
Abstract
Rosai-Dorfman disease is a rare histiocyte disorder that is typically characterized by massive cervical lymphadenopathy. Isolated extranodal involvement is uncommon, and isolated laryngeal involvement is extremely rare. We report an unusual case of Rosai-Dorfman disease with isolated laryngeal involvement that led to recurrent dysphonia and airway obstruction. We discuss the challenges we faced in reaching a correct pathologic diagnosis and in deciding on an appropriate treatment regimen. Based on our experience, we believe that Rosai-Dorfman disease should be considered as a differential diagnosis inpatients who present with a recurrent inflammatory (histiocytic) mass lesion of the larynx.
Introduction
Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy) is a rare proliferative disorder of histiocytes. Its etiology is unclear. Clinical characteristics often include a painless cervical lymphadenopathy, fever, leukocytosis, an elevated erythrocyte sedimentation rate, and polyclonal hypergammaglobulinemia. 1
Reports indicate that 43% of patients with Rosai-Dorfman disease exhibit extranodal disease, with the head and neck region being one of the most common extranodal areas involved.2,3 Within the head and neck, the most common locations are the nasal cavity, paranasal sinuses, and orbit; isolated laryngeal involvement is extremely rare, as only 16 cases have been reported in the literature.4,5 We present a rare case of Rosai-Dorfman disease that was limited to the larynx, and we discuss the diagnostic difficulties we faced, as well as the clinical management of recurrent disease.
Case report
An otherwise healthy 45-year-old woman presented with an ongoing history of dysphonia secondary to a recurring right hemilaryngeal mass. She had been previously treated by a local otolaryngologist, who had removed similar masses on two previous occasions. Both times, pathology demonstrated chronic granulomatous inflammation, collagen interspersed with inflammatory infiltrate, and sheets of epithelioid histiocytes and lymphocytes. Stains for bacterial, mycobacterial, and fungal organisms were negative. The patients medical history was unremarkable, and a workup for autoimmune diseases, including sarcoidosis and Wegener granulomatosis, was negative.
On initial examination at our institution, videostroboscopy demonstrated a large submucosal fullness involving the right true vocal fold, which was relatively adynamic because of the lesion's mass effect. Computed tomography showed a 5.3 × 5.4-mm mass with enlargement and asymmetry of the right true vocal fold. The mass extended to the right false vocal fold, paraglottic space, and subglottis. No cervical lymphadenopathy was observed.
An excisional biopsy of the mass via suspension microdirect laryngoscopy was performed. Despite an adequate amount of specimen, permanent pathology demonstrated nonspecific, nondiagnostic fibrosis with chronic lymphocytic infiltrate. A second opinion was obtained from pathology departments at two academic institutions, but no diagnosis was reached.
The patient did well for 6 months until she again developed a recurrent right hemilaryngeal submucosal mass. At this point, she was referred to an outside institution, where biopsy specimens were diagnosed as Rosai-Dorfman disease based on pathologic interpretation of hyperplastic inflamed granulation tissue with foamy histiocytes. These histiocytes were positive for S-100 protein (figure 1), CD68, HAM-56, and lysozyme, and they showed emperipolesis. Subsequently, the patient began experiencing rapidly recurring laryngeal lesions with extensive glottic and subglottic involvement (figure 2).
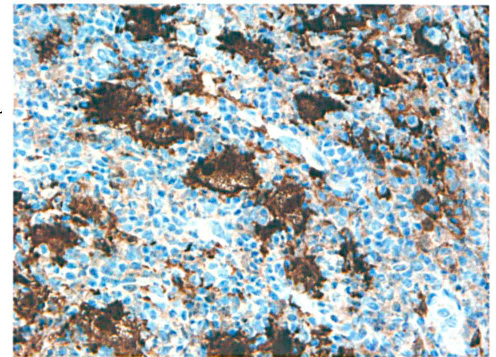
Histopathology with S-100 protein shows diffuse positively staining histiocytes throughout the section (original magnification x40).
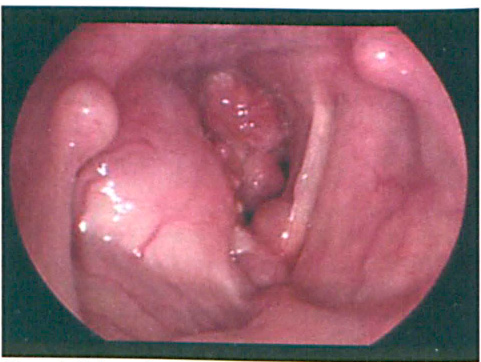
Videostroboscopy shows the submucosal fullness of the right false vocal fold and multiple polypoid lesions obstructing the respiratory glottis.
Over the following 3 months, the patient presented on two occasions with obstructive lesions that had caused stridor and respiratory distress, which required emergency excision. Postoperatively, high-dose steroids slowed the rate of recurrence, but the lesions immediately returned following the steroid taper. The patient then began local external-beam radiation therapy to her larynx, receiving 20 Gy in 10 daily 2-Gy fractions. At follow-up 4 months after the completion of radiation therapy, the patient exhibited no signs or symptoms of recurrence.
Discussion
Rosai and Dorfman first characterized a syndrome of sinus histiocytosis with massive lymphadenopathy in 1969. 1 Their initial description of the disease included the presence of massive bilateral cervical lymphadenopathy. Since then, limited reports in the literature have described extranodal involvement with or without lymphadenopathy. 4 An atypical, purely extranodal manifestation of Rosai-Dorfman disease poses a diagnostic challenge, as occurred in our case, as our patient presented with laryngeal involvement only.
For most cases of Rosai-Dorfman disease, histopathologic examination remains the gold standard for diagnosis. Analysis will show a proliferation of histiocytes with immunoreactivity for S-100 protein and CD68 with surrounding plasma cells and lymphocytes. 1 In addition to the classic histiocyte findings, Rosai-Dorfman lesions can exhibit large areas of nonspecific inflammatory change and fibrosis, which can obscure the underlying diagnosis. The delayed diagnosis in our case exemplifies this problem.
The course of Rosai-Dorfman disease is generally benign and self-limited, with periods of exacerbation and attenuation. 6 Because its etiology remains unknown and frequent spontaneous remissions occur, no standard therapy has been developed, so clinicians must pursue treatment based on the clinical presentation. In the more typically insidious cases, management should include regularly scheduled follow-ups to monitor for disease progression. In cases like ours, with disease recurrence and associated morbidity, more aggressive action—including steroid therapy, surgical excision, and radiation therapy—must be considered.