
Abstract

A 68-year-old man presented with frequent epistaxis and a severe foul odor from the nasal cavity. His symptoms began about 2 months ago. Previous history of facial trauma or nasal surgery was absent. However, he had a medical condition of myelodysplastic syndrome and visited the hemato-oncology department regularly.
Endoscopic examinations demonstrated blood clots in the nasal cavity, and a marked crust, necrotic changes, and septal perforation were observed after removing the clots (Figure 1). Nasal discharge was scanty, and the culture revealed no growth of bacterial organisms. We suspected a midline destructive lesion, such as Wegener granulomatosis, and biopsied the septum. Laboratory tests, including c- and p-antineutrophil cytoplasmic autoantibody (ANCA), were also performed. However, the biopsy showed chronic inflammation with aspergillosis hyphae and c- and p-ANCA were negative.
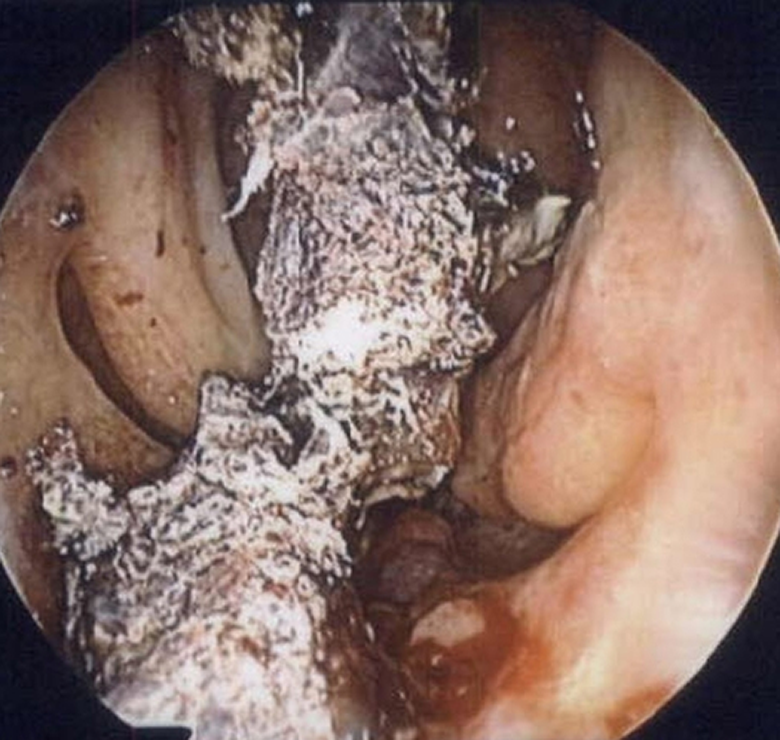
Endoscopic findings show marked crust, necrotic changes, and septal perforation.
We recommended partial septectomy and debridement for tissue diagnosis and treatment, but the hemato-oncologist did not allow the procedure due to its high morbidity (hemoglobin 6.3 g/dL, hematocrit 16.9%, and platelets 2000/μL). We decided to remove the necrotic portion of the septum periodically in the office, and the removed septum was sent for repeated histological examinations. The procedure was performed once a week for a month and thereafter twice a month. It took about 8 months to remove the entire septum, and the pathology was the same as initially. His nasal cavity became a single common space (Figure 2) with clean mucosa without crusts, and epistaxis and foul odor disappeared. He is followed in the office regularly without nasal discomforts.
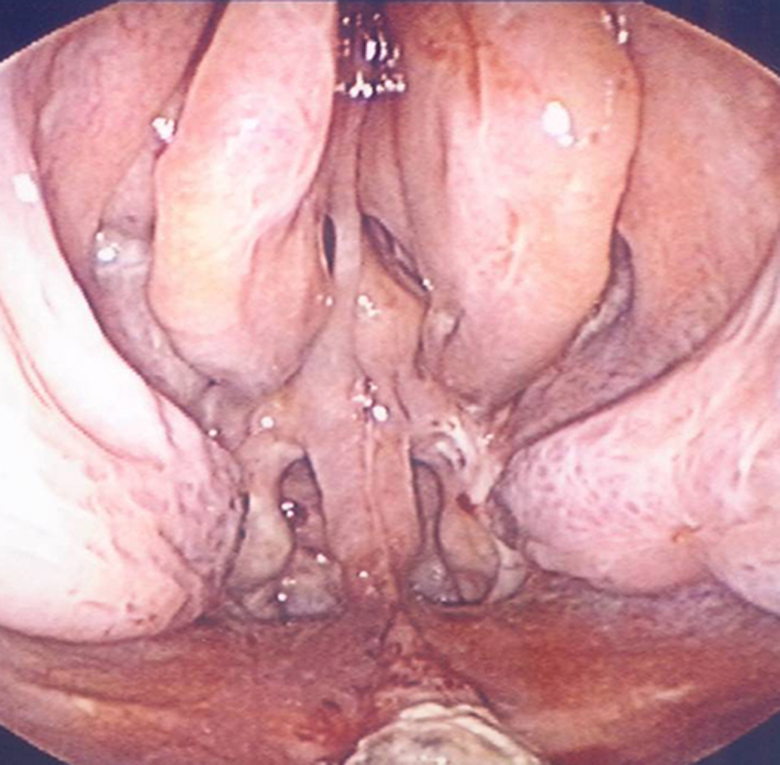
Clearly healed common nasal cavity after 8-month debridement and treatment.
Common reasons for septal perforation include nasal surgery, trauma, electrocautery, cocaine abuse, and topical nasal spray. 1 In addition, there are several reports that septal perforation occurred by invasive fungal sinusitis. 2 However, this patient does not correspond to any causes mentioned above. We postulate that immunocompromised state due to myelodysplastic syndrome lead to initial necrosis of the nasal septum, compromised blood supply, fungal infection, and disruption of the self-healing mechanism. Fortunately, further bacterial or invasive fungal infection did not occur, and he recovered without any additional interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Soonchunhyang University Research Fund. This material has never been published and is not currently under evaluation in any other peer-reviewed publication.