
Abstract
Inflammatory pseudotumor (IPT) is a rare, locally aggressive, benign neoplasm of unknown etiology. It is uncommon in the head and neck region, particularly in the paranasal sinuses. We present an unusual case of IPT of the maxillary sinus and orbit in a 27-year-old woman who presented with cheek swelling, right orbital swelling, double vision, and associated fever and trismus. Computed tomography identified a mass with radiologic features suggestive of a malignancy of the maxillary sinus and orbit; the mass extended into the infratemporal fossa, parapharyngeal space, anterior antral wall, and surrounding soft tissue. A diagnosis of IPT was established on the basis of histologic and immunohistochemical analysis, which identified a proliferation of bland spindle cells and a mixed inflammatory cell infiltrate. Despite its aggressive appearance, IPT is associated with a good prognosis. Our patient was treated successfully with a combination of surgery, steroid therapy, and methotrexate. Chemotherapeutic agents are generally reserved for recalcitrant cases.
Introduction
Inflammatory pseudotumor (IPT) is a rare, locally aggressive, benign neoplasm of unknown etiology. This lesion is also known as a, plasma cell granuloma, myofibroblastoma, inflammatory myofibroblastic tumor, and xanthomatous pseudotumor, and it occurs as the result of an inflammatory myofibroblastic proliferation and a pseudosarcomatous fibroinflammatory process. 1 The various terms used to describe this lesion reflect the uncertainty of its pathogenesis and the variety of its histologic appearances. Several authors have suggested the possibility that IPTs are caused by infection with Epstein-Barr virus 2 or human herpesvirus-8. 3 Histologically, IPTs are characterized by a proliferation of bland spindle cells and a mixed inflammatory cell infiltrate.4–6
IPTs were originally described as a nonneoplastic lesion in the lung, but they appear in extrapulmonary sites as well, including the abdomen, retroperitoneum, extremities, and central nervous system. 7 IPTs of the head and neck region are uncommon.5,6 We report an unusual case of an aggressive IPT that involved the maxillary sinus and orbit.
Case Report
A 27-year-old Malaysian woman presented with a 2-month history of progressive right cheek swelling, right orbital swelling, double vision, and associated fever and trismus. The patient had no history of relevant trauma, nasal surgery, or dental surgery. Clinical examination demonstrated swelling of her right cheek and temporal area, right proptosis, right hypertropia, and limited mouth opening. Rhinoscopy revealed a distortion of the right lateral nasal wall.
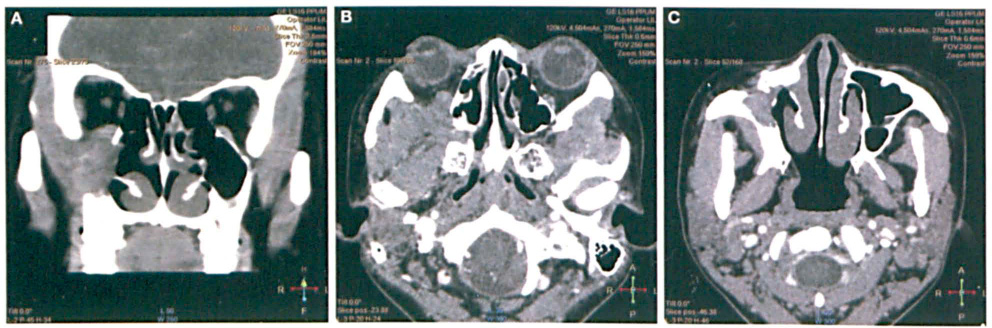
The patients biochemical and hematologic profiles were normal with the exception of an elevated erythrocyte sedimentation rate (140 mm/hr; normal: <20), an elevated C-reactive protein level (1.4 mg/dl; normal: <0.3), mild anemia, and thrombocytosis. The results of the C-antineutrophil cytoplasmic antibody (C-ANCA) test, Mantoux test, and chest x-ray were normal. Computed tomography (CT) revealed that an ill-defined soft-tissue mass with minimal enhancement was occupying the right maxillary sinus (figure 1). The mass had invaded the cheek anteriorly, the orbit superiorly, and the infratemporal fossa and parapharyngeal space posterolaterally.
Surgery with general anesthesia was performed via an endonasal endoscopic approach. The tumor was found to be arising from the right maxillary antrum, and it extended medially to involve the middle meatus, the anterior ethmoid air cells, and the inferior turbinate. A right uncinectomy, middle meatal antrostomy, and anterior ethmoidectomy were performed. A specimen was obtained for histopathology, and the tumor was debulked.
Histology identified a collagenous stroma composed of fascicles of spindle-shaped cells. This stroma was densely infiltrated by an admixture of inflammatory cells made up of lymphocytes, plasma cells, histiocytes, neutrophils, and occasional eosinophils (figure 2). Smooth-muscle actin was positive on immunohistochemistry, confirming the myofibroblastic nature of the spindle cells. Further immunohistochemical analysis was negative for neoplastic epithelial elements. Gomori methenamine silver staining, periodic acid–Schiff staining, and Ziehl-Neelsen staining were negative for infective microorganisms. These histologic findings were most consistent with an IPT.

Photomicrograph shows a section of the lesion that is made up mainly of
plasma cells (), lymphocytes
( ),
neutrophils (➘), and eosinophils (
),
neutrophils (➘), and eosinophils ( ) (hematoxylin and
eosin, original magnification x200).
) (hematoxylin and
eosin, original magnification x200).
On the basis of the histologic and immunohistochemical findings, the patient was started on a course of steroids. Although the steroids alleviated some of her signs and symptoms, the lesion persisted, which resulted in continued diplopia. She was then started on methotrexate, which subsequently led to the resolution of all symptoms.
Discussion
According to the World Health Organizations classification system, IPT is a neoplasm in the intermediate (rarely metastasizing) category. 8 In children, IPTs are quite often characterized by anaplastic lymphoma kinase-1 (ALK-1) gene rearrangements. They are locally invasive and they may recur, but they do not often metastasize (∼5% of cases). 8 While they are uncommon in the head and neck region, IPTs have a predilection for the orbit and less frequently the oral cavity and paranasal sinuses. 9
We have reported a new case of an aggressive IPT that involved the maxillary sinus and orbit with extension into the infratemporal fossa, parapharyngeal space, anterior antral wall, and surrounding soft tissue. Authors who have described some previous cases have reported that the age range of affected patients is wide (6 to 83 years; median: 47.0) and that there is a slight female preponderance (male-to-female ratio: 2:3). 10 The most common signs and symptoms are cheek swelling, nasal obstruction, and epistaxis. The course of an IPT can be acute or subacute, but at presentation, these lesions tend to mimic a malignant process clinically and radiologically. IPTs of the maxillary sinus cause bone changes on CT that mimic a malignant tumor.11,12
Based on the histologic and immunohistochemical findings, our patient was started on a course of steroids. However, this proved to be inadequate, and she later required methotrexate. Other chemotherapeutic agents, such as cyclophosphamide and cyclosporine, may be used in patients who do not respond to steroid therapy. 13
Although our patient was successfully treated with a combination of surgery, steroids, and chemotherapy, the treatment of IPT remains controversial. Based on our literature review, we believe that most clinicians would recommend a trial of systemic steroid therapy. If there is little or no response to the steroid, local resection is advocated, even if the lesion cannot be completely removed. In the event of a recurrence, radical resection is recommended because some of these tumors exhibit very malignant behavior. 14 The role of radiotherapy is controversial; most authors recommend it if surgery or steroid therapy is contraindicated or unsuccessful. 15
Despite the aggressive appearance of IPT, patients have a good prognosis. It is important for clinicians to work closely with an experienced pathologist since IPTs tend to mimic a malignant process.