
Abstract
Objective:
We report a rare case of an intralingual ranula. The differential diagnosis, etiology, diagnostic features, and management are discussed.
Case Report:
An 18-year-old man presented with a mass that extended along the ventral surface of the tongue and up to the tip. The computed tomography scan clearly defined the extent of a cystic lesion. The pathologic diagnosis of an intralingual ranula was made.
Conclusion:
Lingual cysts have a varied etiology. Diagnosis hinges on histological examination of the cyst wall. Conservative resection and histological examination is the standard of care.
Keywords
Introduction
Mucocele is a general term used to describe an abnormal collection of mucous. When it occurred in the tongue, it included numerous entities. We therefore wish to present our experience of the following case and discuss about differential diagnosis, etiology, diagnostic features, and management.
Clinical Case
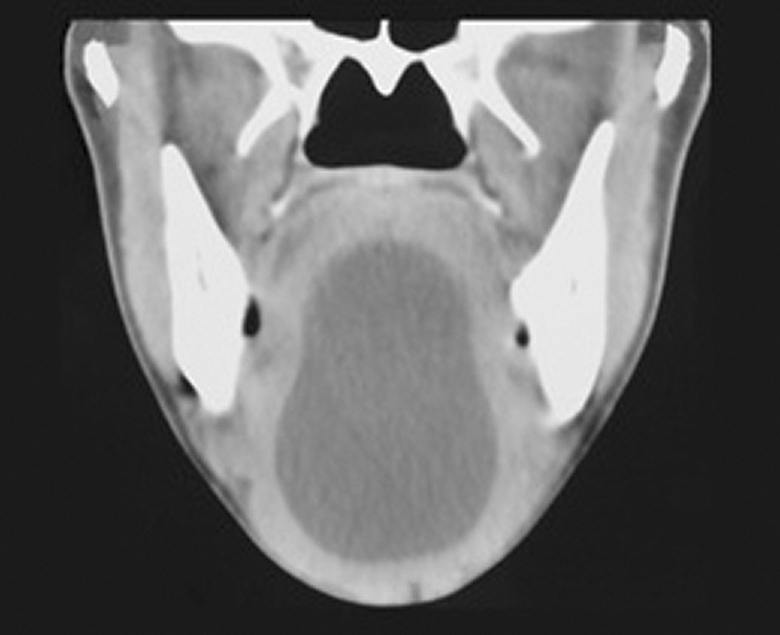
An 18-year-old male presented with a history of intermittent swelling of the ventral surface of the tongue. It had first been noted in early childhood but had only become symptomatic 18 months ago when it enlarged and then ruptured intermittently. A 4-cm-long, midline, submucosal cystic swelling was visible on the ventral aspect of the tongue, extending from the tip of the tongue to the frenulum. Computed tomography (CT) scan demonstrated a thin-walled, intralingual cyst coursing along the ventral midline of the tongue, burrowing into the muscles of the tongue (Figures 1 and 2). The cyst was completely excised and the defect closed with absorbable sutures. The liquid contained in the cyst was thick and straw colored, typically encountered with ranulae. Histologic examination revealed that the cyst contained mucus and that the wall of the cyst was composed of fibroblasts and small-caliber vessels (Figure 3). It did not contain enteric or respiratory epithelium as would be expected with a lingual cyst. 1 –3 Hence, a diagnosis of an intralingual mucous extravasation cyst was made.
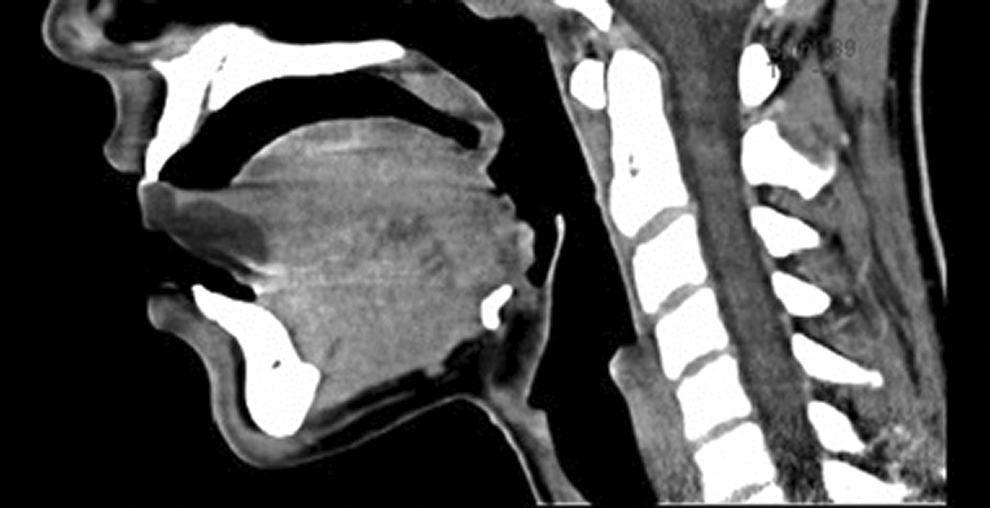
Computed tomography (CT) scan of intralingual ranula, sagittal view.

Computed tomography (CT) scan of intralingual ranula, axial view.
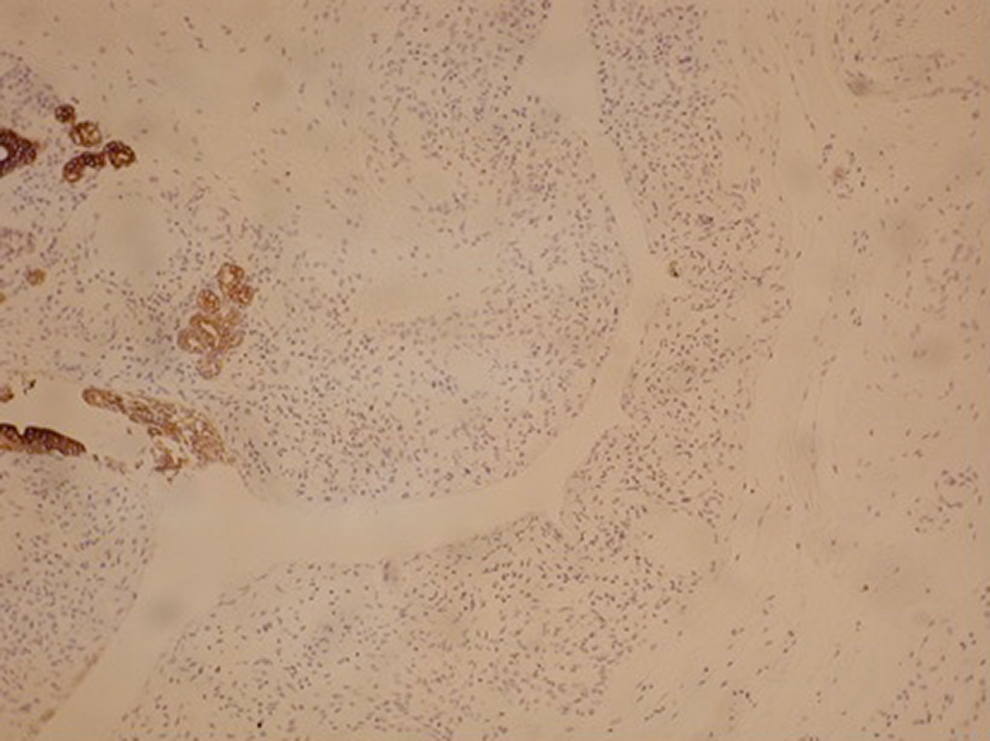
Pankeratin marker (MNF 116) showing no lining to the cyst, but positive staining in the adjacent salivary gland.
Discussion
The differential diagnosis of midline cysts of the anterior/ventral tongue includes lingual cysts; mucoceles; epidermoid, dermoid, and teratoid cysts; lymphoepithelial cysts; lymphangiomas (cystic hygromas); hemangiomas; teratomas; hamartomas; hydatid cysts; and cysticercus cellulosae. 4,5 Lingual cysts may also be clinically confused with lingual lipomas. 6,7
Lingual cysts are of foregut origin and occur in the tongue. 4 They may be symptomatic at birth and manifest with various degrees of feeding and breathing difficulty. Occasionally, they may remain undetected until adulthood. Diagnosis requires histological evidence of an epithelial lining containing respiratory, gastric, or intestinal epithelium or combinations thereof. 3 The embryological explanation for lingual cysts is that rests of foregut epithelium become entrapped between parts of the developing tongue. 1 –3
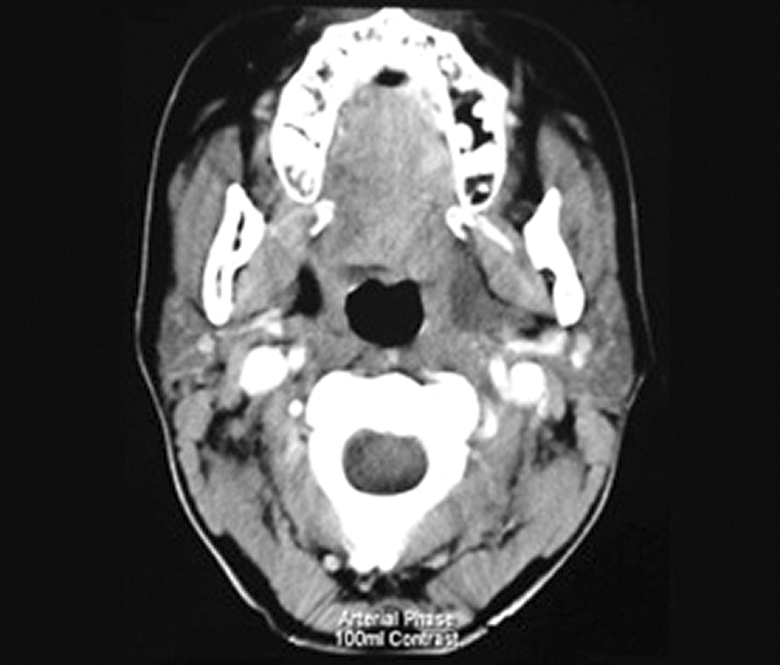
Oral epidermoid and dermoid cysts typically occur in the midline of the anterior floor of the mouth and may elevate the tongue (Figure 4). Intralingual dermoid and epidermoid cysts have been described. 4 Histologically, they comprise epithelial debris entrapped during midline closure of the first and second branchial arches or entrapment during the third and fourth embryonic weeks when the fissures between the lateral swellings of the branchial arches and tuberculum impar close. 1 Teratoid cysts are the rarest of the developmental cysts of the oral cavity and comprise elements derived from ecto-, endo-, and mesoderm. 4
Dermoid cyst of floor of mouth elevating the tongue.
Intraoral lymphoepithelial cysts typically affect the ventral and posterolateral tongue, the floor of mouth, and the rest of the lining of the oral cavity and oropharynx and are clinically indistinguishable from superficial (submucosal) mucoceles. They are thought to originate from epithelial inclusions in lymphoid tissue or from cystic dilatation of superficial ducts of minor salivary glands. 4
Lingual thyroglossal duct cysts present in the region of the foramen cecum to which they are embryologically related. 8 Teratoma and hamartoma should also be included in the differential diagnosis of intralingual cysts. 5 Hydatid and cysticercus cellulosae cysts have been reported to occur in the oral tongue. 4
The term “mucocele” encompasses both mucous extravasation cysts, where mucous has extravasated into the tissues, and mucous retention cysts. Mucous extravasation cysts do not have an epithelial lining, whereas mucous retention cysts are lined by ductal epithelium. 4,7,9,10 Ranulae are mucous extravasation cysts arising from the sublingual salivary glands or less commonly from minor salivary glands. Ranula is derived from the Latin word rana, because of its resemblance to the underbelly of a frog. The term ranula is generally restricted to cysts of the anterior floor of mouth, of which there are 2 types: simple (intraoral) and deep (plunging). They are thought to be caused by traumatic rupture of one or more salivary ducts, with extravasation of mucus into the submucosal tissues planes. The mucus may track through or around the mylohyoid muscle into the neck (plunging ranula) or along fascial planes as far as the parapharyngeal space (Figure 5).
Ranula extending from the anterior floor of mouth to the parapharyngeal space.
Our case was an intralingual extravasation cyst as it did not have an epithelial lining, was filled with mucus, and the cyst was located within the musculature of the tongue having burrowed into the ventral tongue, due to tracking of saliva into the genioglossus muscle. Intralingual mucous extravasation cysts (also referred to as intralingual ranulae in previous reports) have only rarely been reported. 7,9 –12 Mucoceles of the ventral tongue have been associated with the anterior lingual salivary glands, also known as the glands of Blandin and Nuhn. They are mixed mucous and serous glands, measure approximately 8 mm in diameter and 12 to 25 mm in depth, are embedded within the musculature of the anterior tongue ventrum, and drain into the mouth via small ductules in the region of the lingual frenulum. 7,9,10 Unlike our patient, these mucoceles are generally exophytic.
It is not possible to clinically differentiate between a lingual cyst, an intralingual mucous extravasation cyst, and other cysts of the anterior tongue. The CT scan may be helpful to narrow down the differential diagnosis as it will identify a lipoma and may identify calcium deposits and enhancement in hemangiomas. 12,13 Magnetic resonance imaging (MRI) with gadolinium would distinguish a ranula from a hemangioma or lymphangioma. 14 The CT and MRI evidence of a cyst containing membranes and/or daughter cysts and debris is highly suggestive of a hydatid cyst. 15
Because diagnosis generally hinges on histological examination of the cyst wall, conservative excision of such cysts is appropriate. It is unnecessary to resect the sublingual salivary gland, unlike ranulae of the floor of the mouth where resection of the sublingual gland is associated with reduced rates of recurrence. 16 Although sclerotherapy has been employed for treating plunging ranulae, 17 it would be inappropriate for intralingual cases as subsequent scarring might reduce tongue mobility and cause dysarthria.
Conclusions
Lingual cysts have a varied etiology. Intralingual extravasation cysts, though very rare, should be included in the differential diagnosis of intralingual cysts. Conservative resection and histological examination is the standard of care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.