
Abstract
Physiological changes in pregnancy may cause taste dysfunction. The aim of this study was to determine and compare gustatory function of pregnant women with nonpregnant women and also to investigate the effect of pregnancy on gustatory function. It was a case–control study of consecutive 70 healthy pregnant women (cases) and 70 healthy nonpregnant women (control). Participants scored their taste perception on a visual analogue scale (1-10) and their gustatory function was assessed using “taste strips” impregnated with graded concentration of sweet, sour, salty, and bitter taste substances applied on tongue surfaces. Subjective mean gustatory score, correct identification of taste in the strips and total taste strip (TTS) score were compared between both groups and analysis was done using appropriate statistics. The mean age of pregnant women (30.5 [3.9]) and controls (28.5 [6.6]) were comparable. Twenty-one (30%) pregnant women changed their diet in first trimester due to change in taste sensation. Almost all cases developed craving for spicy and salty foods and, aversions to fish, beans, and vegetables. There was a significant difference in the subjective rating of taste perception between the 2 groups (P = .037). About 2.9% of pregnant women have hypogeusia. There was a significant difference between pregnant and nonpregnant women in sour taste (P = .006; 2.90 [0.71] vs 3.92 [0.82]) and TTS (P = .02; 27.50 [3.48] vs 29.21 [2.69]) scores, respectively. In conclusion, gustatory function was reduced in pregnancy compared to nonpregnant women and this led to dietary change in some pregnant women.
Introduction
Taste bud is a special sense which is important in perception of taste and appreciation of food flavor as well as its palatability. Taste is very important as it could be an early warning sign against toxins and spoilt food products which might be injurious to human body. 1 It plays a role in appetite stimulation and triggers secretion of salivary, gastric, pancreatic, and intestinal juices in preparation for food digestion. 2 In addition, it enables one to discriminate among food and select nutritive savory meals in the face of fluctuating nutritional requirements.
Aging, upper respiratory tract infection, HIV/AIDS, viral hepatitis, autoimmune and inflammatory diseases, cancer, chemotherapy and radiotherapy, and so on are diseases or disorders reportedly associated with taste dysfunction. 3,4 Transient physiological changes can modify taste neuron activity. 5 Pregnancy, which is a normal physiologic process, may cause a change in gustatory function. 6,7 Reduced sensitivity to taste qualities as well as development of craving, aversion, and preference for particular type of food have been reported in some pregnant women. 8 –12 There is paucity of such information among pregnant women in Africa where there is still high burden of malnutrition.
Poor taste may put an individual at risk of poor nutritional intake. The practice of adding more salt or sugar to improve food taste may predispose to hypertension or gestational diabetes, respectively. 13 Pregnant women require good and adequate nutritional intake for sustainable healthy living as well as growth and development of their unborn child. Since aversions and cravings are closely linked to dietary intake, understanding these behaviors in pregnant women is important for nutrition. There is, however, a dearth of documentation on the effect of pregnancy on the sense of taste in this environment. This study was designed to determine and compare gustatory function of pregnant women with nonpregnant women as well as investigate the effect of pregnancy on gustatory function. The findings from this study would be useful in providing appropriate nutritional counseling and guide to women.
Materials and Methods
This was a case–control study of consecutive 70 healthy pregnant women (cases) and 70 healthy nonpregnant women (control) between September 2016 and December 2016 at the University College Hospital, Ibadan, Nigeria. The controls were women with menstrual cycle of 28 to 31 days that tested negative for pregnancy test. Ethical approval was obtained from the University of Ibadan/University College Hospital review board for the conduct of the study. Informed consent was also obtained from the participants in the study. The exclusion criteria included women with history of smoking, dry mouth, oral or salivary gland diseases, head and neck tumors, diabetes, exposure to radiotherapy, or on routine medications except hematinic. All the pregnant women tested negative to HIV screening and venereal disease research laboratory.
Pro forma
A pro forma was administered to all participants to obtain relevant information on sociodemographic; medical history including dryness of mouth, oral ulcer or swelling, diabetes, hypertension, smoking, alcohol intake, loss of taste, change in taste during pregnancy, preference for sweet, salt, sour, and bitter taste; aversion and craving for food; routine medications; and other clinical data. Participants were socially stratified based on occupational strata devised by Famuyiwa et al. 14
Subjective Assessment
Subjective self-rating of taste perception was scored on a visual analog scale from 1 to 10 (where 1 stands for complete loss of perception of taste and 10 stands for excellent perception of taste). A score of 1 to 2 is very poor, 3 to 4 is poor, 5 to 6 is good, 7 to 8 is very good, and 9 to 10 is excellent.
Test for Taste
Participants were instructed not to eat food or drink for at least 2 hours before the test of taste which was done after mouth rinsing with clean water. The taste functions of the participants were assessed using 16 filter paper strips (‘‘Taste Strips’’; Burghart Messtechnik Gmbh, Wedel, Germany) impregnated at one end with 0.05, 0.1, 0.2, or 0.4 g/mL sucrose (sweet taste); 0.05, 0.09, 0.165, or 0.3 g/mL citric acid (sour taste); 0.016, 0.04, 0.1, or 0.25 g/mL sodium chloride (salty taste); or 0.0004, 0.0009, 0.0024, or 0.006 g/mL quinine hydrochloride (bitter taste). 15 The taste strips were presented in increasing concentrations in a randomized fashion, alternating the side of presentation. The participants were told to identify the taste with their tongue still extended from the 4 descriptors, that is sweet, sour, salty, and bitter (4-alternative forced choice). The taste strips were applied on the left and right side of the protruded tongue, about 1.5 cm from the tip; at different times resulting in a total of 32 trials. The strips were presented at intervals of 30 seconds from one another. The participant’s taste detection threshold is the lowest concentration at which the taste being tested can be detected. Wrong identification of each taste strip at the strongest concentration was scored 0, and correct identification was scored from 1 to 4. Correct identification of the taste at the lowest concentration was 4 and at the highest was 1. The minimum and maximum scores on one side of the tongue is 0 and 16, respectively. Thus, the overall total taste score (OTTS), which is the sum of the score from both sides of the tongue, ranged from 0 to 32. Based on normative data for “taste strips,” hypogeusia was defined as the score below the 10th percentile. Sweet score <2, sour <2, salty <2, bitter <1 for each side of the tongue, total score for each side of the tongue <9, or score from both sides of the tongue of <19 were suggestive of hypogeusia. 15,16 Scores ≥10th percentile was suggestive of normogeusia. Scores of taste test of the pregnant women were compared to that of nonpregnant women and normative values by Landis et al, 15 respectively. New taste strips were used for each participant.
Statistical/Data Analysis
The sociodemographic and clinical characteristics of the pregnant and nonpregnant women were compared using χ2 tests. The comparison of mean subjective gustatory scores between pregnant women and nonpregnant women was done using the independent samples t test. Descriptive data were presented as mean (standard deviation [SD]) and proportion for quantitative and qualitative variables, respectively. Association between categorical variables was explored using χ2 or Fisher exact test, while association between quantitative variables was done using the Student t test for 2 groups and analysis of variance for more than 2 groups. Association between participants’ characteristics and TTS was tested. Correlation between continuous variables was determined using Pearson correlation coefficient. Level of significance was determined at P < .05 and 95% confidence interval.
Results
Participants’ Sociodemographic and Clinical Characteristics
A total of 70 consecutive pregnant women and 70 nonpregnant women participated in the study. The age range of the pregnant women was from 22 to 38 years with a mean age of 30.5 (3.9) while that of nonpregnant women (control group) was from 20 to 40 years with a mean age of 28.5 (6.6). There was no significant difference between the age of participants in the 2 groups (P = .0987). Two (2.9%) of the pregnant women were in their first trimester, 28 (40%) in the second trimester, and 40 (57.0%) in the third trimester.
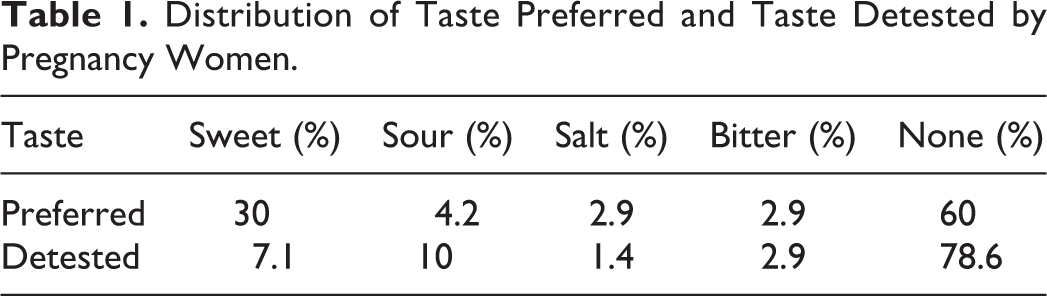
None of the participants reported loss of sense of taste. Twenty-one (30%) pregnant women changed their diet in the first trimester of pregnancy due to change in taste sensation, and 5 (23.8%) of them believed that the change in taste sensation was due to pregnancy. Six (8.6%) pregnant women experienced craving for food during pregnancy while 17 (24.3%) pregnant women reported food aversions during pregnancy. Almost all the pregnant women (95.7%) preferred their food to be spicy. About 30% of the pregnant women preferred sweet taste while 10% detested sour taste in pregnancy. The type of tastes preferred and detested by the pregnant women are shown in Table 1.
Distribution of Taste Preferred and Taste Detested by Pregnancy Women.
Subjective taste perception
The mean subjective taste assessment result of pregnant women was 6.6 (0.2) while that of nonpregnant women was 7.6 (2.3). There was a significant difference in the subjective self-rating of taste perception between the pregnant women and nonpregnant women (P = .037).
Objective Taste Test
The sour taste detection threshold, left total taste score, right total taste score, and OTTS of the pregnant women were significantly different from those of nonpregnant women (P < .05). The comparison in the taste detection thresholds between the pregnant and nonpregnant women is shown in Table 2. There was a significant difference in the sour and total taste score between the pregnant and nonpregnant women.
Comparison of the Taste Detection Threshold Between the Pregnant and Nonpregnant Women.
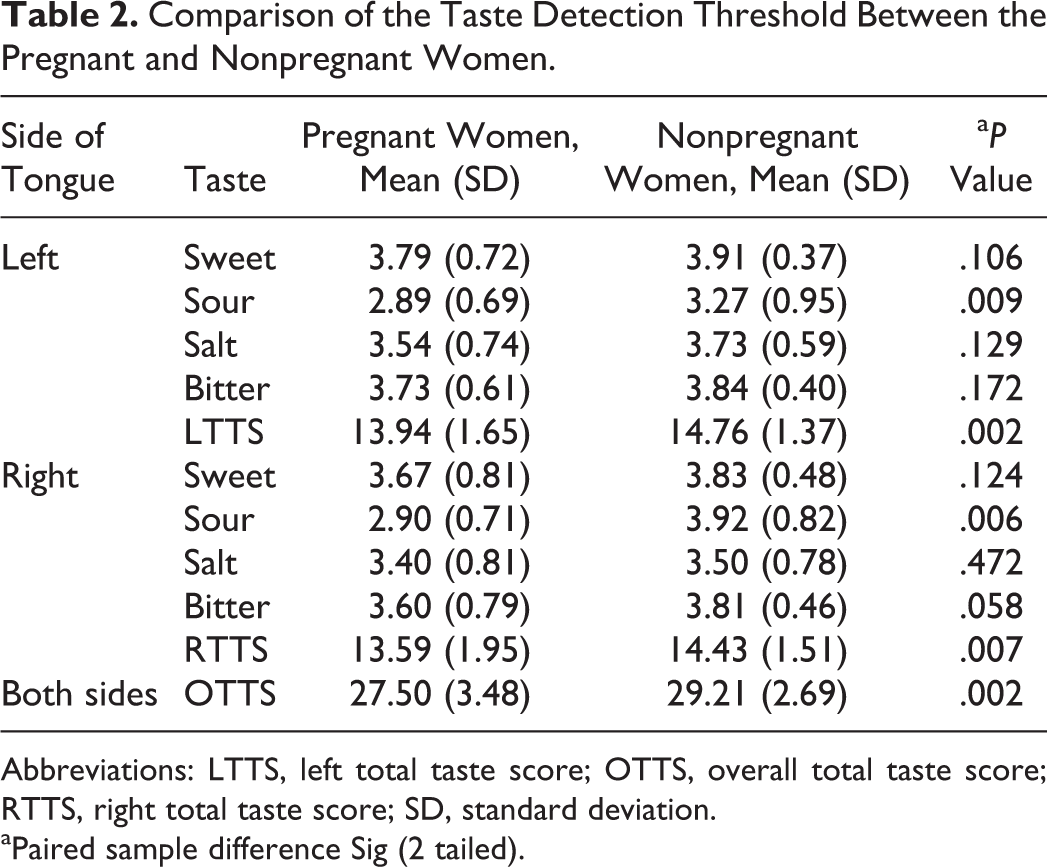
Abbreviations: LTTS, left total taste score; OTTS, overall total taste score; RTTS, right total taste score; SD, standard deviation.
aPaired sample difference Sig (2 tailed).
The gustatory function of the left side of the tongue was significantly better than the right for salty taste and total taste score in both groups and for bitter taste only among the pregnant women (Table 3).
Comparison of Taste Detection Thresholds Between Left and Right Side of the Tongue.
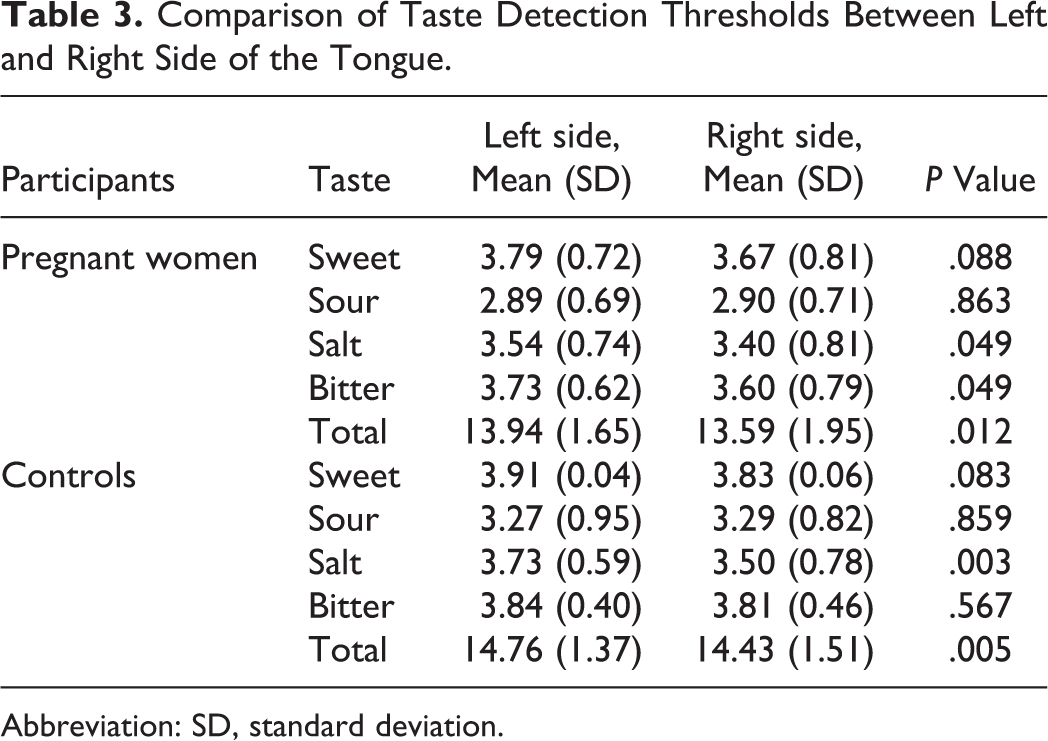
Abbreviation: SD, standard deviation.
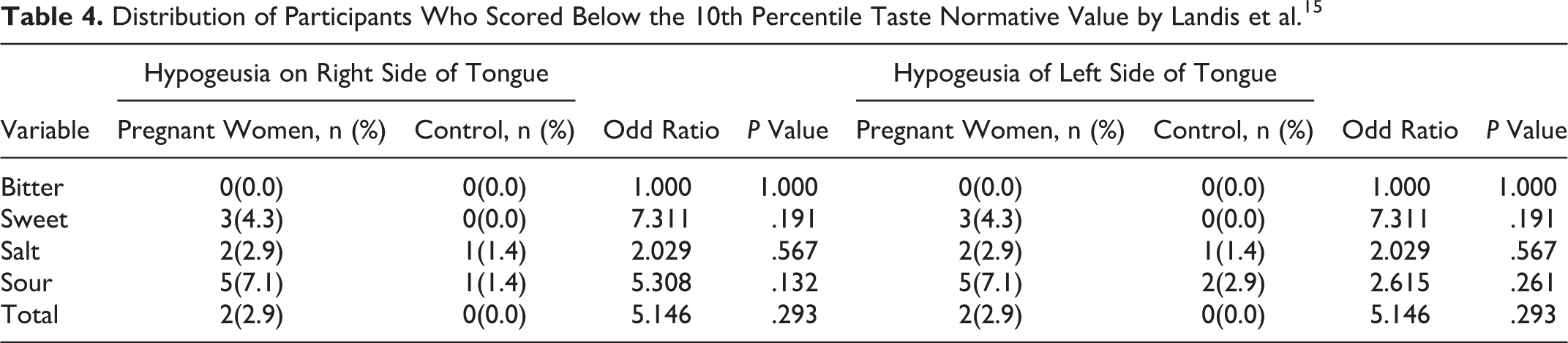
There was no significant difference in the gustatory function of the 28 pregnant women in the second trimester and nonpregnant women (P = .892), but there was difference between the 40 pregnant women in their third trimester and the nonpregnant women (P = .048). The pregnant women have increased tendency of being hypogeusic than the nonpregnant women (Table 4). Table 4 shows the distribution of participants who scored below the 10th percentile normative data for “taste strips” value by Landis et al. 15
Distribution of Participants Who Scored Below the 10th Percentile Taste Normative Value by Landis et al. 15
Discussion
Taste is the capability to identify and distinguish ingested substances. It is mediated by taste bud and affects appetite and choice of food. Pregnant women require healthy taste for adequate nutritional intake. Their nutritional status will invariably influence nutritional health status, growth, and development of their babies. Sense of taste protects against ingestion of toxic substance or spoilt food which might be injurious to both mother and their unborn child.
In pregnancy, many physiological changes take place and a change in taste is one of them. 6–7 This is confirmed in this present study where 30% of the pregnant women experienced change in taste. About 40% of the pregnant women have specific taste preference while only 22% of them detest particular taste. The change in taste may not be unconnected with hormonal changes and different dietary needs of pregnant women. The preference for sweet taste reported by 30% of the pregnant women may make them add more sugar or sweetener to improve the taste of food. This increase in calorie intake may predispose to weight gain, hyperglycemia, or diabetes thereby making them to have big babies with accompany difficulty in successful natural vagina delivery. In a similar study by Ochsenbein-Kolble et al, 7 sour taste was the most preferred by the pregnant women. This difference may be explained by cultural experiences and genetic differences. Similarly, the 2.9% of the pregnant women that preferred salty taste are at risk of garnishing their food with more salt thereby predisposing them to increased water retention and hypertension. Unfortunately, we did not measure the plasma glucose or blood pressure of the participants to know whether they had actually developed the disease.
Food cravings and aversions may be as a result of physiological, psychological, and cultural influences. 8,11,12 The aversion for food reported by 24.3% pregnant women may not be unrelated to changes in their taste and this may predispose them to develop anemia. In Africa, the prevalence of anemia in pregnancy ranged from 35% to 75% while a study in Nigeria has reported a prevalence of 6.5%. 17,18 Anemia in pregnancy may predispose to still birth, premature delivery, and low birth weight. 18 –20
In this study, food craving was reported by 8.6% of pregnant women. This is similar to findings from similar studies where food craving was reported among 3.4% pregnant women in Tanzania 11 and 67% to 84% pregnant women in various groups in South Africa. 21 Pregnant women may eat more of or avoid a particular food depending on the information they have received. If a particular food is recommended, it might trigger a craving to eat that food. For example, pregnant women in Kenya often eat “Odowa” (soft stone) because of the belief that it increases woman’s strength during labor and it is a source of iron supplement and tonic needed for their babies’ growth and development. 22 Pica was reported among 29% of Mexican women during pregnancy. 23
A change in taste sensitivity has been reported in similar studies on pregnant women. 6,7,24,25 The taste detection threshold of pregnant women was significantly lower when compared to nonpregnant women (P = .002 or Table 2). Decrease in a particular taste sensitivity or detection threshold will make the individuals to add supplements that will improve the missing taste to their food so as to have savory meals. In this study, the sour, bitter, sweet, and salty taste detection thresholds of pregnant women were lower than those of nonpregnant women. The sensitivity to sour taste was found to be significantly reduced in pregnant women compared to nonpregnant women. This decreased sensitivity to sour taste may encourage or increase craving for food with sour taste, such as citrus, lemon, lime, and so on. These fruits are good sources of vitamins, minerals, and calories in pregnancy. Ingestion of sweet-sour fruit is beneficial to the health of both mothers and their unborn babies. The micronutrients in fruits (vitamins and minerals) will improve blood and immune status as well as help in proper body development. The difference in sour taste in pregnant women compared to controls supports the notion that pregnancy indeed has an effect on gustatory function.
The decreased bitter sensitivity reported among the pregnant women compared to nonpregnant women found in this study is similar to what had been reported in a few similar studies 26 –29 while a study had documented increased bitter sensitivity. 30 This decreased bitter sensitivity helps pregnant women to take in more nutritional meals like “bitter leave soup,” a local delicacy that has very good nutritional value for boosting blood levels and proper embryonic/fetal development. Some pregnant women get easily nauseated and pool saliva in the mouth which is irritating to their neighbors. Anecdotal report has shown that these symptoms are relieved by ingestion of “bitter kola” called Kolaviron. Bitter kola will be better tolerated by these pregnant women and benefit from its antioxidants and anti-inflammatory properties. 31 An increased sensitivity to bitter taste would increase the risk of hyperemesis which can be harmful to both mother and fetus. 32
The decrease in gustatory function in pregnancy had been explained by the need for increased intake of salt and calories, 8,24 changes in serum concentration of trace elements, 22,28 and changes in serum estrogen and progesterone levels. 7,28,33,34 Experimental studies on rat have demonstrated estrogen receptors in brain areas involved in gustatory processing, 35 and estrogen is known to affect gene expression within the central nervous system. 36 Electron microscopical scanning of the lingual papillae of pregnant rats showed difference in topographical configurations of these papillae as compared to that of nonpregnant rats. 37
Salt taste and total taste detection threshold were significantly higher on the left side than right side of the tongue in both pregnant and nonpregnant women. This depicts that the taste function in the left side of the tongue is better than that of the right half. There is no clinical explanation for this in this study. Nevertheless, a review of the functional neurology imaging of human cortical gustatory areas has shown significantly more peaks originating from the right brain hemisphere. This suggested asymmetrical cortical representation of taste thereby favoring the right hemisphere (small, human cortical gustatory areas). 38
The prevalence of hypogeusia was 2.9% in the pregnant women, and these pregnant women are approximately 5 times likely to develop hypogeusia than the nonpregnant women (Table 4). This supports the earlier report that taste function of women could change in pregnancy.
Conclusion
Although the taste detection threshold for sweet, sour, salt, and bitter for both pregnant and nonpregnant women were within the 10th percentile taste normative reference value, the higher values seen in the later is an evidence that pregnancy may have effect on gustatory function. There is an increased tendency for women to develop hypogeusia in pregnancy. It is therefore important to create awareness of possible change in gustatory function in pregnancy among women. In addition, they should be educated on how to manage it for better quality of life and optimal maternal nutrition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.