
Abstract
To investigate the application of inner ear 3-dimensional fluid-attenuated inversion recovery (3D-FLAIR) magnetic resonance imaging (MRI) in patients with sudden sensorineural hearing loss (SSNHL) accompanied by inner ear hemorrhage. A total of 1252 SSNHL patients who were admitted from January 2010 to April 2018 were included in the study. The patients’ clinical features, complete blood counts, coagulation profiles, audiometry data, and MRI scans were retrospectively reviewed. Twenty-four patients had high labyrinth signals on inner ear 3D-FLAIR MRI (24/1252, 1.9%) that were diagnosed as inner ear hemorrhage. One patient had endolymphatic hydrops on the contralesional side. In the 24 patients, pure tone audiometry curves revealed profound deafness (19/24) and flat moderate hearing loss (5/24); most patients had associated vertigo (23/24) and tinnitus (19/24). Patients with SSNHL (N = 24) were treated. Sixteen patients had invalid improvement, 3 patients were markedly improved, 4 patients had effective treatment, and only 1 patient was cured, for a therapeutic efficacy of 33.3% (8/24). Follow-up 3D-FLAIR MRI in patients showed absorbance of labyrinthine hemorrhage and disappearance of the high signal intensity in the inner ear within 2 weeks to 4 months. Inner ear 3D-FLAIR MRI indicate that most cases of inner ear hemorrhage are spontaneous and that high labyrinth signals are absorbed within 4 months. The site of labyrinth hemorrhage is irregular and independent of hearing loss. Conventional treatment is not very effective, and an appropriate therapy for SSNHL requires further investigation.
Keywords
Introduction
Sudden sensorineural hearing loss (SSNHL) refers to a rapid hearing impairment of at least 30 dB at 3 consecutive frequencies in one or both ears over a 72-hour period. 1 During the acute stage, only 4.47% to 15% cases of SSNHL can be attributed to identifiable causes after adequate investigation, 2,3 such as vestibular schwannomas (1.85%-6%), 4,5 inner ear or labyrinthine hemorrhage, internal auditory canal metastasis, or ruptured dermoid cysts.
Among these causes, severe initial hearing loss accompanied by vertigo is one of the most well-known factors for a poor prognosis. The characteristics of hearing loss and prognosis of patients with SSNHL accompanied with vertigo or dizziness secondary to labyrinthine hemorrhage remain controversial. From previous case reports, causes of labyrinthine hemorrhage may be hematologic disease, 6 infectious (viral or bacterial) disease, 7,8 vascular disease, immune-mediated disease (within the inner ear or systemically), 9 neurological disease (migraine, multiple sclerosis), neoplasia, or ototoxicity. From 2007 on, as a member of the Chinese multicenter SSNHL randomized controlled trials, we attempted to probe the etiology of SSNHL through magnetic resonance imaging (MRI). As previously reported, high signals in the labyrinth, which can be clearly detected through the 3-dimensional fluid-attenuated inversion recovery (3D-FLAIR) sequence, have been documented to support labyrinthine hemorrhage, with a varied incidence of 0.397% to 6.25%. 5,10 –12
With its unique advantages, 3D-FLAIR MRI has been applied to investigate the etiology of SSNHL and differentiate pathological conditions in the inner ear. The current study attempted to analyze the different sites of labyrinthine hemorrhage through the application of a 3D-FLAIR sequence and to distinguish hearing impairment patterns and evaluate the prognosis of labyrinthine hemorrhage patients in terms of hearing recovery.
Materials and Methods
Ethical Considerations
Written informed consent was obtained from all the participants. The study was approved by the Institutional Review Board of the First Affiliated Hospital of Fujian Medical University. All aspects of the study were conducted according to the Declaration of Helsinki and its later amendments or comparable ethical standards.
Data Collection
A total of 1252 patients diagnosed with clinical SSNHL in our hospital from January 2010 to April 2018 were reviewed in the study. All the recruited patients diagnosed with clinical SSNHL based on American Academy of Otolaryngology Head and Neck Surgery Clinical Practice Guideline: Sudden Hearing Loss. 1 Their clinical data from complete blood count (CBCs), coagulation profiles, pure tone audiometry (PTA), tympanometry, distortion product otoacoustic emissions and transient evoked otoacoustic emissions (DPOAE + TEOAE), auditory brainstem responses (ABRs), and 3D-FLAIR MRI were retrospectively evaluated. Twenty-four patients who were diagnosed with labyrinthine hemorrhage on MRI by 2 trained radiologists and another otolaryngologist were qualified and enrolled as the hemorrhage group (10 males and 14 females, with a mean age of 42 years and an age range of 12-73 years). The control group (nonhemorrhage group) included 40 sex- and age-matched patients who had no abnormal findings related to hearing loss on MRI (20 males and 20 females, with a mean age of 46 years and an age range of 19-80 years). None of the study participants had a neurological disorder or a history of myocardial infarction or head trauma.
Magnetic Resonance Imaging Acquisition and Diagnostic Criteria
The inner ears of all patients were examined by axial 3D-FLAIR, 3D heavily T2-weighted imaging (T2WI), and images were obtained on a 3.0-T MRI unit (Magnetom Verio, Siemens AG, Erlangen, Germany). The procedures were performed as follows: (1) T2WI was performed through the inner acoustic meatus with Turbo SE T2WI (repetition time [TR] = 6000 milliseconds, echo time [TE] = 96 milliseconds, slice thickness = 3 mm) as the scanning sequence; (2) A 3D-SPACE-Inversion Recovery-FLAIR sequence (TR = 6000 milliseconds, TE = 388 milliseconds, inversion time [TI] = 2100 milliseconds, scan time = 5 minutes 32 seconds). The spatial resolution was 0.7 mm × 0.7 mm for the isotropic acquisition. (3) All the original images were transmitted to the workstation and then reconstructed into maximum intensity projections (MIPs), and inner ear MIP images were thus obtained. The images were further rotated from 0° to 180° at every 15°, and multiaxis and multiangle MIP images were obtained.
The diagnostic criteria 13 were as follows: (1) With the cerebrospinal fluid (CSF) as a reference, the inner ear signal was evaluated on the 3D-FLAIR sequence. A signal higher than CSF was considered high signal. (2) The same level of the cerebellar hemisphere was used as a reference. The ratio of signal intensity in the inner ear to the cerebellar hemisphere was calculated (Figure 1). (3) The signal analysis referred to the semiquantitative method of reference, 14 and a ratio > 0.5 was diagnosed as labyrinthine hemorrhage. (4) The morphology and signals on the 3D-FLAIR sequence were calculated by 2 experienced head and neck neuroradiologists who were familiar with the anatomical structure of the inner ear and were blinded to the lesion side of the patients.
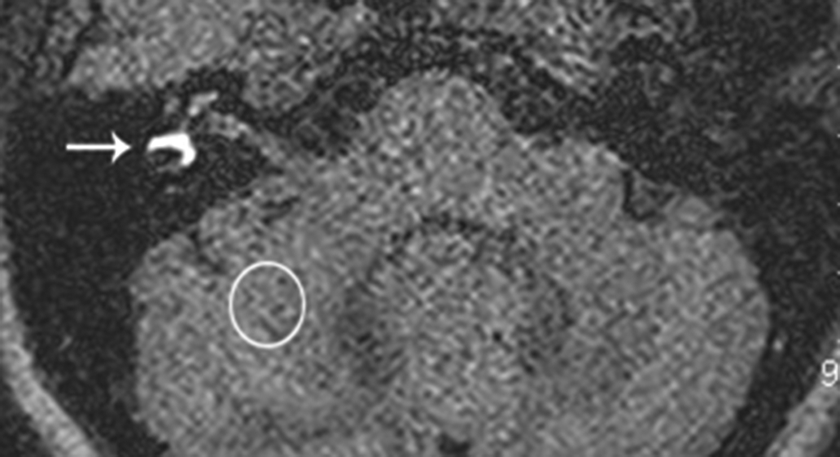
Characteristic image of labyrinthine hemorrhage (axial inner ear MRI T2 3D-FLAIR sequence). The arrow indicates high signal intensity in the right semicircular canal and vestibule. 3D-FLAIR indicates 3-dimensional fluid-attenuated inversion recovery; MRI, magnetic resonance imaging.
Treatment Protocols and Curative Effect Criteria
Referring to Guideline of Diagnosis and Treatment of Sudden Deafness (2015), 2 the treatment protocol was determined according to the type of hearing loss and included vasoactive agents (such as injection of extract from ginkgo biloba leaves), systemic corticosteroids, neurotropic agents (such as mecobalamin), and thrombolytics (such as batroxobin injection) over a treatment course of approximately 7 to 14 days.
The response to therapy was categorized according to the guidelines 2 : (1) Invalid indicated a gain of less than 15 dB on average. (2) Effective indicated that the hearing threshold for the damaged frequency increased by 15 dB to 30 dB on average. (3) Remarkably effective indicated that the hearing threshold for the damaged frequency increased by more than 30 dB on average. (4) Cured indicated that the hearing threshold for the damaged frequency returned to normal, reached the level of the healthy ear, or reached the level before the illness.
Effective rate = (cured + remarkably effective + effective) patients/total patients × 100%.
Statistical Analysis
All statistical analyses were performed using SPSS version 22.0 (IBM Corp. for Windows) with the level of significance setting at P < .05. The differences between groups were analyzed by the χ2 test, and significance was defined as P < .05.
Results
A total of 1252 SSNHL patients underwent inner ear MRI including 3D-FLAIR sequences. High signal intensity was found in various parts of the inner ears of 24 patients, with an incidence of labyrinthine hemorrhage of 1.9% (24/1252). The demographic and clinical data of the 24 patients (the hemorrhage group) are summarized in Table 1. The clinical symptoms of most labyrinthine hemorrhage patients were profound deafness (17/24, 77.3%), vertigo (23/24, 95.8%), and tinnitus (19/24, 79.2%). Inner ear hemorrhage in the 24 patients was unilateral. The lesion laterality was 8/24 (33.3%) in the left ear and 16/24 (66.7%) in the right ear, at a ratio of 1:2 (left to right). The average length of time for treatment protocol is 9.8 ± 2.6 days. No significant differences were found in gender, age, and length of time for treatment. One patient (case 7) CBC showed red blood cell (RBC) 2.5 × 1012/L (↓), HGB 79 × 1012 g/L (↓), cell volume 0.3 L/L (↓), mean corpuscular volume 103.2fL (↑). Coagulation profile showed thromboplastin time24.9 seconds, activated partial thromboplastin time 46.2 seconds. For the hemorrhage group, PTA revealed profound deafness in 19 patients and flat moderate hearing loss in 5 patients. The χ2 test showed no significant correlation between the type of hearing loss and the site of hemorrhage in the inner ear. Tympanic curve analysis showed: Type A in 20 patients, Type As in 3 patients, and Type Ad in 1 patient. Transient evoked otoacoustic emissions + DPOAE were abnormal in 23 patients and normal in 1 patient. Evaluation of ABRs revealed no response in 17 patients, abnormal response in 6 patients, and a normal response in 1 patient.
Demographics of 24 Patients With Labyrinthine Hemorrhage.a
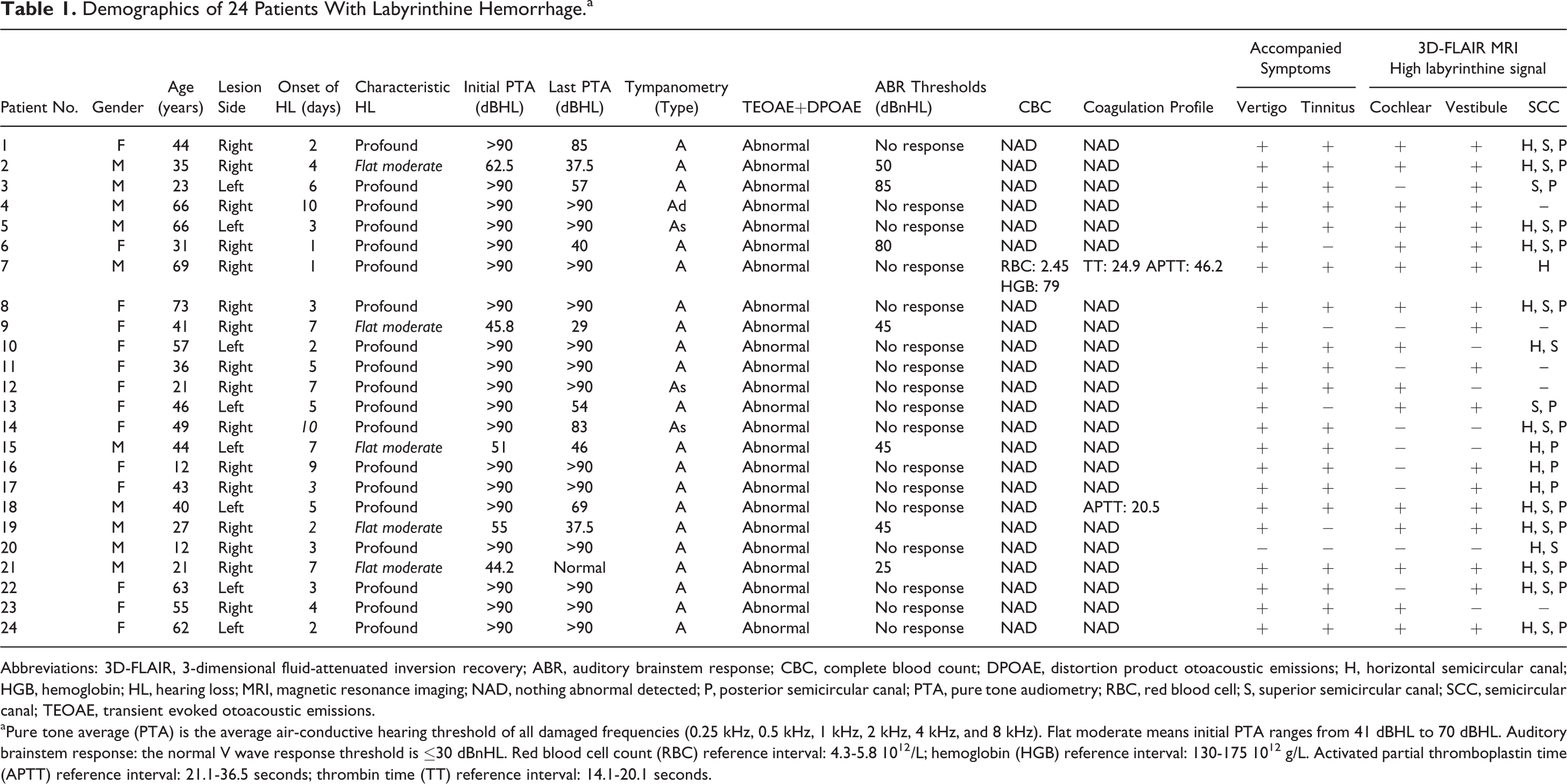
Abbreviations: 3D-FLAIR, 3-dimensional fluid-attenuated inversion recovery; ABR, auditory brainstem response; CBC, complete blood count; DPOAE, distortion product otoacoustic emissions; H, horizontal semicircular canal; HGB, hemoglobin; HL, hearing loss; MRI, magnetic resonance imaging; NAD, nothing abnormal detected; P, posterior semicircular canal; PTA, pure tone audiometry; RBC, red blood cell; S, superior semicircular canal; SCC, semicircular canal; TEOAE, transient evoked otoacoustic emissions.
aPure tone average (PTA) is the average air-conductive hearing threshold of all damaged frequencies (0.25 kHz, 0.5 kHz, 1 kHz, 2 kHz, 4 kHz, and 8 kHz). Flat moderate means initial PTA ranges from 41 dBHL to 70 dBHL. Auditory brainstem response: the normal V wave response threshold is ≤30 dBnHL. Red blood cell count (RBC) reference interval: 4.3-5.8 1012/L; hemoglobin (HGB) reference interval: 130-175 1012 g/L. Activated partial thromboplastin time (APTT) reference interval: 21.1-36.5 seconds; thrombin time (TT) reference interval: 14.1-20.1 seconds.
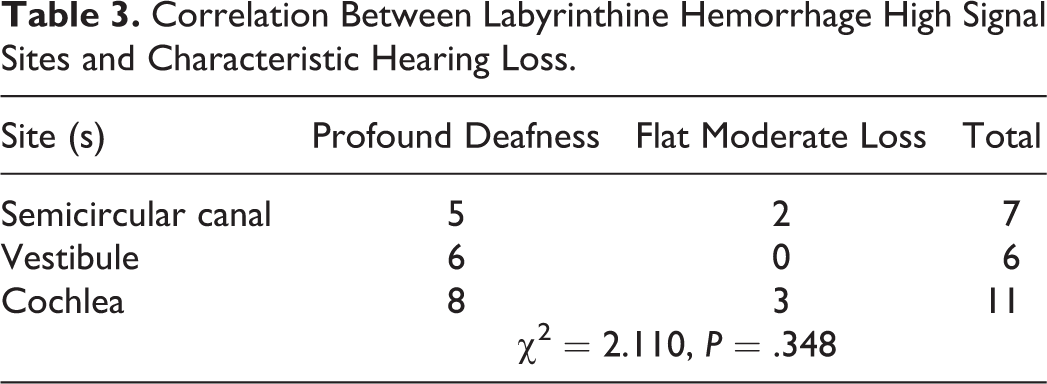
The distribution of high signal intensity in the inner ear on 3D-FLAIR MRI involved the horizontal semicircular canal (H, 17 patients), superior semicircular canal (S, 15 patients), posterior semicircular canal (P, 16 patients), vestibule (Ve, 18 patients), and cochlea (Co, 15 patients). One patient had endolymphatic hydrops on the contralesional side. Chi-square tests revealed no significant difference between the distributions of lesion areas (χ2 = 1.292, P > .05; Table 2) or between the site of labyrinthine hemorrhage and hearing loss when the latter was considered (P > .05; Table 3). The initial MRI scans following sudden hearing loss ranged from 4 to 53 days, with a mean of 12.2 days.
The Distribution of Lesion Areas of 24 Labyrinthine Hemorrhage Cases.

Abbreviation: Sc, semicircular canal.
Correlation Between Labyrinthine Hemorrhage High Signal Sites and Characteristic Hearing Loss.
After the treatment, 16 patients had invalid improvement, 3 patients were markedly improved, 4 patients showed effective hearing improvement, and 1 patient was cured, for an efficacy rate of 33.3% (8/24). There were 3 cases involving the left ear and 5 cases involving the right ear, which were compared with those before treatment by the χ2 test. The difference in therapeutic benefits depending on the lesion side was not statistically significant (χ2 = 0.187, P > .05).
For the nonhemorrhage group, PTA revealed profound deafness in 25 patients and flat moderate hearing loss in 15 patients. After treatment, 29 patients were unresponsive, and 11 patients had effective treatment. However, no significant difference in curative effect was found between the labyrinthine hemorrhage group and the control group (χ2 = 0.245, P > .05).
All 24 SSNHL patients from the hemorrhage group returned for a follow-up 3D-FLAIR MRI, which showed absorbance of the labyrinthine hemorrhage and disappearance of the high signal intensity in the inner ear within 2 weeks to 4 months.
Typical Case 1 (Case 17)
The patient (43-year-old female) was admitted to the hospital with a history of hearing loss in the right ear for 3 days accompanied by vertigo and tinnitus. She received primary 9-day treatment from a collaborative hospital based on Guideline of Diagnosis and Treatment of Sudden Deafness (2015) 1 before transferring to our institute. Pure tone audiometry indicated right profound sensorineural hearing loss (Figure 2A). An acoustic impedance examination suggested a Type A tympanic curve. An ABR threshold examination showed that the V wave response threshold of the right ear was not induced. Her otoacoustic emissions were abnormal, while her CBC and coagulation profile were normal. On the 35th day after the onset of SSNHL, the patient underwent inner ear MRI, including a 3D-FLAIR sequence, which revealed high signal intensity in the right H, P, and Ve (Figure 3A). The patient was diagnosed with labyrinthine hemorrhage. The treatment involved suspending vasoactive agents and thrombolytics and continuing systemic corticosteroids and neurotropic agents. Six days later, a repeated PTA revealed right profound sensorineural hearing loss (Figure 2B). Two months later, a follow-up 3D-FLAIR MRI scan revealed high signal intensity only in the right horizontal semicircular canal ampulla (Figure 3B); MIP MRI image demonstrating symmetric labyrinthine uptake(Figure 3C).
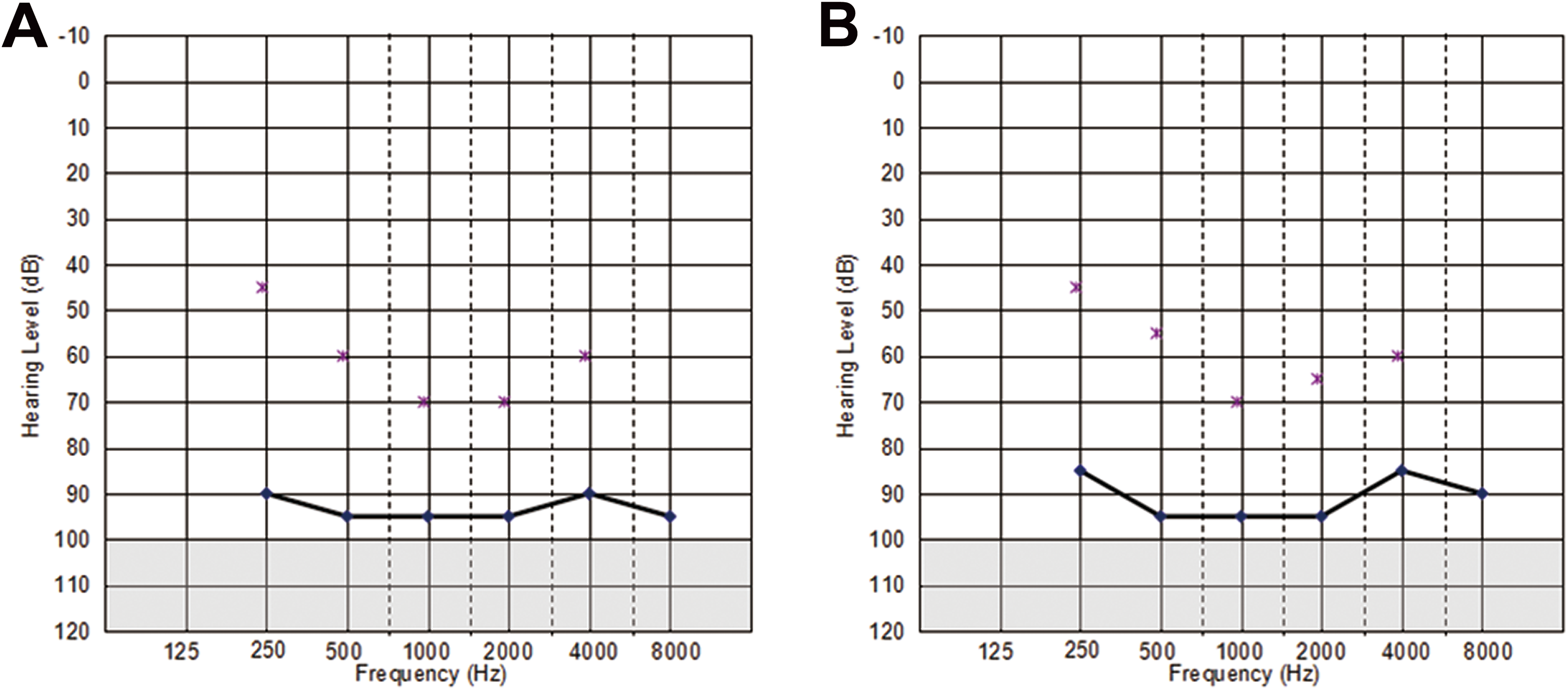
A, Initial PTA indicated right profound sensorineural hearing loss at 93 dBHL. B, PTA 6 days after the treatment showing no improvement in right-sided hearing at 91 dBHL. PTA indicates pure tone audiometry.

A, Labyrinthine hemorrhage. An axial T2-weighted 3D-FLAIR MRI image reveals higher signal intensity in the right H, P, and Ve (arrows). B, A 2-month follow-up T2 3D-FLAIR MRI image shows mildly high signal intensity in the right HC (arrows). C, A 2-month follow-up inner ear MIP MRI image demonstrating symmetric labyrinthine uptake. 3D-FLAIR indicates 3-dimensional fluid-attenuated inversion recovery; H, horizontal semicircular canal; MIP, maximum intensity projection; MRI, magnetic resonance imaging; P, posterior semicircular canal; Ve, vestibule.
Discussion
Inner ear hemorrhage is rare and difficult to diagnose during the acute stage of SSNHL. Our study utilized inner ear 3D-FLAIR MRI sequences to provide an established and objective diagnostic modality for evaluating SSNHL patients. In principle, inner ear MRI can reveal high signal intensity resulting from fat and protein, which indicates inflammatory or hemorrhagic lesions. On MRI, inflammatory lesions, such as labyrinthitis and/or vestibulocochlear neuritis, show low signal on T1-weighted images and marked high signal intensity on T2-weighted 3D-FLAIR images.
In our investigation, patients with inner ear hemorrhage showed high signal intensity on T1-weighted images and marked low signal intensity on T2-weighted images but high signal intensity on T2-weighted FLAIR images. Several previous studies have noted high signal intensity in the inner ear on precontrast and postcontrast 3D-FLAIR MRI and attributed this finding to the breakdown of the blood-labyrinth barrier and the destruction of erythrocytes in the inner ear, which produce intracellular methemoglobin. 10 –12,15 Therefore, 3D-FLAIR imaging is of great clinical importance for the diagnosis of inner ear hemorrhage and is also an objective technique for evaluating inner ear pathology early in the course of disease.
In our study, only 1 patient had abnormal CBC findings, and 2 patients had mildly abnormal coagulation profiles. Labyrinthine hemorrhage was not related to abnormal CBC findings or coagulation dysfunction, which indicates that most labyrinthine hemorrhage is spontaneous. In our opinion, SSNHL can be evaluated with routine inner ear 3D-FLAIR MRI, which is beneficial for the early detection of the etiology in SSNHL patients and timely treatment.
In addition, we analyzed the distribution of high signal intensity in the inner ear on 3D-FLAIR MRI. We found no statistical significance between various hemorrhagic lesion sites in the inner ear, which indicates that hemorrhagic lesions are irregular and are more inclined to involve the whole inner ear (12/24, 50.0%). Most labyrinthine hemorrhage sites showed high signal intensity in the cochlea. Based on Kim et al study, high signals involving both the endolymphatic and perilymphatic compartments of labyrinth on pre- or post-enhanced 3D FLAIR images without enhancement are the characteristic MRI imaging finding of labyrinthine hemorrhages. 10 Kaya et al 16 analyzed temporal bone dissections of 46 labyrinthine hemorrhage patients and found that labyrinthine hemorrhage could induce a significant loss of outer hair cells in the cochlea and endolymphatic hydrops, which accounts for hearing loss and vertigo. Even if no high signal was present in the cochlea on the 3D-FLAIR sequence, the hearing of labyrinthine hemorrhage patients also declined.
Magnetic resonance imaging showed that the inner ear structure was normal in all SNNHL hemorrhage group. We suspect that the symptom of vertigo results from changes in the lymphatic environment that are caused by the infiltration of methemoglobin. Methemoglobin leads to lipid peroxidation and inhabits sodium/potassium (Na/K) adenosine triphosphatase (ATPase) activity. 17 Kaya et al 17 quantitatively demonstrated that inner ear hemorrhage may damage vestibular hair cells but not dark cells or transitional cells, which suggest a decrease in vestibular hair cells (especially type Ⅰ) might lead to vertigo/dizziness. Furthermore, the changed microenvironment in the inner ear causes abnormal nerve stimulation and results in tinnitus. With the absorption of ruptured RBC and the improvement in the environment of lymphatic fluid and microenvironment of the inner ear, the accompanying symptoms, especially vertigo and tinnitus, can be greatly alleviated. In the follow-up review, hearing was not improved in some patients, which was probably due to irreversible damage to the cochlear hair cells and their function.
Lesion laterality in the left ear and right ear was 33.3% (8/24) and 66.7% (16/24), respectively. Three patients with left ear laterality and 5 patients with right ear laterality were effectively treated. The χ2 test showed that the therapeutic effect was not related to the affected side. We also showed that the sites of hemorrhage were not related to hearing loss. Therefore, labyrinthine hemorrhage patients, regardless of the severity of hearing loss, should be treated. The rate of treatment efficacy in the 24 labyrinthine hemorrhage patients was 33.3% (8/24), and 1 patient was even cured. Jan et al 18 and Chen et al 19 separately identified labyrinthine hemorrhage patients with potential word recognition scores recovery during at least 6 months follow-up, despite no improvement in PTA in the affected ear, either spontaneously or via corticosteroid intervention. We suggest that 3D-FLAIR MRI should be routinely performed as early as possible for patients with sudden deafness. Patients with labyrinthine hemorrhage should stop using vasoactive agents and thrombolytics and should continue using corticosteroids and neurotropic agents, which are beneficial for hearing improvement.
Considering case 21, the initial PTA showed right flat moderate sensorineural hearing loss. However, ABR, DPOAE, and TEOAE were normal (S/N-ratio dB Right < Left sided). The possible etiopathogenesis might be that labyrinthine hemorrhage caused mild damage to the outer hair cells, which could be reversed by timely treatment.
Shinohara et al 20 reported that although red blood corpuscles normally have a life span of approximately 120 days in the vessel, high signals persisted for more than 6 months. Yoshida et al 21 performed a follow-up MRI study (11/48) and found that high signals in the affected inner ears on precontrast or postcontrast 3D-FLAIR scans disappeared after approximately 90 to 150 days from the onset of SSNHL. In our study, we believe that the labyrinthine hemorrhage-induced high signals will disappear within 4 months, which may be related to self-limiting inner ear hemorrhage and absorption of this hemorrhage. Theoretically, we have to rule out intratumoral hemorrhage, which would disappear after 4 months on FLAIR, but contrasted T1 images would still show hyperintensity. Bastier et al 22 reported characteristic MRI imaging of 3 endolymphatic sac tumors, those are presence of cysts and spontaneous hemorrhage, hyperintense on T1-weighted images, hypointense bone spicules and flow void on T1- and T2-Weighted images, and heterogeneous enhancement after injection at MRI. Jeong et al also observed 9 patients of intralabyrinthine schwannoma can display characteristic MRI findings of a lack of normal fluid density on T2-weightd imaging, with corresponding enhancement observed on gadolinium-enhanced T1-weighted scans. 3 Therefore, we suggest that 3D-FLAIR MRI should be repeated after 4 months in patients with intratumoral hemorrhage. If high signal intensity persists, it is necessary to rule out the possibility of etiologies other than labyrinthine hemorrhage-induced SSNHL.
Although the incidence of inner ear hemorrhage is low (1.9%), inner ear 3D-FLAIR sequence imaging is vital to diagnose SSNHL accompanied by inner ear hemorrhage and can assist in timely treatment adjustments and provide new radiographic indicators to aid in prognosis. 11,21
Kaya et al 16 found that labyrinthine hemorrhage does not damage inner hair cells, spiral ganglion cells, the stria vascularis, or the spiral ligament. Thus, we speculate that patients with labyrinthine hemorrhage can serve as candidates for amplification with hearing aids or cochlear implants. One enlarged vestibular aqueduct (EVA) syndrome patient (case 20), who had a history of bilateral hearing loss for 12 years with hearing aids, suffered from right sudden hearing loss accompanied by labyrinthine hemorrhage and was ultimately afflicted with bilateral profound hearing loss. The patient received a left cochlear implant and rehabilitated well. Koesling et al 23 reported one patient with labyrinthine hemorrhage after sudden hearing loss among 17 EVA patients (28 ears). The plausible mechanism for this hemorrhage may be an increase in intracranial pressure with a consecutive increase in pressure within the endolymphatic system and rupture of the stria vascularis, but no trigger mechanisms have yet been verified. Generally, patients with labyrinthine hemorrhage-induced bilateral profound deafness who were deafened postlingually can benefit considerably from cochlear implantation and have an improved prognosis.
This study has some limitations by its retrospective nature. We only relied on clinical features, audiological results, and MRI findings to diagnose inner ear hemorrhage. Therefore, the suggested explanation for labyrinthine hemorrhage remains speculative. The number of patients who underwent follow-up was limited, and the results of our study should be confirmed by well-controlled, prospective, randomized controlled studies of clinical cases. The treatment of inner ear hemorrhage is still limited to corticosteroid medications, neurotropic agents, and other medications. Many future efforts are urgently needed to explore the clinical effectiveness of medical treatment, the correlation between prognosis and the onset of the disease, and the dilemma of whether to stop using vasoactive agents and thrombolytics. To develop more effective therapies, it is necessary to understand the natural history and pathology of labyrinthine hemorrhage more precisely.
Conclusion
In summary, inner ear 3D-FLAIR MRI indicated that most cases of inner ear hemorrhage were spontaneous and that high labyrinth signals were absorbed within 4 months. The labyrinth hemorrhage sites were irregular and independent of hearing loss. Generally, patients with labyrinthine hemorrhage should stop using vasoactive agents and thrombolytics and should continue using corticosteroids and neurotropic agents, which are beneficial for hearing improvement. If possible, we suggest the first follow-up MRI scan could be arranged 4 months later after the onset of labyrinthine hemorrhage with SSNHL.
Footnotes
Authors’ Note
Xi-Hang Chen and Chao-Jun Zeng are co-first authors and contributed equally to this study.
Acknowledgments
Authors are grateful to Mr Hong-Zhi Huang (School of Foreign Languages, Fujian Medical University) for reviewing our manuscript for clarity.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2017 Youth Project, which is funded by Fujian Provincial Health and Family Planning Commission (grant number 2017-1-52).