
Abstract
Patients with chronic obstructive pulmonary disease (COPD) may be at increased risk of aspiration secondary to impaired swallow function. One possible cause of this impairment is a reduction in laryngopharyngeal sensitivity. The relationship between COPD and laryngopharyngeal sensitivity has not been previously determined. We conducted a study to investigate the effect of COPD on laryngopharyngeal sensitivity by using laryngopharyngeal sensory discrimination testing (LPSDT). Our study population was made up of 20 adults (mean age: 71.7 yr) with clinically proven COPD and 11 healthy, age-matched controls. All 31 subjects underwent LPSDT with the use of an air-pulse stimulator via a nasendoscope. The threshold of laryngopharyngeal sensation was evaluated by measuring the amount of air pressure required to elicit the laryngeal adductor reflex (LAR). We found that the patients with COPD had a significantly higher LAR threshold than did the controls (p < 0.001). We conclude that patients with COPD have significantly less mechanosensitivity in the laryngopharynx. This sensory change may place patients with COPD at increased risk for aspiration.
Introduction
Chronic obstructive pulmonary disease (COPD) is the fourth-leading cause of death in the United States and Europe, and mortality among women as a result of COPD has more than doubled during the past 30 years. 1 COPD is reportedly the only principal cause of death whose prevalence is increasing, 2 and the burden of COPD is likely to worsen as the population continues to age. Indeed, hospitalization rates for COPD patients increase with age. The primary goals of hospitalization are to provide supportive care and to monitor drug therapy. The increasing demands on the healthcare system justify further research within this population to facilitate more effective management.
COPD patients commonly exhibit signs of malnourishment. Studies have indicated that 24% of COPD outpatients 3 and 47% of COPD inpatients 4 have a body weight less than 90% of their ideal weight. Dysphagia is often a precipitating factor for malnutrition. 5 Other possible factors include (1) the development of cachexia as a result of metabolic changes and (2) multiple periods of fasting as a prelude to procedures or investigations. 6
To date, relatively little research has been conducted on the prevalence of dysphagia and other swallowing disorders in patients with COPD. The reported prevalence of dysphagia in COPD patients varies considerably—from 17 to 85%.7,8 Some investigations have suggested that COPD may weaken the strength of swallow9,10 and increase the prevalence of pulmonary aspiration. 10 When combined with an impaired ability to use expired air to clear the larynx and protect the airway, a weak swallow may contribute to an increased risk for aspiration of pharyngeal contents, which in turn can lead to aspiration pneumonia. Although a range of abnormalities in swallowing function has been reported in patients with COPD who have frequent exacerbations, 10 the basis for the dysphagia is uncertain. One hypothesis is that a laryngopharyngeal sensory deficit exists.
Laryngopharyngeal sensory deficits in patients who have experienced a stroke have been reported to be predictive of aspiration pneumonia.11–13 More important, a laryngopharyngeal sensory deficit without clinical evidence of dysphagia— that is, a silent sensory deficit—may be hazardous because it is likely to escape detection and to predispose the patient to silent aspiration. 12
Additionally, conventional clinical techniques used to assess laryngopharyngeal sensory deficits, such gag reflex testing, seem to be of questionable value. The gag reflex test measures the activity of the glossopharyngeal nerve (cranial nerve IX) rather than the superior laryngeal branch of the vagus nerve (cranial nerve X), which innervates the hypopharynx and larynx. Moreover, some research has shown that the gag reflex test is not a useful predictor of laryngopharyngeal sensitivity or aspiration pneumonia. 14 A more sensitive test is required.
Laryngopharyngeal sensory discrimination testing (LPSDT) is a safe, reproducible method of identifying patients with laryngopharyngeal sensory deficits and hence those at increased risk for pulmonary aspiration.14,15 With this test, the integrity of laryngopharyngeal sensitivity is determined by identifying the threshold at which the laryngeal adductor reflex (LAR) is triggered in response to air-pulse stimuli. The LAR represents the transient adduction of the true vocal folds in response to a mechanical stimulus. This reflex is designed to protect the lower airway from foreign material (food, fluid) and noxious stimuli (hot air, gases).
Laryngopharyngeal sensitivity as measured by LPSDT has been determined in normal subjects, 16 in patients after stroke, 12 and in patients with proven gastroesophageal reflux disease (GERD). 17 However, it is not known whether laryngopharyngeal sensitivity as measured by LPSDT is abnormal in patients with COPD and, if it is, whether such an impairment predicts the presence of a swallowing disorder or pulmonary aspiration.
A simple, reproducible test of laryngopharyngeal sensitivity that would potentially predict which COPD patients are at highest risk for swallowing disorders and aspiration would be clinically useful and would allow clinicians to initiate preventive measures earlier. Therefore, we evaluated LPSDT to determine if it fills these needs.
Patients and methods
The primary goals of our study were (1) to identify the prevalence of laryngopharyngeal sensory impairment as determined by the LAR threshold in patients with proven COPD and (2) to characterize the relationship between laryngopharyngeal sensory impairment and the severity of COPD.
Inclusion criteria
The criteria for study eligibility were:
age between 40 and 80 years;
a diagnosis of COPD based on The Thoracic Society of Australia & New Zealand (TSANZ) criteria 18 ;
a baseline forced expiratory volume in 1 second (FEV1) measurement of less than 70% of predicted;
clinically stable COPD—that is, an absence of exacerbations for at least 6 weeks—as determined by a senior thoracic physician (A.J.I.); and
respiratory failure on blood gas criteria—that is, an arterial oxygen pressure (PaO2) of less than 60 mm Hg or an arterial carbon dioxide pressure (PaCO2) of more than 50 mm Hg.
The TSANZ criteria for a diagnosis of COPD specify that the patient must present with symptoms of breathlessness, cough, and sputum production. 18 Also, spirometry results must show a ratio of FEV1 to forced vital capacity (FVC) of less than 70%. The predicted FEV1 values in our COPD patients ranged from 19 to 68% (mean: 38.35 ± 14.60%; 95% confidence interval [CI]: 31.87 to 44.82%) (table 1).
Selected patient characteristics
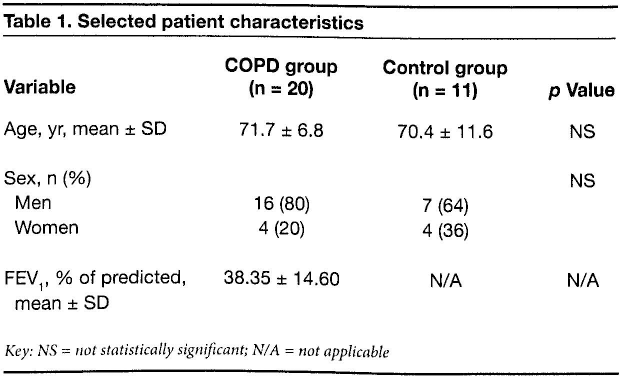
Key: NS = not statistically significant; N/A = not applicable
The severity of COPD was determined by pulmonary function testing performed in accordance with American Thoracic Society criteria.19,20 Respiratory function tests were performed with body plethysmography (Vmax: SensorMedics Corp.; Yorba Linda, Calif.).
Exclusion criteria
Potential participants were excluded if they demonstrated any of the following:
a history of head and neck surgery;
a neurologic impairment or progressive neurologic disease, including traumatic brain injury and bulbar or pseudobulbar palsy; and
a diagnosis of GERD or reported clinical symptoms of GERD.
These conditions are known to be associated with swallowing disorders and impaired laryngopharyngeal sensitivity.
Patients and controls
Once potential participants were judged to have met all eligibility criteria, they were approached for consent to participate. Patients had been recruited through one of two methods:
We consulted hospital admissions lists to identify patients who had been admitted under the care of respiratory physicians or who were admitted to the respiratory ward. These patients had been hospitalized for treatment of exacerbations of their illness or for some other medical or surgical reason.
We consulted lists of outpatients of visiting thoracic physicians. All potential candidates had their medical records examined by the study's speech pathologist (N.A.C.), who determined their eligibility for inclusion in the study.
Controls were recruited from a variety of sources: hospital staff, family members of the researchers, and current orthopedic patients at Concord Repatriation General Hospital in Concord, New South Wales, Australia.
During the study period, 33 participants were recruited: 22 patients and 11 controls. Two of the COPD patients were unable to tolerate LPSDT, and they were dropped from the study and their data were not included in our results, leaving us with 20 COPD patients—16 men and 4 women, aged 54 to 80 years (mean: 71.7). The control group was made up of 7 men and 4 women, aged 41 to 79 years (mean: 70.4). The differences between age and sex in the two groups were not statistically significant (table 1).
Laryngopharyngeal sensitivity testing
Preparation for LPSDT involved the topical application of viscous lidocaine to both nares to facilitate tolerance of the nasendoscopy. Anesthetic spray was not used because it might have influenced the results of sensory testing. The nasendoscope (FNL-10AP; KayPENTAX; Montvale, N.J.) was attached to an air-pulse sensory stimulator (AP-4000; KayPENTAX), and it was then passed transnasally through to the laryngopharynx until it became situated approximately 3 mm above the arytenoid eminence. Establishing the presence of light reflection from the nasendoscope onto the arytenoid eminence in addition to deflection of arytenoid tissue when an air pulse was triggered allowed us to correctly position the nasendoscope and thereby ensure the accuracy of the distance between the scope and the arytenoid eminence.
Air pulses of 50 ms in duration were delivered to the arytenoid eminence, initially at a pressure of 6.0 mm Hg in accordance with the descending and ascending threshold testing protocol described by Aviv et al in 1993. 14 If the LAR was triggered at 6.0 mm Hg, the pressure of the pulses was reduced in 0.5-mm Hg increments until the reflex was no longer observed. At that point, air pressure was then increased in 1.0-mm Hg increments until the reflex was observed again.
If no LAR was triggered at 6.0 mm Hg, air pulses were increased in 1.0-mm Hg increments until the reflex was observed. Once the reflex was elicited, air pulses were systematically reduced by 0.5 mm Hg until the reflex was no longer observed. The LAR threshold was defined as the lowest air pressure that triggered the reflex on three separate occasions.
The air-pulse sensory stimulator we used was unable to generate air pulses greater than 9.9 mm Hg. So for the purposes of this study, if no LAR was observed at 9.9 mm Hg, the duration of the air pulse was extended from 50 ms to 1.0 sec at 9.9 mm Hg. If a response was still not elicited, the LAR threshold was determined to be 9.9 mm Hg.
Testing was conducted unilaterally only because none of the COPD patients was considered to be at risk of asymmetrical sensory impairment in view of the absent history of neurologic disease and head/neck pathology. The physician performing LPSDT (A.J.I.) was blinded to the patient's level of lung function abnormality, but not to the COPD diagnosis.
For LPSDT, patients sat upright in a chair. They were not informed about the ascending and descending nature of the air-pulse pressures. The air pulses were delivered at irregular intervals so that the patients could not know or anticipate when each would be administered.
Controls
All the control subjects were recruited for the purpose of determining normal laryngopharyngeal sensation. Each control provided a detailed medical history that included information that would be useful in identifying a potential swallowing disorder. Potential controls were excluded if they had a history of neurologic disease, respiratory disease, dysphagia, GERD, smoking, abnormal lung function as measured by spirometry, or any other relevant significant disease. All controls underwent LPSDT under the same protocol used for the COPD patients.
Analysis of results
Our null hypothesis was that there is no difference in laryngopharyngeal sensitivity between COPD patients and healthy controls. Based on the findings of a previous pilot study, in which a difference of 0.5 mm Hg (±0.32) was seen between COPD and healthy populations, we conducted a sample size calculation based on α = 0.05 and β = 0.10 (power = 90%). Using these values, we determined that we would need a minimum of 14 COPD patients to test our null hypothesis.
Our data were entered into a Microsoft Excel spreadsheet (Microsoft; Redmond, Wash.), and statistical analysis was performed with the Statistical Package for the Social Sciences software (v. 11.0; SPSS; Chicago). All data were tabulated and reviewed descriptively for completeness and distribution. In view of non-normal distributions and our limited sample size, nonparametric methods were used to evaluate the relationship between the primary outcome (LAR threshold) and all other endpoints.
Means, modes, and standard deviations were derived for all variables. Groups were then compared for variables such as age, sex, admission diagnosis, and respiratory function. Any differences between the groups were sought using odds ratios with 95% CIs applied.
Cross-tabulation and the Fisher exact test were employed to examine the relationship between the categorical endpoints of each group; FEV1 values, age, and sex. The Mann Whitney U test, which is the nonparametric t test for independent samples, was employed to evaluate the relationship between the LAR threshold and each group.
Ethical considerations
All procedures were approved by the Concord Repatriation General Hospital's Research and Ethics Committee. All study patients provided written informed consent.
Results
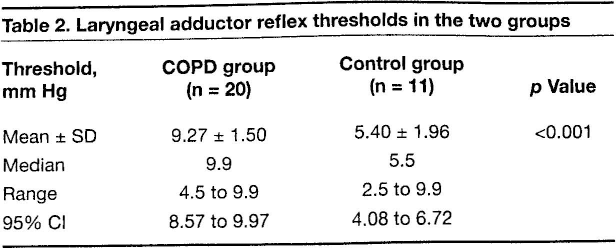
The LAR thresholds for the COPD patients ranged from 4.5 to 9.9 mm Hg (mean: 9.27; median: 9.9; 95% CI: 8.57 to 9.97). For the control group, thresholds ranged from 2.5 to 9.9 mm Hg (mean: 5.40; median: 5.5; 95% CI: 4.08 to 6.72) (figure 1, table 2). The difference between the two groups was statistically significant (p < 0.001) according to the independent samples t test where equal variance was assumed (Levene test for equality of variances).
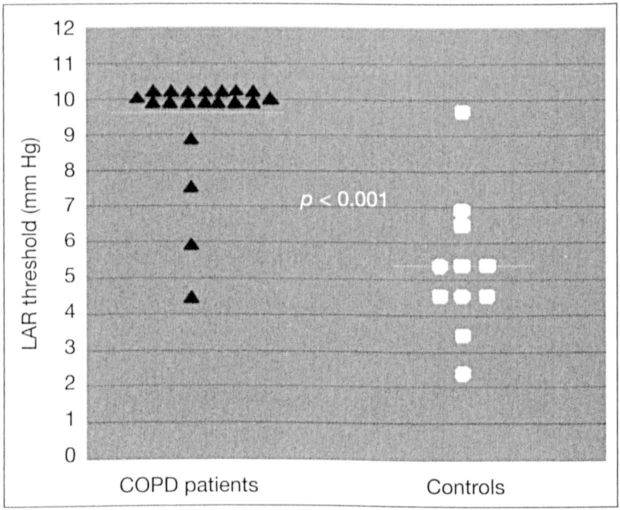
Graph shows the individual LAR thresholds in the two groups. The difference was statistically significant.
Laryngeal adductor reflex thresholds in the two groups
LPSDT and FEV1 data were reviewed to identify the presence of any relationship using the Pearson product-moment correlation coefficient. No significant correlation was identified between laryngopharyngeal sensitivity and FEV1 (r = 0.240; p = 0.308) (figure 2).
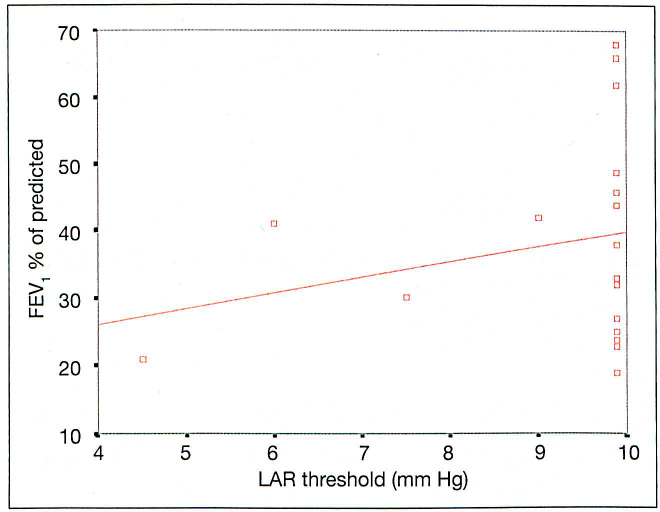
Graph shows the distribution of LAR thresholds according to the percentage of predicted FEV1 in the COPD patients (some values overlap). There was no significant correlation between the two parameters. Diagonal line indicates the comparative trend.
Discussion
LPSDT was considered to be reproducible in our clinical setting. Reproducibility was previously reported in 2005 by Phua et al, 17 who conducted LPSDT with the same equipment and parameters that we used in our study. They demonstrated a standard deviation for measurement error at 0.34 and a coefficient of variation at 9.7%; additionally, test repeatability was 0.96.
Our study revealed that patients with COPD have a significantly worse level of laryngopharyngeal sensory impairment as defined by the LAR threshold compared with healthy controls (p < 0.001). Impaired laryngopharyngeal sensitivity may be clinically important in COPD patients, who have high rates of hospitalization related to lower respiratory tract infections. In fact, impaired sensitivity may be partly responsible for the higher incidence of these complications in COPD patients.
A number of researchers have completed studies examining the effect of impaired laryngopharyngeal sensitivity on the risk for aspiration and aspiration pneumonia. In 1997, Aviv et al evaluated laryngopharyngeal sensitivity testing by using the modified barium swallow test as a predictor of aspiration pneumonia after stroke. 13 They found that the combination of the two tests was useful in predicting which patients were at high risk for developing aspiration pneumonia. They also reported that those patients who had bilateral sensory deficits (as defined by LPSDT) had the greatest risk for developing pulmonary complications secondary to aspiration, regardless of whether or not they showed evidence of aspiration on a modified barium swallow examination.
In our study, 19 of 20 COPD patients (95%) demonstrated impaired laryngopharyngeal sensitivity as indicated by a LAR threshold of 5.0 mm Hg or higher. This high proportion suggests that these patients may be at increased risk for developing aspiration pneumonia.
In 2001, Setzen et al reported the results of their study of laryngopharyngeal sensory deficits as a predictor of aspiration. 21 They examined pharyngeal muscle contraction and aspiration in 40 patients with dysphagia. Their results revealed that patients with no LAR had a higher incidence of aspiration and pharyngeal muscular weakness than did controls with normal laryngopharyngeal sensitivity. They concluded that a strong relationship exists between sensory loss and motor deficits, and that these two features may be used to predict those patients at greater risk for aspiration. Their results suggest that the COPD patients in our study may be at increased risk for both aspiration and impaired pharyngeal muscle strength. Further studies to examine the relationship between laryngopharyngeal sensitivity and pharyngeal muscle strength in patients with COPD would be beneficial.
As an extension of the study by Setzen et al, 21 Avivet al 22 investigated LAR and pharyngeal squeeze (a technique designed to assess the integrity of pharyngeal muscle contraction) as predictors of laryngeal penetration and aspiration. Aviv et al also reported a strong association between motor and sensory deficits, and they concluded that patients with no LAR were more likely to demonstrate laryngeal penetration and aspiration than were those in whom LAR was intact (p < 0.0001).
Aviv et al also reported a significant difference in the integrity of pharyngeal muscular contraction (as defined by pharyngeal squeeze) between the two groups. 22 Those patients with no LAR had a higher incidence of impaired pharyngeal squeeze (p < 0.0001) than did the patients with an intact reflex. The findings of Aviv et al further suggest that the COPD patients in our study may have an increased risk for impaired pharyngeal muscle strength and aspiration.
Setzen et al 23 in 2003 and Perlman et al 24 in 2004 reported further studies examining the predictive value of laryngopharyngeal sensitivity and pharyngeal squeeze for aspiration. Setzen et al concluded that regardless of pharyngeal motor function, severe laryngopharyngeal sensory deficits were associated with aspiration of thin liquids (p < 0.05). 23 Perlman et al concluded that patients with impaired pharyngeal motor function at different levels of sensory loss had a higher risk for aspiration of pureed foods than did subjects with normal pharyngeal motor function. 24 Furthermore, they suggested that hypopharyngeal muscle tone may be a better predictor of aspiration of pureed foods than is laryngopharyngeal sensation.
The implications for our study are that although laryngopharyngeal sensitivity deficit in COPD may be indicative of a higher aspiration risk, an additional assessment of pharyngeal muscle strength may further reinforce the evidence suggesting an elevated risk for aspiration.
While our study demonstrated a high incidence of laryngopharyngeal sensory impairment in patients with COPD, the integrity of pharyngeal motor function in this population remains unknown. Investigators contemplating future studies should consider examining the relationship between laryngopharyngeal sensitivity, pharyngeal squeeze, and swallow function in COPD patients.
In our study, no relationship was identified between the severity of laryngopharyngeal sensory impairment (as defined by the LAR threshold) and the severity of COPD (as defined by FEV1 testing). While the diagnosis of COPD was strongly related to laryngopharyngeal sensory impairment, the severity of COPD did not correlate with deterioration in laryngopharyngeal sensitivity. This may imply that the presence of COPD itself is enough to predict impairment of laryngopharyngeal sensitivity.
A future study that involves a larger sample size and a study population that includes non-COPD subjects with a similar percentage of predicted FEV1 values might be able to determine if a relationship exists. Additionally, if LAR thresholds can be more accurately determined in the upper range (should LPSDT be modified to reflect pressures greater than 9.9 mm Hg), the nature of any relationship might be further clarified.
For our study, we attempted to remove age as a possible confounding factor. COPD typically occurs in older populations because lung damage from tobacco use takes a period of time to present as an airways disease. The mean age of the COPD patients in our study was fairly high (71.7 yr). Therefore, we age-matched our healthy control group to the COPD group in an effort to ensure that any difference in laryngopharyngeal sensitivity between the two groups could not be attributed to age alone.
Our study demonstrated that COPD patients exhibited a significant reduction in mechanosensitivity in the laryngopharynx. The cause of this sensory impairment may be related to a number of variables. For example, the effect of inhaled corticosteroids and inhaled anticholinergics on laryngopharyngeal sensation is unknown. These medications are used widely in COPD management, and they may have an unknown effect on the sensory mucosa in the laryngopharynx. Active smoking and the presence of chronic cough resulting in laryngeal edema are commonly reported in COPD patients; such edema may be a contributing factor to reduced sensation.
Finally, GERD is known to inhibit laryngopharyngeal sensitivity. 17 While patients with symptomatic GERD were excluded from our study, the presence of occult GERD cannot be ruled out. Future research efforts should attempt to account for the presence of GERD by requiring 24-hour ambulatory esophageal dual-channel pH manometry as a part of any study protocol.
In conclusion, our study has revealed that the laryngopharyngeal sensation of patients with COPD was significantly impaired, suggesting that this population may be at increased risk for aspiration. Additional longer-term investigations of the outcomes of COPD patients with this impairment are warranted.