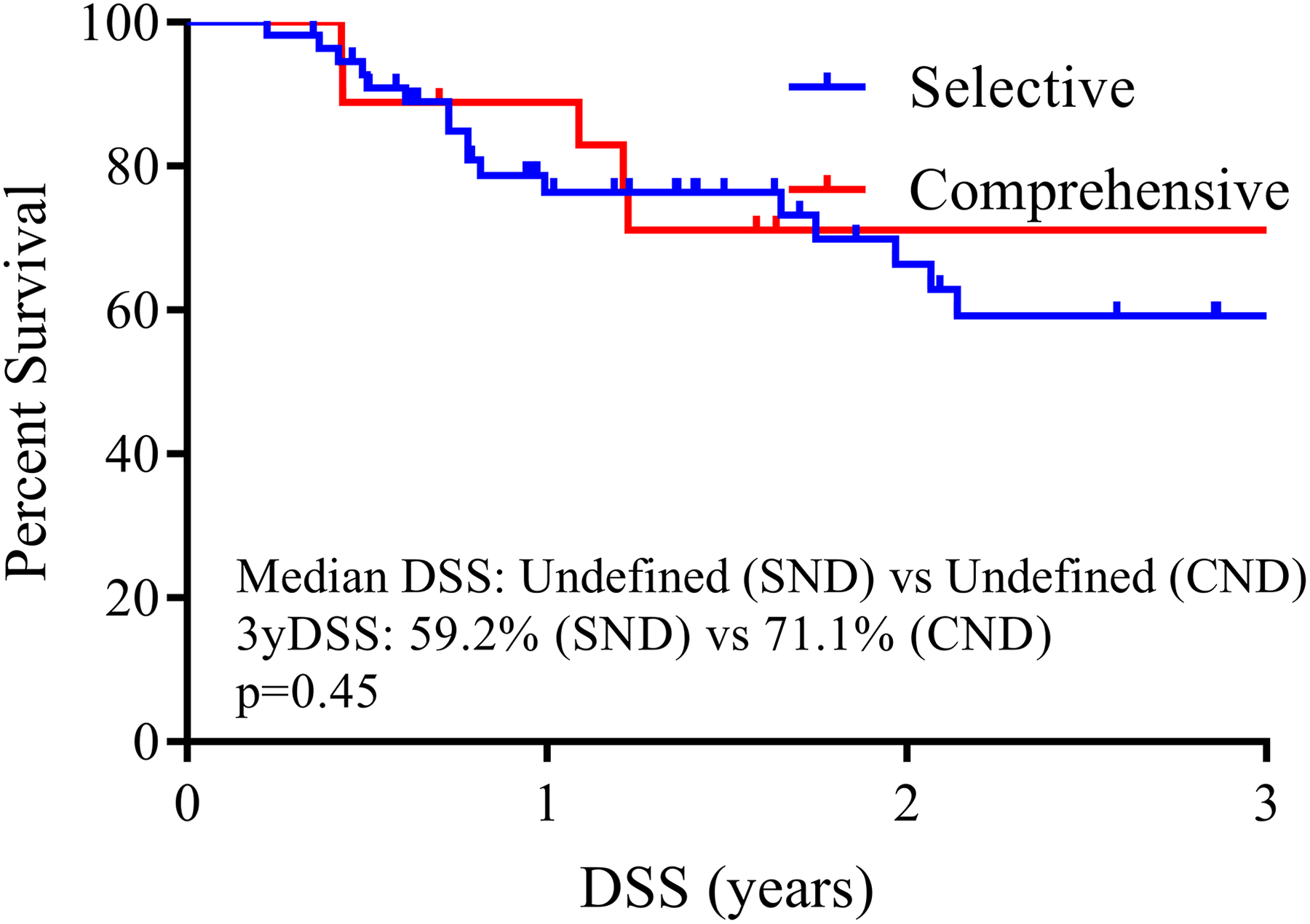
Kaplan Meier curve for disease-specific survival of patients with selective versus comprehensive neck dissection.
Discussion
Classic teaching dictates that when a patient has node-positive disease, the surgery of choice is CND. However, SND offers several advantages over CND. By not removing non-nodal/fatty structures, the morbidity of the procedure can be reduced. This includes postoperative shoulder pain and dysfunction, cosmetic deformity, and neck numbness. 17 -20 Despite the sternocleidomastoid muscle and CN XI being spared in a CND, the spinal accessory nerve can be damaged leading to shoulder dysfunction. Another benefit to SND is it requires less operative time and may lead to faster recovery and less surgical drainage output. The use of SND as sole treatment for node-positive disease has been shown to result in high rates of neck recurrence. 4,15 Other authors have shown excellent regional control rates when postoperative radiation is added. 21 -29 Our study is not the first to look at the effectiveness of SND in node-positive patients receiving adjuvant treatment, though it is one of the few that compares it to CND at the same institution.
In our study, the overall regional recurrence at 3 years was 7.1% in patients who underwent SND versus 11.1% in whom who underwent CND. Overall survival at 3 years was 51.8% in the group of patients who underwent SND versus 61.1% in the group of patients who underwent CND. There was no significant statistical difference between the SND and CND groups. This suggests the extent of neck dissection did not influence recurrence or survival outcome.
To determine results of SND in management of the node-positive neck, other studies have been done and supported this conclusion. Chepeha et al 21 did a retrospective review of 52 patients who had been treated with SND for HNSCC. Of those, 26 had positive neck nodes before surgery and went on to get adjuvant radiation. After a 2 year follow-up, the regional control rate was 94%.
To determine the oncologic efficacy of SND in patients with node-positive HNSCC, Andersen et al 22 did a 10-year retrospective single cohort chart review on 106 previously untreated patients who were clinically and pathologically node-positive and underwent SND for HNSCC. Patients who had extracapsular extension or multiple nodes positive had postoperative radiation. Overall, regional control rate was 94.3% at 5 years
Battoo et al 23 did another retrospective study on 49 patients with oral SCC who underwent SND (I to III/IV) to evaluate its oncologic safety in management of cN1/N2 node-positive disease. Patients were divided into 2 groups with clinical N0 but pathologic N1/N2 (cN0-pN1/N2) and clinical N1/N2 (cN1/N2). Regional recurrence was 4%, and these patients were in the cN1/N2 group. The 3-year ipsilateral regional control rate was 95%.
Schiff et al 24 did a retrospective review similar to ours in which, patients were divided into SND and RND/MRND groups. Of the patients that were confirmed by pathology to be node-positive who received postoperative radiation, 6.2% had neck recurrences after SND and 4% had neck recurrences after RND/MRND. This study suggests that excellent regional control can be obtained with either type of neck dissection. This further supports our data, although this study was limited to oral SCC and did not evaluate overall and disease-specific survival. In addition, there was no comment on the adjuvant chemotherapy.
There are a few limitations to this study. First, it is a retrospective review limited to patients who had complete data regarding survival outcomes. The study could not account for differences in surgeon technique or rationale for SND versus CND/RND. Second, given the limited cohort size, it is possible that with more patients a true difference in the 2 groups would emerge. The limited cohort size also did not allow for a separate analysis of patients regarding whether they received adjuvant concurrent chemoradiotherapy or just RT. Third, all sites were included and analyzed together. Again, it is possible that certain head and neck subsites would show a difference in regional failure rates.
Taken together, our study and the existing literature support the use of SND rather than CND in carefully selected HNSCC patients for the treatment of node-positive neck disease, as long as adjuvant (chemo) radiation is given postoperatively. Favoring SND over CND has the potential to reduce operative complications, shorten surgery time, and result in faster recovery. The importance of selecting the proper patients should be stressed. Patients with bulky nodal disease/N3 disease, gross extracapsular invasion, or invasion into non-lymphatic structures may be better served with more aggressive surgery.
Conclusion
Selective neck dissection, combined with proper adjuvant treatment, achieved regional control and survival rates comparable to CND.
Footnotes
Authors’ Note
The paper was accepted as a poster presentation at the American Head and Neck Society (AHNS) meeting during Combined Otolaryngology Spring Meetings (COSM), April 18-22, 2018, Maryland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.