
Abstract
In the current value-based health-care environment, 30-day unplanned hospital readmissions have been identified as a quality measure and an opportunity to help reduce health-care costs. The LACE Index Scoring Tool for Risk Assessment of Death and Readmission utilizes length of stay, acuity of admission, comorbidities, and emergency department visits to stratify patients into high and low risk of readmission. A retrospective chart review of 161 patients who underwent a tracheotomy or laryngectomy for head and neck indications at a tertiary care academic center demonstrated that the readmitted patient cohort was not statistically or clinically different from the nonreadmitted cohort when comparing LACE scores (P = .789), length of hospital stay (P = .237), discharge disposition (P = .569), or insurance status (P = .85). Addressing the problem of unplanned 30-day readmissions will likely require enhanced patient education, improved coordination of care, and further research.
Introduction
In the current value-based health-care environment, 30-day unplanned hospital readmissions have been identified not only as a quality measure but also as an opportunity to help reduce health-care costs. 1 Historically, Medicare patients have had an unacceptable readmission rate of nearly 20%. 2 In an effort to encourage health systems to improve their readmission rates, the Center for Medicare & Medicaid Services reduces payments to hospitals with readmission rates that underperform relative to other hospitals within their comparable cohort. From the patient perspective, readmissions have also been found to contribute to a decreased quality of life and increased mortality. 3,4
Several metrics have been developed to help predict which patients are at increased risk of unplanned readmissions. 5 -8 One such tool is the LACE Index Scoring Tool for Risk Assessment of Death and Readmission. This tool uses length of stay, acuity of admission, comorbidities, and emergency department visits to stratify patients into high and low risk of readmission. 8 A large study conducted in the United Kingdom examined all-alive discharge adult inpatient episodes between January 2013 and December 2014 (approximately 90 000 patients) and showed that a LACE score of 11 was most effective at distinguishing higher and lower risk patients. 9 The efficacy of the LACE scoring system, however, remains controversial as a similar study conducted by Wang et al showed that the LACE scoring system did not accurately predict unplanned readmissions in patients admitted with acute congestive heart failure exacerbations. 10 To date, there have been no studies that have examined the utility of the LACE score among patients who have undergone tracheotomy or laryngectomy. This specific patient cohort represents a unique population that could be a target for reducing readmissions. Assessing the cause of readmission for purposes of readmission reduction has been a focus of ongoing quality improvement efforts in otolaryngology–head and neck surgery. 11 -14
Patient and Methods
The study protocol was approved by the institutional review board. A retrospective chart review of adult (>18 years of age) patients who underwent a tracheotomy or laryngectomy for head and neck indications between August 2016 and July 2017 at a tertiary care academic center was performed. Patients were classified into 2 cohorts based upon whether they had an unplanned hospital readmission within 30 days. Key variables that were collected included LACE score, length of hospital stay, insurance status, concurrent surgery, and discharge disposition. As our data were not normally distributed, Mann-Whitney U and χ2 tests were used to evaluate for statistical significance. Statistical tests were 2-tailed and considered significant at P < .05. Data analysis was conducted using SPSS software (IBM Corporation, New York).
Results
The study population was comprised of 161 patients who underwent a tracheotomy or laryngectomy. As noted in Table 1, 32 (19.8%) patients had an unplanned readmission within 30 days of surgery. The mean time to readmission was 7.5 days (range = 1-21 days) after discharge. The majority of patients in our cohort underwent a tracheotomy or laryngectomy as part of their planned cancer resection (n = 110, 68%) or for urgent upper airway obstruction (n = 42, 26%). As noted in Table 2, the majority of readmissions were secondary to concurrent surgical complications (n = 22, 68.7%) such as wound breakdown, infections, and fistulas, with only a minority being related to the tracheostomy (ie, shortness of breath or increased secretions; n = 5, 15.6%). Nearly all patients (n = 147, 91.3%) were discharged from the hospital with home health services or to rehabilitation facilities. Of note, the readmitted patients were not statistically or clinically different from the nonreadmitted cohort when comparing LACE scores (P = .789), length of hospital stay (P = .237), discharge disposition (P = .569), or insurance status (P = .85).
Comparison of Readmitted Versus Nonreadmitted Patients Who Underwent a Tracheotomy or Laryngectomy.a
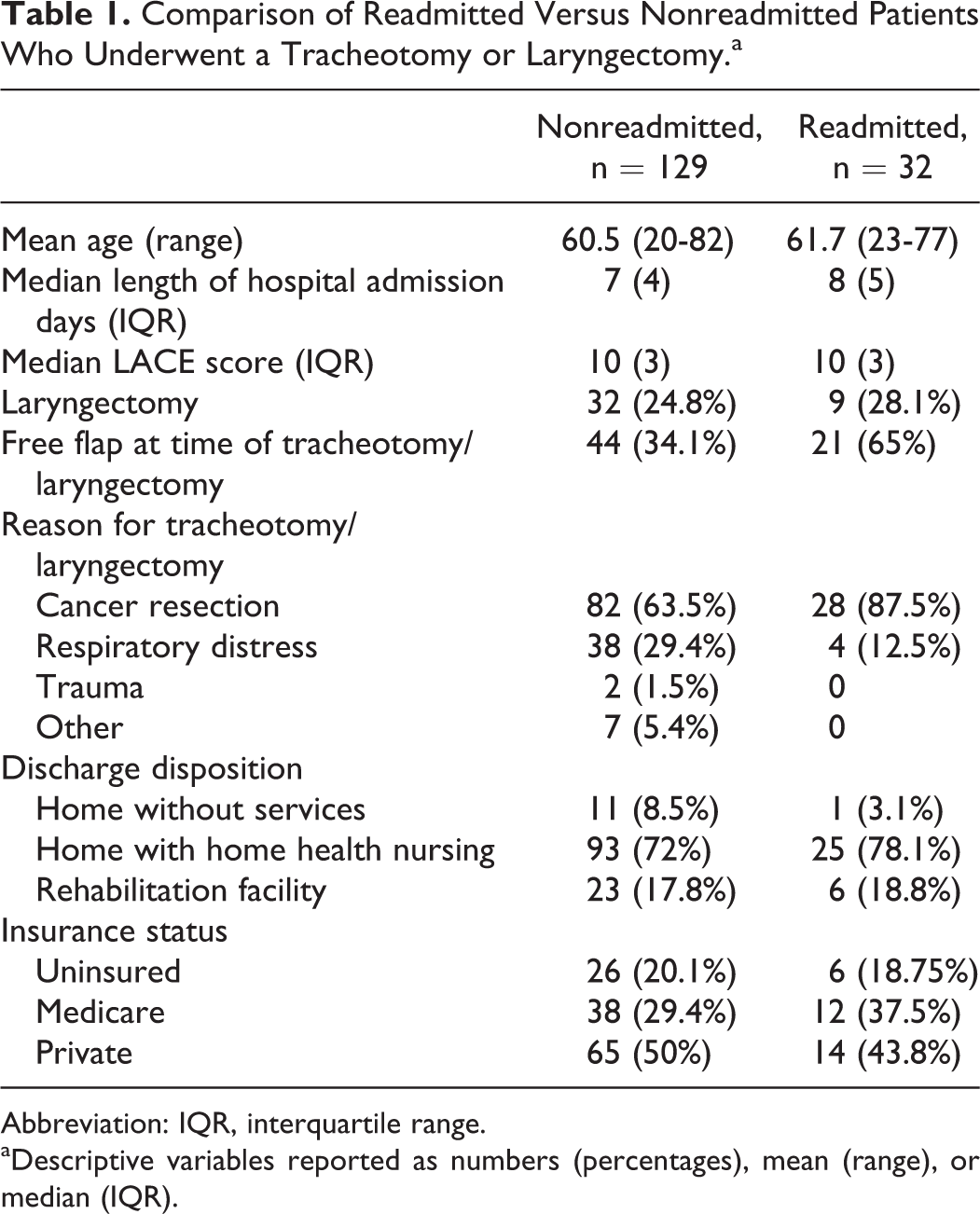
Abbreviation: IQR, interquartile range.
aDescriptive variables reported as numbers (percentages), mean (range), or median (IQR).
Readmission Population Data Set.a
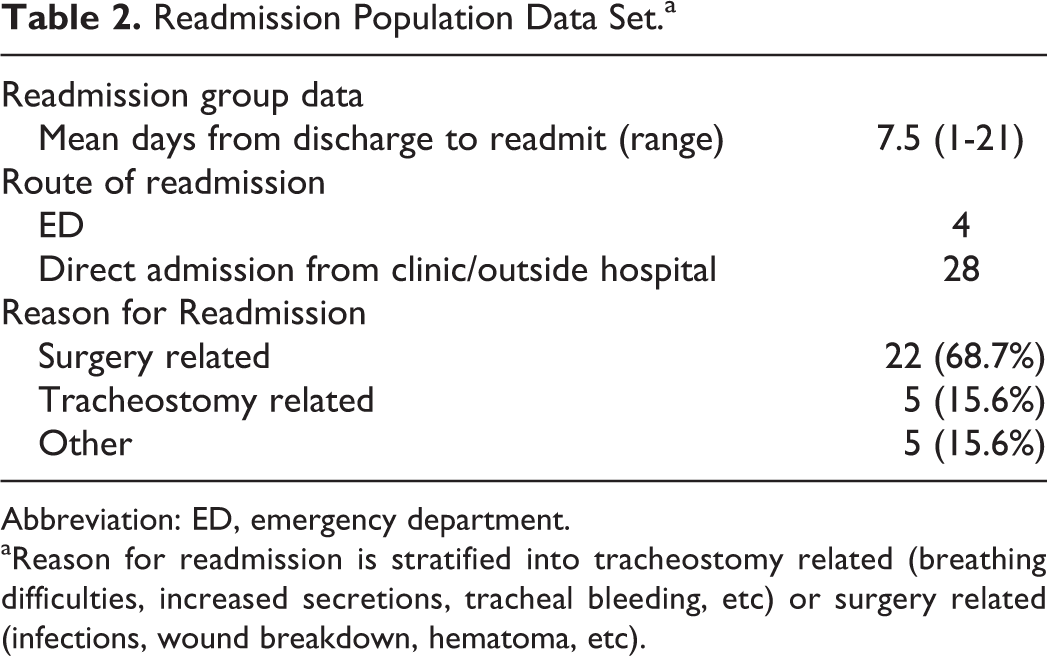
Abbreviation: ED, emergency department.
aReason for readmission is stratified into tracheostomy related (breathing difficulties, increased secretions, tracheal bleeding, etc) or surgery related (infections, wound breakdown, hematoma, etc).
Discussion
In our single-institution retrospective review of 30-day unplanned readmissions following tracheotomy or laryngectomy, we demonstrated that these patients are at high risk for readmission. Our readmission rate of 19.8% is comparable to previously published reports of readmission rates. 2,11 -13
The LACE score has been previously used to identify patients at increased risk of unplanned readmissions. 9 In our cohort, LACE scores were a poor predictor of readmission among patients who have undergone a tracheotomy or laryngectomy. We noted that in our population, the average LACE score of both groups (readmission and no readmission) was close to the previously published cutoff of 11 for high risk of readmission. 9 This finding may be an inherent limitation of the utility of the LACE score in patients with tracheotomy and laryngectomy. The LACE score evaluates length of stay, acuity of admission, comorbidities, and emergency department visits. Tracheotomy and laryngectomy patients typically score highly in these indices as they tend to have longer hospital stays with a higher overall acuity—especially at tertiary care academic medical centers. A similar finding was noted in the paper published by Wang et al, which found that LACE scores were poor predictors of readmission rates among patients with congestive heart failure. In their cohort, the average LACE score of the readmission versus no readmission group was 12.17 versus 11.80, respectively. Similar to our study, their patient group had relatively high baseline LACE scores that showed no correlation with readmission rates.
Overall, the readmitted cohort was not statistically or clinically different from the nonreadmitted cohort when comparing LACE scores (P = .789), length of hospital stay (P = .237), discharge disposition (P = .569), or insurance status (P = .85). The inability to risk stratify these patients based upon LACE score suggests that further research needs to be conducted to identify specific risk factors that could be applied to this patient population.
The limitations of the current study include the retrospective study design, relatively small sample size, limited ability to assess the patients’ cause for readmission, and reliance on clinical documentation for calculation of LACE scores. Another limitation of this study is that patients may be readmitted to an outside facility resulting in an underestimation of the rates of readmission.
Hospital readmission is a complex problem with a multifactorial etiology that disproportionately impacts tertiary care centers. 1 Addressing the problem of unplanned 30-day readmissions will likely require enhanced patient education, improved coordination of care, and further research. The development of additional targeted strategies to identify and intervene with patients who are at high risk for readmission will be necessary. The importance of studying and improving performance on this quality measure cannot be overstated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Barnes-Jewish Hospital Foundation (Grant #3144-36969).