
Abstract
Oral Cavity Spindle Cell Carcinoma (OCSCC) is a rare variant of squamous cell carcinoma involving the nasopharynx and oral mucosa. This tumor has a high propensity to invade local structures of the head and neck region, making surgical removal challenging and potentially morbid for the patient. Here, we report a case of OCSCC and the complications that were confronted during its surgical resection. Additionally, a review of the literature regarding OCSCC complications and their treatments was performed.
Introduction
Oral Cavity Spindle Cell Carcinoma (OCSCC) is a rare and rapidly progressive biphasic neoplasm that is a variant of squamous cell carcinoma. On histology, the neoplasm presents with epithelial squamous cells and mesenchymal spindle cells that commonly arise in the nasopharynx and oral mucosa. 1 Risk factors for developing OCSCC include alcohol use, tobacco use, poor oral hygiene, and previous irradiation to the head and neck region. 2 We now report a case of a 56-year-old female who presented with severe complications post-OCSCC resection surgery.
Case report
A 56-year-old female presented for evaluation for multiple recurrent Oral Cavity Spindle Cell Carcinomas (OCSCC). The patients’ therapy began at an outside hospital in 2011 with surgery (partial glossectomy and neck dissection) followed by chemoradiation for her squamous cell carcinoma. Subsequently, the patient had tumor recurrence of the squamous cell carcinoma and required a radial free flap, followed by chemotherapy and re-irradiation. The patient was placed on maintenance cetuximab from 2019 to 2021. She presented to the clinic in 2021 with a 10-day rapidly growing mouth mass (Figure 1A). The pathology confirmed a new spindle cell tumor presumed to be a late complication of the head and neck radiation from her prior treatment. The tumor was invading the mandible on imaging. Surgical resection, including a segmental mandibulectomy, and free flap reconstruction were recommended. (A) A 10-day rapidly growing mouth mass. (B) A 2.5 cm longitudinal laceration with possible mucosalization.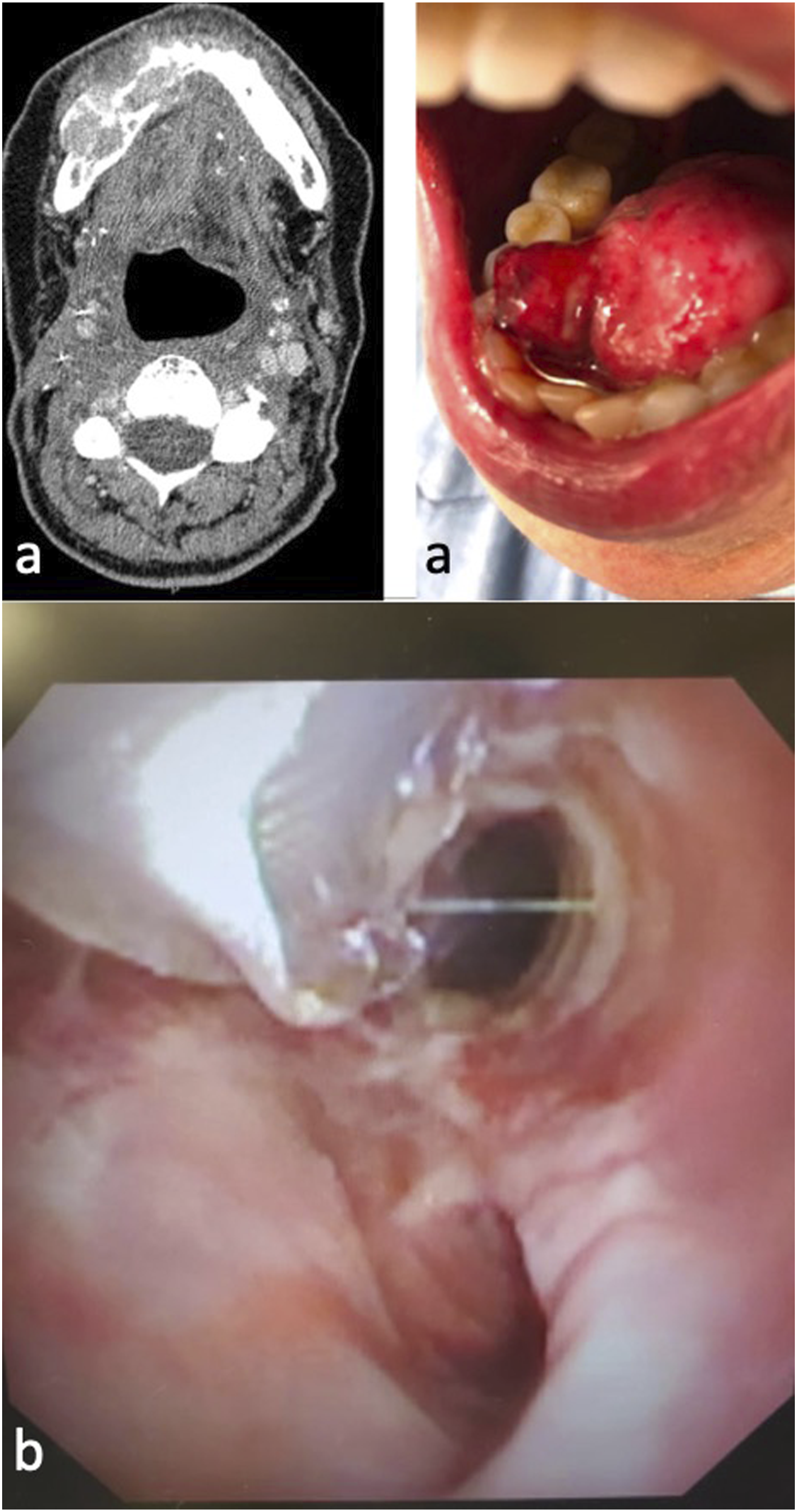
The surgical procedure included a tracheotomy, right oral composite resection with segmental mandibulectomy, and left fibula-free flap reconstruction with anastomoses to the left neck using the facial artery and facial vein. Intraoperatively the ablative surgeon used a midline lip incision to access the significantly scarred neck region and performed a wide local excision of the skin on the right neck and chin due to tumor invasion. The fibula-free flap was used to reconstruct the mandible, the floor of mouth/partial glossectomy defect, and the external neck skin defect.
After the procedure, a 7-5 armored endotracheal tube (ETT) was exchanged with an inner cannula (6 Shiley tracheostomy tube) under direct visualization. Chest rise was initially seen, but the patient had poor tidal volume with no EtCO2 detection. The tracheal tube was removed and replaced with the same armored ETT under direct visualization, but poor tidal volumes with no EtCO2 persisted. Thus, a bronchoscope was inserted into the tracheostomy incision for better visualization. The scope revealed a tear of the posterior tracheal wall and exposed lung parenchyma. The patient was transferred to the ICU with the endotracheal tube in place past the obstruction.
Upon arrival, a CXR revealed a pneumothorax with a mediastinal shift, pneumomediastinum, and pneumopericardium. The placement of a chest tube resolved the pneumothorax and hemodynamic instability. The patient returned to the operating room multiple times over the following week for evaluation of the tracheal wall injury. She remained sedated for most of this period in the ICU. The patient received intermittent pressors (norepinephrine) to tolerate the sedation and was NPO due to the need to return to the operating room multiple times. On postoperative day 3, the ETT was exchanged for an adjustable length Bivona. Flexible tracheoscopy revealed a healing 2.5 cm longitudinal laceration with early mucosalization (Figure 1B).
During the first postoperative week, the patient also had an intermittent fever, leukocytosis, and tachycardia despite broad-spectrum antibiotics and fluids, presumably a consequence of mediastinitis associated with the tracheal laceration. On postoperative day 7, a change in the fibula-free flap exam was noted. There was intermittent bleeding of the skin paddle upon scratch test, and no Doppler signal was able to be found (Figure 2A). On close examination, there was intraoral dehiscence on the posterior aspect of the flap along the remnant native tongue, which appeared frankly necrotic, resulting in a large fistula onto the vessels of the left neck. All three anastomoses were tenuous and not salvageable on two revision attempts in the operating room. Due to the patient’s surgical history and active neck infection, no further donor vessels could be identified. After 2 hours of ischemia, the flap was removed, and a left myocutaneous pectoralis major flap reconstruction was performed. (A) Intermittent bleeding of the skin paddle upon scratch test. (B) Healing of the tracheal laceration.
On postoperative day 15, the tracheal laceration showed healing with improvement in the patient’s leukocytosis and fever (Figure 2B). On postoperative day 18, the patient was decannulated with a stoma open to the air and was discharged two days later. On postoperative day 34, the patient presented with successful healing of the laceration and revision oral cavity reconstruction.
Discussion
Oral cavity spindle cell carcinoma is a highly invasive tumor that often invades the local structures in the head and neck regions. The primary treatment is wide local excision. Primary radiation is shown to be ineffective.3,4 Surgeries that involve large resections and reconstruction in the oral cavity often require the placement of a tracheotomy at the time of surgery to maintain a safe airway in the postoperative period. After the conclusion of these procedures, it is common practice to perform a tracheotomy tube exchange with a cuffed tracheotomy tube. 5 Tracheal exchanges are common procedures that occur post-operatively and should be given maximal precaution after any surgery. According to the study conducted by Asai et al, immediate tracheal extubation complications are significantly more common than intubation complications at a rate of 12.6% compared to 0.8%. 6 Early signs of tracheal lacerations include pneumoperitoneum, pneumomediastinum, displaced ETT, and subcutaneous air on chest CXR. 7 These early signs were seen in our patient, which prompted further exploration of the tracheal tube.
Additionally, tracheal lacerations are rare complications associated with endotracheal tubes that can result in high mortality. 8 According to a study conducted by Kaloud et al, risk factors for tracheal laceration may include advanced age, chronic steroid use, and inflammatory lesions. 9 In our patient, we believe that the tracheal injury occurred due to the patient’s prior radiation that compromised the tissue in the trachea, making it highly susceptible to tracheal laceration during tube exchange.
Moreover, according to Conti et al, conservative nonoperative management should be considered in patients breathing on their own due to a higher success rate than those treated surgically. 10 We found that in our patient, conservative management with close follow-up in the operating room led to the successful healing of the tracheal laceration. Thus, it is crucial to be aware of the complexity of a tracheal exchange and be vigilant after surgery due to the high risk of developing severe complications.
Surgical site infection after free tissue flap reconstruction of the head and neck is not uncommon. In a study examining 100 patients after free flap reconstruction in the oral cavity with standard antibiotic use, 21 of the patients developed head and neck wound infections. 11 If free tissue is unavailable, it is suggested that a pectoralis major flap is used for reconstruction in the head and neck region due to its reliability for defect reconstruction. According to a study that assessed 73 pectoralis major myocutaneous flap procedures, it was determined that the flap design, operative technique, and postoperative management significantly reduced the rate of complications. 12 Therefore, it is imperative for surgical teams to prepare for the possibility of tissue flap transfer infections by assessing the vasculature in the area and its postoperative management.
Conclusion
Wide surgical resection is the recommended primary treatment for OCSCC. Due to the tumor invasiveness of local structures, surgical complications are common and can result in significant patient morbidity. Hence, surgeons must be vigilant of the complications that may arise during and after tumor resections.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.