
Abstract
Pleomorphic adenoma is rare in pediatric populations, where viral and congenital problems are the usual culprits responsible for submandibular masses. We report the case of a 12-year-old child who presented with a painless right submandibular mass that had developed over the course of 4 months. The patient denied fever, erythema, and edema. The mass was diagnosed as a branchial cleft cyst before complete excision was performed. The pattern and etiology of a pleomorphic adenoma in children differs from those in adults. In children, it requires prompt and correct diagnosis to keep morbidity and mortality at a minimum.
Introduction
Less than 5% of all salivary gland tumors occur in children; these tumors are approximately 10 times more likely to take place in the parotid gland than in the submandibular gland.1–9 Pleomorphic adenomas, also called mixed tumors for their remarkable histologic diversity, represent about 60% of all tumors in the parotid gland; however, like all salivary gland tumors, they are far less common in the submandibular gland. 6 When pleomorphic adenomas do occur, 85% of the time they will occur in the parotid gland, 4 to 8% in the submandibular gland, and approximately 7% in the minor salivary glands.4,5
The literature has demonstrated the occurrence of pleomorphic adenomas in the pediatric population, although they occur in this group rarely. 7 It is more common to see them between the fourth and sixth decades of life, with the typical age at presentation being approximately 43 years. 8 Multiple sources have shown that the occurrence of salivary gland tumors, including pleomorphic adenomas in children ≤18 years of age, ranges from 4.3 to 11.2%.2,3
The diagnosis of a submandibular pleomorphic adenoma can be difficult in children. Clinicians will first rule out more common causes of neck masses, such as viral lymphadenopathy, acute or chronic sialadenitis, secondary inflammation in sialolithiasis, congenital anomalies, and the various benign and malignant neoplasms. This article describes the rare occurrence of a submandibular pleomorphic adenoma in a pediatric patient.
Case Report
A 12-year-old boy was referred by his pediatrician for a right-sided neck mass located in the submandibular triangle. The mass was painless and had grown over the course of 4 months. It caused no other symptoms. The patient had not experienced fever, erythema, edema, dyspnea, or trauma to the neck, and had no significant medical or surgical history. He was not on any medication and was allergic to artificial sweeteners. Moreover, there was no family history of neck masses.
On examination, the patient was afebrile, hemodynamically stable, and in no acute distress. A right-sided, round, well-demarcated, smooth submandibular mass was found on palpation. It was partially mobile, hard, rubbery, and nontender. The mass was only partially palpable because approximately half of its circumference was too deep to palpate. Contrast-enhanced computed tomography (CT) of the neck showed a large, low-density, well-defined mass in the right submandibular triangle extending posteriorly and superiorly to the body of the mandible and measuring 4.5 cm × 3 cm × 3 cm (figure 1).
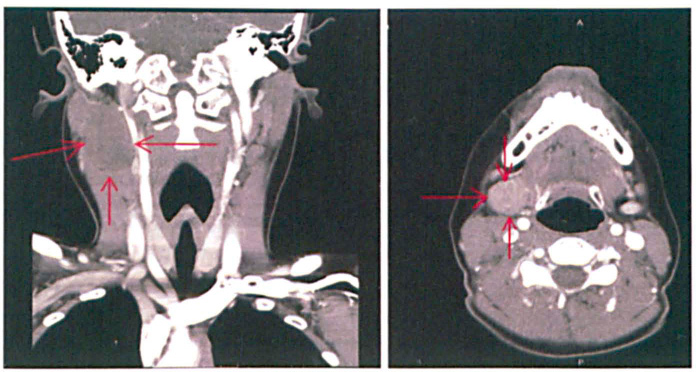
Contrast-enhanced CT scans of the neck show a large low-density, well-defined mass (arrows) in the right submandibular triangle extending posteriorly and superiorly to the body of the mandible and measuring 4.5 × 3 × 3 cm.
Examination and CT findings led us to suspect a branchial cleftcyst. The options were discussed with the patient and the family, who opted for surgery. The patient was operated on via the submandibular approach (figure 2). The tumor was bound anteriorly by the anterior digastric muscle and posteriorly by the sternocleidomastoid muscle and retromandibular fossa. The superior boundary was the angle of the mandible. The lesion was directed medially and deep toward the hyoid bone. Upon removal, a 4.0 × 4.0 × 3.5-cm multinodular mass weighing 26 g was observed (figure 3).
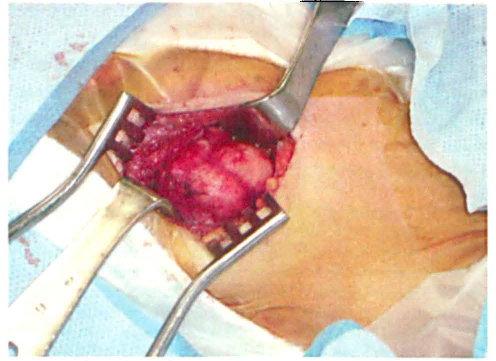
Photo shows the intraoperative view via the submandibular approach prior to tumor removal.

The resected multinodular tumor measures 4.0 × 4.0 × 3.5 cm and weighs 26 g.
The transected gross specimen was a yellow mass with a surrounding thick capsule. The encapsulated mass was composed of bland epithelial cells that formed a few branching ducts and small acinar clusters surrounded by a chondromyxoid stroma (figure 4). After histopathologic review, a diagnosis of pleomorphic adenoma was rendered. Although a pleomorphic adenoma is rare in this anatomic location and in this age group, the lesion displayed typical histopathologic features. In addition, the clinical history allowed for a definitive diagnosis without referral to an external authority on pediatric tumors.
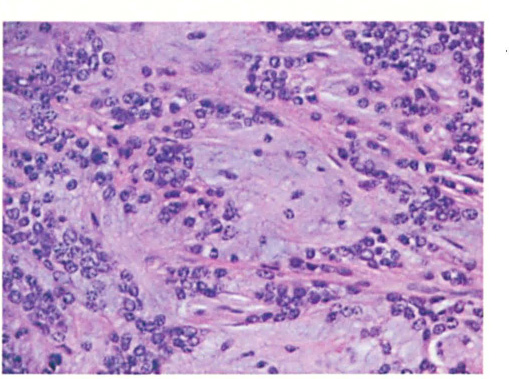
Histopathology reveals that the encapsulated mass is composed of bland epithelial cells forming a few branching ducts, and small acinar clusters surrounded by a chondromyxoid stroma.
The patient had no postoperative complications, and no recurrence was seen on follow-up.
Discussion
A neck mass in the pediatric population presents a broad differential diagnosis and varied presentation. The differential diagnosis may include lesions that are inflammatory or congenital, with benign tumors and malignant tumors also being possible. A neck mass may present with systemic signs, such as fever or flu-like symptoms. Alternatively, it may cause neck weakness due to nerve compression. However, it can also be asymptomatic.
A pleomorphic adenoma usually presents as a single painless, slowly growing, firm, nodular mass. 8 Although pleomorphic adenomas are benign, they are aneuploid and can recur after resection. These tumors have the capacity to grow to a large size and can undergo malignant transformation to form carcinomas. 8
The diagnosis of salivary gland tumors relies on both histopathologic sampling and radiographic studies. Histopathologic sampling procedures include fine-needle aspiration and core-needle biopsy. Diagnostic imaging techniques for salivary gland tumors consist of ultrasound, CT, and magnetic resonance imaging. 8 The mainstay of treatment for salivary gland tumors is surgical resection. The need for more detailed surgical techniques and adjuvant radiotherapy depends on whether the tumor is malignant or benign. 8
A literature review reveals that pleomorphic adenomas are far less common in children than in adults and that when they occur, they are rarely located in the submandibular gland. Salivary gland lesions, regardless of location, comprise less than 10% of all pediatric head and neck tumors. 10
A study of 9,993 salivary gland lesions at the Armed Forces Institute of Pathology revealed only 10 cases of pleomorphic adenoma in the submandibular gland in children. 11 A prospective study regarding salivary gland tumors in 52 pediatric patients by Ellies et al demonstrated that only 3 children had pleomorphic adenomas of the submandibular gland. 7 A review of 105 pediatric patients with submandibular triangle tumors by Hockstein et al demonstrated that only 4 of 105 patients had pleomorphic adenomas. 1 The majority of the studies reviewed in the literature revealed that submandibular masses tended to be either inflamed or infected lymph nodes or glands.
Correct diagnosis of neck masses is important as it determines whether surgical intervention is required. In children, disease of the submandibular triangle requiring surgery is uncommon. Most pediatric lesions are inflammatory and resolve spontaneously or with a short course of antibiotics. 1 The diagnosis of the tumor may allow the surgeon to understand the gross dimensions and tissue texture. For example, a fleshy, invasive tumor will have different dimensions and tissue texture than a benign encapsulated tumor or a soft cystic mass. These traits, coupled with the local anatomy, will also affect the scope of the surgical procedure with regard to removing adjacent structures.
Knowing the tumor's anatomy and normal tissue anatomy will determine which anatomic structures the surgeon should pay particular attention to during surgery. This maximizes preservation of normal structures and removal of abnormal tissue in order to prevent recurrence.
A possible complication of surgery in the submandibular triangle is damage to the marginal mandibular branch of the facial nerve. It is much less common to damage the lingual and hypoglossal nerves. 1 The marginal mandibular branch of the facial nerve passes forward beneath the platysma and triangularis muscles. It innervates the muscles of the lower lip and chin, and it eventually communicates with the mental branch of the inferior alveolar nerve. Nerve damage may be caused by transection, stretch, or crush injury from aggressive dissection of the nerve. 1 Moreover, thermal injury may occur from electrocautery. For pleomorphic adenomas of the submandibular gland, it is prudent to perform regional dissection of the submandibular triangle to reduce the risk of recurrence.1,10
In summary, pleomorphic adenomas of the submandibular triangle in children are rare. In this population, it is more likely for the submandibular mass to be inflammatory in nature. Unfortunately, if the tumor is misdiagnosed or if its anatomy in this region is not delineated, incomplete excision may result in unacceptable recurrence rates. 1
The technical aspects of the surgery are important, particularly the preservation of the marginal mandibular branch of the facial nerve. This can be achieved by possessing a sufficient understanding of surgical principles and regional anatomy.