
Abstract
We describe a very rare case of tuberculous otitis media (TOM) with direct intracranial extension. The patient was a 55-year-old man who presented to our ENT clinic for evaluation of severe headaches and right-sided otorrhea. A biopsy of granulation tissue obtained from the right external auditory canal demonstrated chronic inflammation that was suggestive of mycobacterial infection. Magnetic resonance imaging of the brain indicated intracranial extension of TOM through a destroyed tegmen mastoideum. After 2 months of antituberculous medication, the headaches and otorrhea were controlled, and the swelling in the external ear canal subsided greatly. Rarely does TOM spread intracranially. In most such cases, intracranial extension of tuberculosis occurs as the result of hematogenous or lymphogenous spread. In rare cases, direct spread through destroyed bone can occur, as it did in our patient.
Introduction
Tuberculous otitis media (TOM) is rare in developed countries; it accounts for only 0.06% of all cases of suppurative otitis media. 1 Although the prevalence of tuberculosis has decreased in South Korea during the past decade, it remains a serious public health problem. In 2007, the incidence of tuberculosis in South Korea was 71.6 per 100,000 population; of these, there were only 4 cases of TOM. 2
The diagnosis of TOM is difficult and therefore often delayed because of its rarity, its variable clinical manifestations, and frequently false-negative results of cultures and laboratory tests.3,4 Delayed diagnosis and treatment may have serious consequences. As a rare consequence, TOM may spread intracranially. In most such cases, the intracranial extension of tuberculosis is a result of hematogenous and lymphogenous spread rather than direct extension.5,6
In this article, we report a very rare case of TOM with intracranial spread that occurred as a result of the direct extension of tuberculosis, and we review the relevant literature.
Case Report
A 55-year-old man presented to our ENT clinic for evaluation of severe headaches and right-sided otorrhea. The otorrhea and associated ear fullness had begun approximately 1 year earlier. At that time, the patient was treated for external otitis at a local clinic, but his symptoms did not resolve. His headaches and accompanying nausea developed 10 months later.
The physical examination revealed a narrow external auditory canal (EAC) caused by bulging of the posterior wall. A small amount of granulation tissue was seen in the lateral portion of the posterior wall. On otoscopy, only the inferior part of the tympanic membrane could be seen through the narrowed EAC; the tympanic membrane also had a bulging appearance. Laboratory tests, including a complete blood count and a blood chemistry panel, detected no abnormality except for an increase in the erythrocyte sedimentation rate (26 mm/hr). The chest radiograph was normal.
Pathologic examination of granulation tissue obtained from the ear canal revealed chronic inflammation with multinucleated giant cells, which suggested a mycobacterial infection (figure 1). A Ziehl-Neelsen stain of the granulation tissue and a polymerase chain reaction (PCR) examination of the otorrhea found no further evidence of mycobacterial infection.
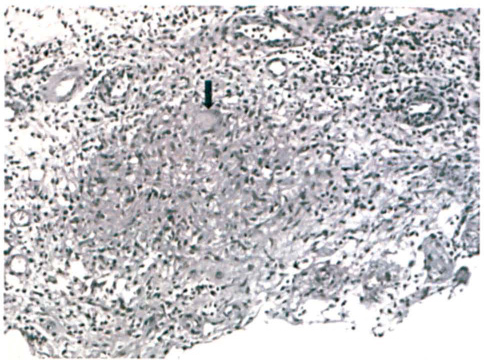
Microphotograph of the material obtained from the right EAC shows the chronic granulomatous inflammation and a multinucleated giant cell (arrow) (hematoxylin and eosin, original magnification ×200).
Since the patient complained of worsening headaches and nausea, we obtained magnetic resonance imaging (MRI) of the brain to look for any intracranial extension of tuberculosis (figure 2). MRI showed that the middle ear, mastoid cavity, and EAC were filled with a heterogeneously enhancing soft-tissue density. Moreover, the tegmen mastoideum was destroyed and the meninges of the right temporal lobe and cerebellum were thickened and enhanced by contrast. In addition, several small, round, strongly enhanced lesions with a central hypointense signal were seen in the right temporal lobe and cerebellum along with perilesional edema; these lesions were thought to represent tuberculomas.
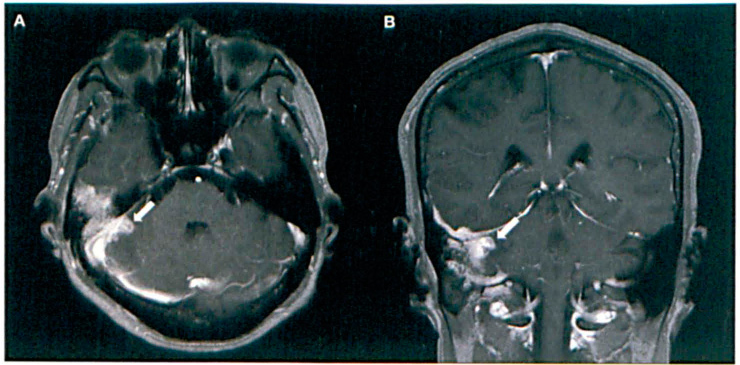
T1-weighted postcontrast axial (
Although mycobacterial infection could not be confirmed by PCR assay and Ziehl-Neelsen staining, we took into consideration the high incidence of mycobacterial infection in South Korea and we started the patient on antituberculous medication with a four-drug combination: rifampicin, isoniazid, pyrazinamide, and ethambutol. After 2 months of this regimen, his headaches and otorrhea were controlled and the swelling of the EAC had subsided greatly. The patient was maintained on medication as an outpatient.
Discussion
TOM can occur in three ways: by spread to the middle ear through the eustachian tube, by hematogenous spread from another tuberculous focus, and by direct implantation through the EAC and a tympanic membrane perforation. Approximately 40 to 50% of patients with TOM do not exhibit other tuberculous findings elsewhere in the body. 4 The prevalence of TOM is higher among children than adults, and it occurs more frequently in males than females. 4
As mentioned, the diagnosis of TOM is difficult and therefore typically delayed. Its classic manifestations are painless otorrhea with multiple tympanic membrane perforations, exuberant granulation, early severe hearing loss, and bone necrosis. However, some patients do not exhibit these classic features, and other signs and symptoms are variable. For example, Cho et al reported that otalgia was not rare (13.5% of cases); on the other hand, they found multiple tympanic membrane perforations in only 1 of 52 patients with TOM. 3 Vaamonde et al observed similar features of TOM: relatively frequent otalgia (30% of cases) and a paucity of multiple perforations (10%). 4
The most interesting feature of our case was the direct intracranial extension. The incidence of secondary meningitis, which is associated with TOM, is low, and hematogenous and lymphogenous spread have been implicated more often than direct extension from the mastoid cavity.5,6 Tuberculoma or abscess formation associated with TOM is rarer, as only a few cases have been reported. 5 The most common sites of tuberculous meningitis are the sylvian fissure, the chiasmatic cistern, and the perimesencephalic cistern. 7 Unlike previously reported cases, in our patient the meninges above the destroyed tegmen mastoideum was thickened and enhanced by contrast, and several small, round, enhancing lesions with perilesional edema were seen nearby. This finding suggested direct intracranial extension rather than hematogenous spread.
The treatment options for TOM include antituberculous chemotherapy and surgery. The current indications for surgical intervention are to obtain histologic material for diagnosis, drainage of a subperiosteal abscess, removal of sequestra and, according to some authors, decompression of the facial nerve. 8 However, the role of surgery in the treatment of TOM has obviously declined markedly since the introduction of antituberculous chemotherapy, the results of which are excellent. 3
The two major problem areas in our case were the tuberculous meningitis and intracranial tuberculomas. The chemotherapeutic regimen for the treatment of tuberculous meningitis is divided into two phases: an intensive initial phase and a continuation phase. 9 During the intensive phase, which usually spans 2 months, the regimen includes a combination of four first-line drugs: rifampicin, isoniazid, pyrazinamide, and streptomycin. The continuation phase, which lasts for 7 to 10 months, includes only rifampicin and isoniazid. 9 Corticosteroids are strongly recommended for the treatment of tuberculous meningitis. 10 They significantly reduce mortality and neurologic deficits.
From a surgical perspective, cerebrospinal fluid diversion procedures are often used in patients who have tuberculous meningitis with hydrocephalus. Despite these efforts, the prognosis for patients with tuberculous meningitis is very poor, as antituberculous treatment prevents death or disability in less than 50% of patients. 9 Early diagnosis and treatment are important for a better prognosis, and the routine use of corticosteroids is strongly recommended.