
Abstract

A 44-year-old woman was referred to the department of head and neck surgery for a 12-month history of decubitus dyspnea in the context of a painless mass of the right side of the neck, blocking the homolateral shoulder joint. Medical history reported the realization of a biopsy of the mass 4 months ago in Chechnya with a diagnosis of rhabdomyoma of the right side of the neck. The patient had never underwent other surgical procedures. Since then, the size of the mass continued to expand rapidly, leading to a recent decubitus dyspnea. The ear, nose, and throat examination revealed a very painful mass located in the right side of the posterior cervical area next to the cervical scar of the previous biopsy. The mobilization of the shoulder of the patient was very limited with regard to the pain and the mass effect. There was no neurological defect. Magnetic resonance imaging (MRI) showed an extensive tumor of the neck basis measuring 20 × 15 cm and infiltrating the nerve roots of the brachial plexus, the scalene muscles, the right carotid, the right phrenic nerve, and the adjacent adipose tissue (Figure 1). The chest X-ray found a right-side elevation of the right diaphragmatic cupola highlighting the paresis of the right side of the diaphragm. A fine-needle aspiration biopsy was performed but the result was noncontributory. Regarding the risk of malignancy, a debulking of the mass was performed with a frozen examination that could not found the histopathological nature of the lesion. Vascular and nerve structures have been conserved and there was no postoperative defect. The postsurgery histopathological examination of the mass revealed a desmoid-type fibromatosis of the neck (Figure 2). The reconstruction was made with a right pectoralis major musculomyocutaneous flap. Following the discussion of the oncological multidisciplinary group, patient received complementary radiation for the residual tissue. The 4-year follow-up was unremarkable.
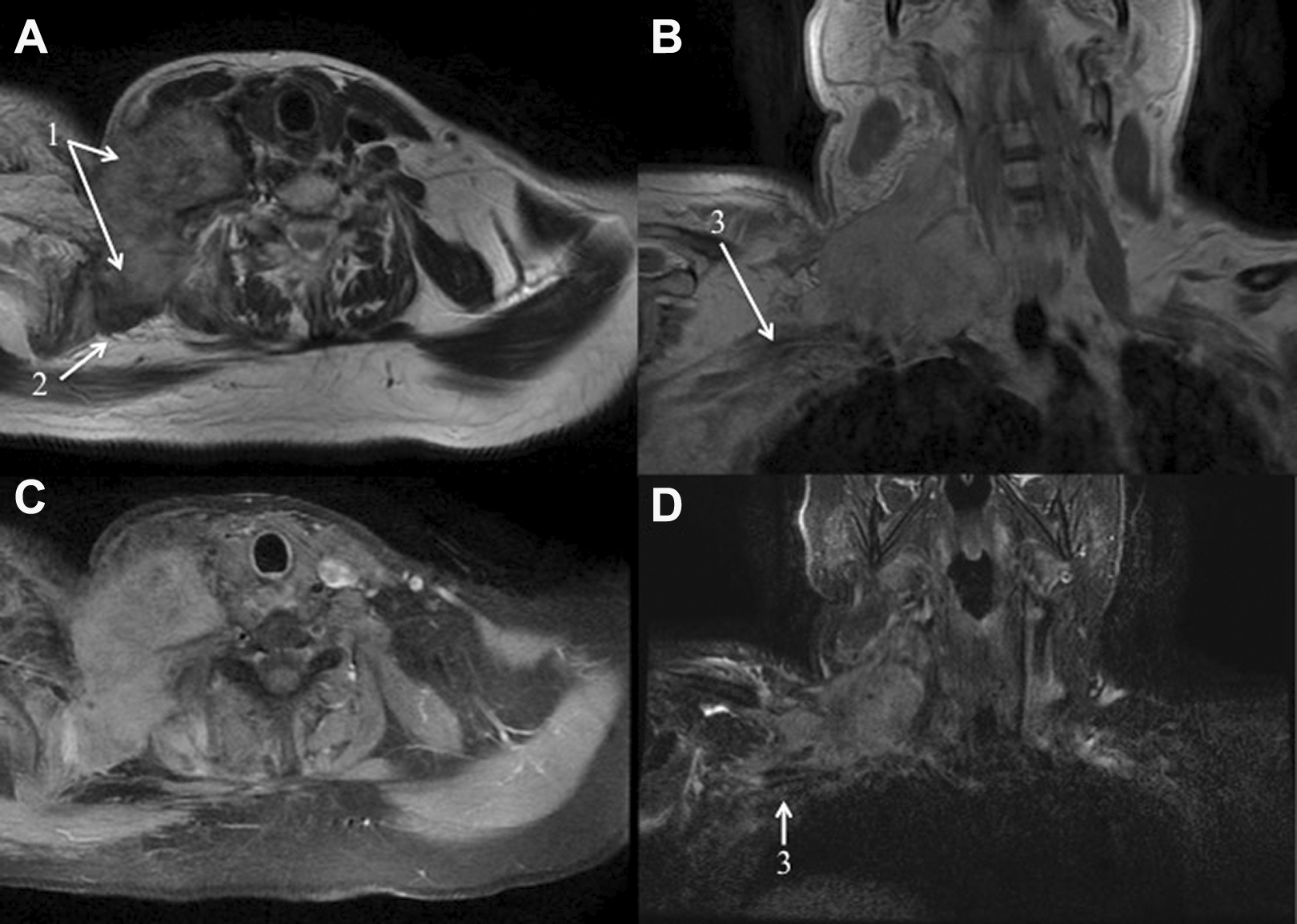
Magnetic resonance imaging of the lesion (sequences T1 [A and B] and T2 [C and D]). Magnetic resonance imaging showed a large tumor (1), infiltrating scalene muscles (2), brachial plexus (3), and into the mass, carotid artery, internal jugular vein, and phrenic nerve. Tumor appeared fleshy with an intense but inhomogeneous contrast enhancement and extended from clavicle (anteriorly) to the ventral face of the scalene muscle (posteriorly).
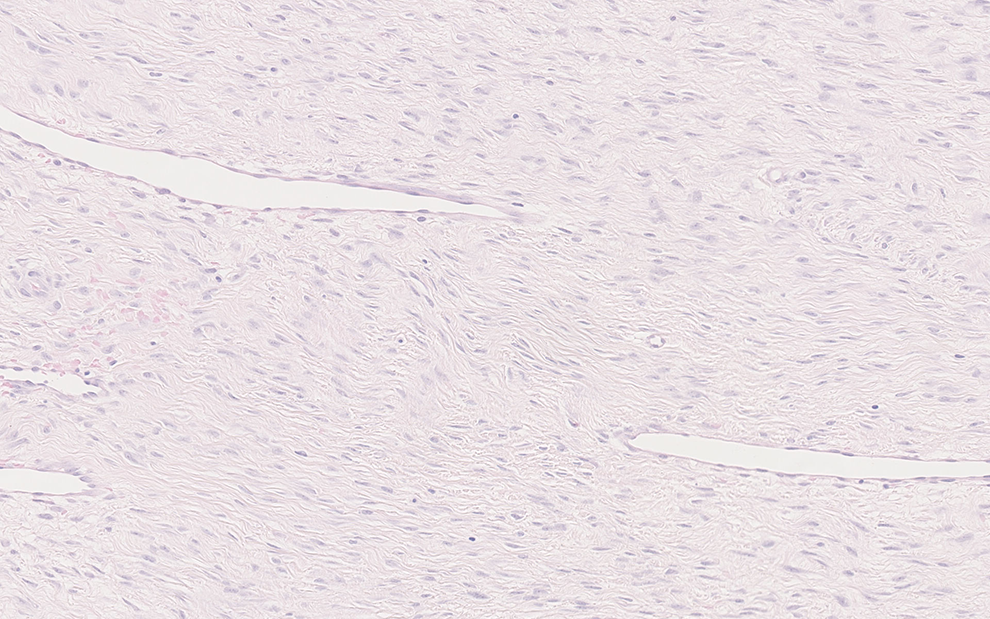
Histopathological findings. The hematoxylin and eosin staining (×200) reported a clonal myofibroblastic proliferation in a stromal tissue rich in collagen.
Desmoid-type fibromatosis represents 0.03% of all tumor with an incidence ranging from 2 to 4 individuals per million per year. 1 This rare mesenchymal tumor rarely occurs in head and neck area accounting for 7% to 15% of all desmoid tumors. 2,3 Etiology of desmoid tumors is little known, although it has been suggested that history of surgical trauma in tumor’s region has a key role. 4 Other more confidential researches identified sex hormonal environment of women in reproductive age as a risk factor. 5 The originality of our case is the lack of previous surgical trauma since, to our knowledge, all cases described in head and neck region were associated with a clear history of surgical trauma in the tumor area. 2,6 Regarding the age of the patient, the occurrence of the desmoid tumor in the present case could be associated with the hormonal environment of the patient. Clinically, desmoid lesions rapidly grow leading to pain and focal deficit 6 as described in our patient who developed pain and dyspnea related to invasion of the right phrenic nerve. The first step of the diagnostic still remains the imaging, especially MRI that commonly reveals soft tissue infiltration by the tumor and an inhomogeneous contrast enhancement. 7 The second step involves the histopathological identification, which is often complicated because of the rarity of the disease. 8 Treatment consists of surgical resection and, with regard to the high risk of recurrence (70%), 6 adjuvant chemotherapy or radiotherapy. 9 Our patient had no recurrence 5 years after the end of the radiotherapy.
Footnotes
Authors’ Note
Didier Dequanter and Alexandra Rodriguez contributed equally to this work and should be regarded as joint last authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.