
Abstract

Castleman disease (CD), first described in 1956, is a rare, lymphoproliferative disease characterized by benign, localized enlargement of lymph nodes. 1,2 It most commonly presents as a solitary mass with a benign course, known as the localized type. Castleman disease of the head and neck in the pediatric population is rare, with only 32 reported cases in the literature. 3 –6 The authors report the 33rd pediatric case presenting as a supraclavicular mass in a child.
A 10-year-old female presented to our department with a 4-month history of an enlarging, right-sided neck mass. This mass was painless and did not arise in the setting of an infection. She had no history of clinical symptoms, such as fever, malaise, night sweats, or weight loss. On physical examination, there was a soft, nontender, mobile, right supraclavicular mass measuring approximately 4 cm × 2 cm in size. There were no overlying skin changes. The remainder of the physical examination was normal. Laboratory testing revealed a normal white blood cell count with elevated lymphocytes, positive Epstein Barr virus, early immunoglobulin G, and elevated copper. Bartonella and cytomegalovirus testing was negative.
The workup proceeded with a neck ultrasound which showed a 4.0 cm × 1.4 cm solid, right supraclavicular nodule with internal vascularity and well-defined borders, concerning for an abnormal lymph node. A computed tomography (CT) scan of the neck showed an oval-shaped, mildly heterogeneous, enhancing soft tissue mass with well-defined borders measuring 2.5 cm × 3.9 cm × 3.4 cm (Figure 1, red arrow). The mass mildly displaced the surrounding structures without clear invasion.
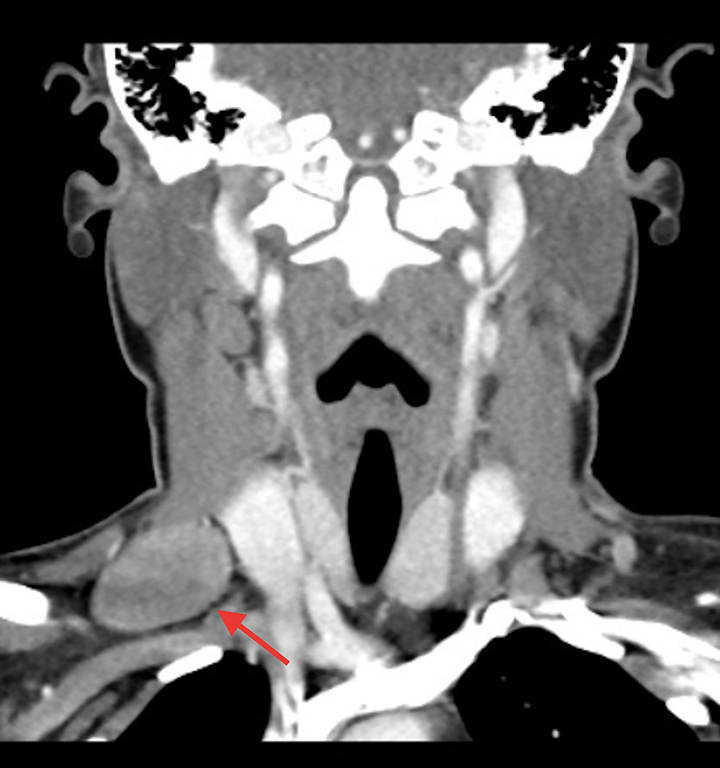
Computed tomography scan of the neck showing an oval-shaped, mildly heterogeneous, enhancing soft tissue mass with well-defined borders measuring 2.5 cm × 3.9 cm × 3.4 cm (red arrow).
The patient underwent excision of the mass with nerve monitoring. Intraoperatively, the mass was noted to be a lymph node and it was completely excised. Pathology review revealed an enlarged lymph node with follicular hyperplasia, small germinal centers, and prominent mantle zones with penetrating “onion-skinning” vessels with a “lollipop” appearance and marked vascular proliferation (Figure 2, black arrow). Atypical dendritic cells were seen within and outside the follicles which were CD21 positive and negative for CD30, CD15, and CD20. There were focal areas of marked fibrosis without necrosis. Flow cytometry showed no immunophenotypically abnormal cell populations. These morphological features favored the diagnosis of hyaline-vascular type CD. The patient recovered well postoperatively without any further lymphadenopathy or recurrence.
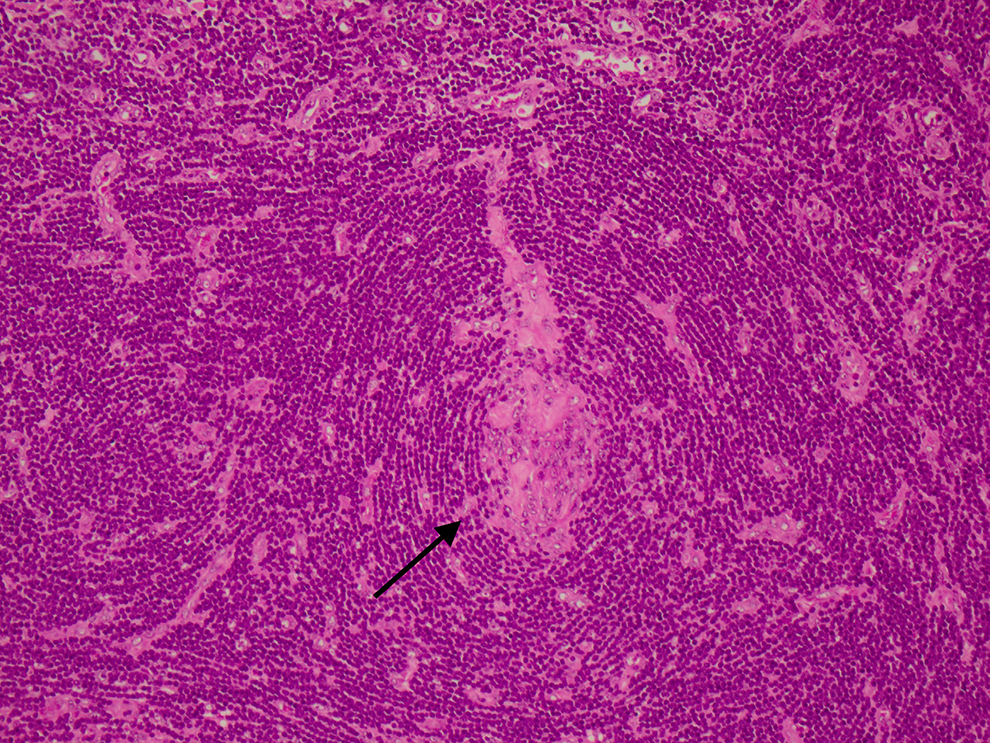
Lymph node showing follicular hyperplasia, small germinal centers, and prominent mantle zones with penetrating “onion-skinning” vessels with a “lollipop” appearance (black arrow).
Most individuals affected by CD are young to middle-aged, with males and females equally affected. 1 Castleman disease can be subcategorized by morphology (unicentric vs multicentric) or histology (hyaline-vascular, plasma-cell, or mixed type). 3 Most cases are asymptomatic, unicentric, and hyaline-vascular tissue type. The etiology of CD is believed to involve the overproduction of cytokine interleukin 6, which has been shown to increase the proliferation and survival of B cells. 1 Additionally, follicular dendritic cell abnormalities and vascular endothelial growth factors have shown to contribute to the development of the unicentric form. Human herpesvirus-8 has also been a proposed etiology. 3 The classic pattern will be follicular hyperplasia, transformed geminal centers, expanded mantle zones with an “onion-skin” pattern, and vascular proliferation with a lollipop formation. CD21-positive follicular dendritic cells can be seen. 4,5
Pediatric CD is known to be a rare entity. Although rare, it is important to include CD in the differential diagnosis of a pediatric neck mass. The largest study looking at pediatric CD in the neck was a review article involving 18 studies, which included 29 patients. 3 Subsequently, there have been 3 additional reported cases which displayed similar features. 4 –6
Our patient’s presentation was consistent with previously reported literature. The unique aspect of this case was its location in the supraclavicular region. Our patient underwent both CT scan and ultrasound, which aided in surgical planning but was largely nonspecific from a diagnostic standpoint. Similar to already reported cases, laboratory testing did not dictate the diagnosis or management of our patient. The patient underwent excision which revealed typical pathologic features of hyaline-vascular type CD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.