
Abstract
Bleeding during endoscopic sinus surgery (ESS) can interrupt the flow of the procedure and increase the risk of complications. Advances in microdebrider design now allow for bleeding to be controlled by bipolar energy during the suctioning and shaving of polyps. We conducted a retrospective study to examine the effects of this technology on blood loss and operating times during ESS for chronic rhinosinusitis with nasal polyps (CRS+P). Our patient population was made up of 80 patients who had undergone ESS for CRS+P by the same surgeon from January 2007 through May 2008. All surgeries were performed with either the PK diego bipolar microdebrider (Gyrus ACMI, ENT Division; Bartlett, Tenn.) or a standard microdebrider. There were 40 patients in each group. The PK group was made up of 23 males and 17 females, aged 14 to 66 years (mean: 43.1), and the control group included 21 males and 19 females, aged 17 to 71 years (mean: 43.1); there were no statistically significant differences between the two groups in terms of sex and age. In addition to demographic data, the charts were reviewed for comorbidities and operative variables; the latter included blood loss, operating room (OR) time, and complications. The preoperative treatment and anesthesia protocols were similar for all patients, and all patients demonstrated a similar disease burden on imaging (mean Harvard CT stage: 3.12 for the PK group and 3.15 for the controls; p > 0.05). We found that during ESS, the PK group experienced significantly less intraoperative blood loss than did the controls (means: 86.0 and 123.0 ml, respectively; p = 0.015). In addition, the PK device was associated with significantly shorter OR times (means: 88.9 and 101.4 min, respectively; p = 0.026). There were no complications in either group. We conclude that usinga microdebrider with bipolar capabilities during ESS may offer the advantages of less blood loss and shorter operating times inpatients with nasal polyps.
Introduction
Since their introduction in 1984, 1 endoscopic sinus surgery (ESS) techniques have continued to evolve at a rapid pace, often propelled forward by technological advances. The popularity of the microdebrider, which is heralded as one of the premier innovations in instrumentation for ESS, has continued to grow and has reduced our reliance on traditional sinus instruments such as curettes and forceps.
Invented for use in small-joint arthroscopic surgery, the microdebrider is a cylindrical, electrically powered shaver that has a hollow blade through which continuous suction is applied. 2 The rotating blade is housed within a smooth outer sheath, which limits the risk of adjacent trauma. These devices were introduced for nasal surgery in 1996 by Setliff 3 and Parsons, 4 and they have continued to undergo improvements in design and versatility. 5
Microdebriders are preferred for ESS by many surgeons because they not only spare adjacent mucosa, but they also offer improved precision, more expeditious tissue removal, and better visualization.6–8 The ability to simultaneously suction blood away from the surgical field is especially advantageous during ESS for polyp removal, given the propensity of polypoid tissue to bleed during removal. Significant intraoperative bleeding can increase the risk of complications, and it may even necessitate that a procedure be terminated prematurely.
While microdebriders were originally designed to clear bleeding, until recently they could do nothing to actually stop bleeding. Today, however, advances in microdebrider technology have led to the added ability of the device to control bleeding with bipolar energy while retaining the shaving and suctioning capabilities of conventional microdebriders. We hypothesized that the ability to locally control bleeding as it arises during ESS would decrease blood loss and, as a byproduct, reduce the operating time. Therefore, we conducted a study of our initial experience with a bipolar microdebrider to explore the impact of this new tool on blood loss and operating times during ESS performed in patients being treated for chronic rhinosinusitis with nasal polyps (CRS+P).
Patients and methods
Patients
In this retrospective cohort study, we compared the outcomes of a group of 40 consecutively presenting patients who had undergone surgery with the new technology after it had become available at our institution (Saint Louis University Hospital) with the outcomes of a sex- and age-matched group of 40 controls who had undergone ESS prior to the acquisition of the bipolar microdebrider. All patients had presented with medically refractory CRS with evidence of nasal polyps on endoscopy, as well as significant disease on post-therapy computed tomography (CT).
Exclusion criteria included insufficient documentation, a known coagulopathy, the routine use of anticoagulants, and a final pathology report containing evidence of anything other than benign inflammatory polyps (e.g., sarcoidosis, inverted papilloma, and other neoplasia).
The 80 patients in this study had undergone ESS for CRS+P from January 2007 through May 2008. The 40 patients treated with the bipolar microdebrider—23 males and 17 females, aged 14 to 66 years (mean: 43.1)—had undergone surgery with the PK diego bipolar microdebrider (Gyrus ACMI, ENT Division; Bartlett, Tenn.). The 40 controls—21 males and 19 females, aged 17 to 71 years (mean: 43.1)—had been operated on with a conventional microdebrider without hemostatic capabilities (Straightshot; Medtronic Xomed; Jacksonville, Fla.).
Surgical procedure
Prior to surgery, each patient had been treated with a standardized preoperative regimen of prednisone 30 mg/day beginning 5 days before surgery. At operation, the nose was prepared with oxymetazoline spray 0.05% followed by a submucosal injection of 1% lidocaine with 1/100,000 epinephrine into the middle turbinates and lateral nasal walls. Then pledgets soaked with cocaine 4% were placed for further decongestion.
All patients were administered a standardized intravenous anesthesia protocol: midazolam 1 to 2 mg for preinduction; lidocaine 50 mg, propofol 2 mg/kg, and fentanyl 50 to 100 μg for induction; rocuronium 35 mg and either desflurane or sevoflurane 1 to 1.5 minimum alveolar concentration for maintenance; and dexamethasone 10 mg and ondansetron 4 mg for prevention of postoperative emesis.
All 80 operations had been performed by the same senior surgeon (R.S.). One blade perprocedure was used. Postoperatively, patients were given a 7-day course of antibiotics and instructed to begin nasal saline irrigations on postoperative day 1, per routine.
Outcomes measures
The primary endpoint was estimated intraoperative blood loss, which was obtained from the surgical notes and medical records. As a secondary endpoint, we examined intraoperative times. In each instance, the surgical time was defined as the recorded “cut time” rather than the “in and out of the room time”; the latter includes allowances for time spent on patient positioning, anesthesia, and preliminary preparations, which we did not factor in.
In addition to demographic data, we compiled information on a variety of comorbidities to assess potential covariates for blood loss and operating room (OR) time. We also reviewed medication use (notably aspirin), family history of blood dyscrasias, and smoking status (patients who had abstained from tobacco for a least 1 year were considered to be nonsmokers). Preoperative CT scans were reviewed and graded according to the Harvard CT staging system as an index of disease severity. We also noted operative variables, such as revision status, the use of image guidance, and the extent of surgery (i.e., the number of sinuses operated on).
Other protocols
Statistical analysis was performed with the unpaired Student t test. Approval of the study protocol was obtained from the Saint Louis University Institutional Review Board.
Results
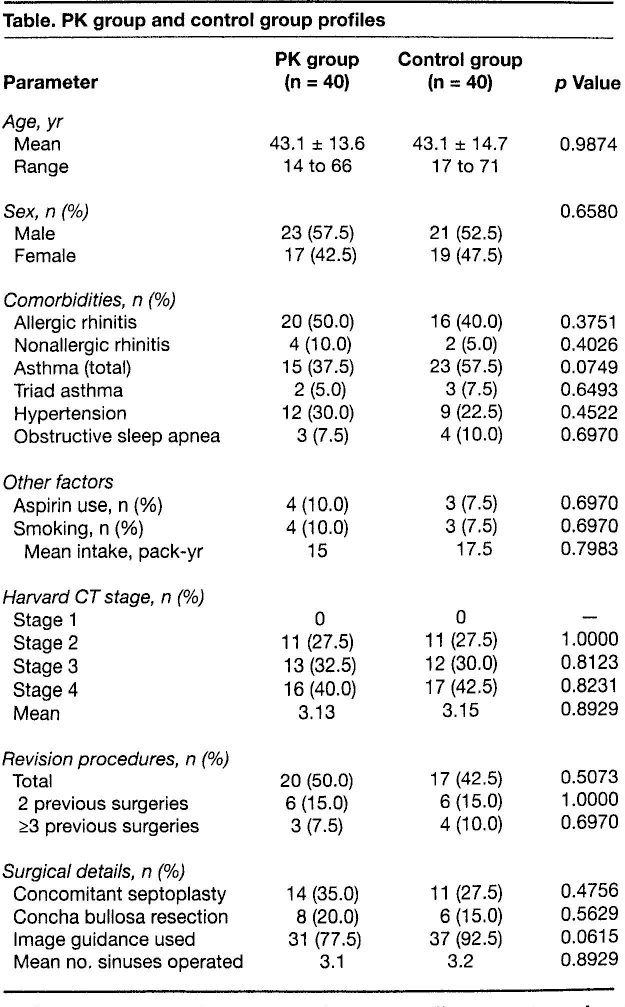
The two groups had similar findings in all tracked covariates. There were no statistically significant differences between the two groups in demographic variables, comorbidities, aspirin use, or smoking status (table). In addition, the disease burden based on Harvard CT stage and surgical variables such as revision status, the use of image guidance, and the extent of surgery were also very similar (p > 0.05).
Table. PK group and control group profiles
There were no complications in either group. All patients were discharged home after surgery. No patient required any postoperative intervention for bleeding such as cautery, packing, or an emergency department visit.
Amount of blood loss
The PK group experienced significantly less intraoperative blood loss than did the control group (figure 1). The mean amount of blood loss was 86.0 ml (±40.9) in the PK group and 123.0 ml (±66.0) in the control group, which represents an overall reduction of 30.1% (p = 0.015).
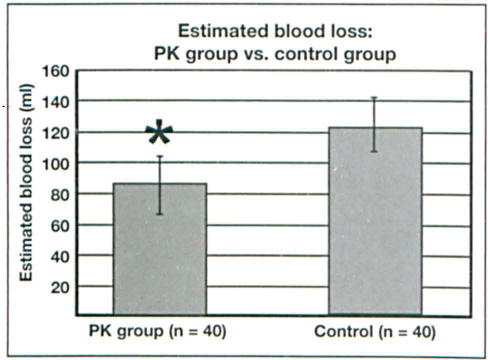
Chart shows that the PK group experienced significantly less (p = 0.015) mean intraoperative blood loss (86.0 ml) than did the control group (123.0 ml).
Amount of operating time
The patients in the PK group also benefited from a significant decrease in operating time (figure 2). Their mean OR time was 88.9 minutes (±23.6), versus 101.4 minutes (±24.9) for the control patients (p = 0.026). The 12.5-minute difference represents a reduction of 12.3%.
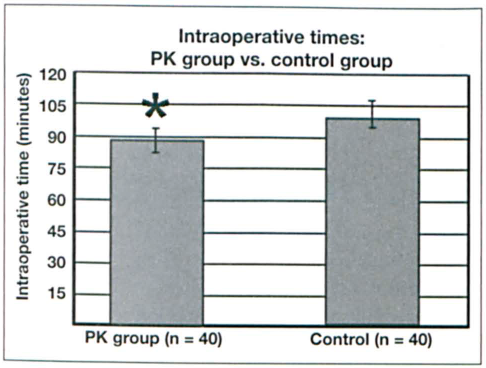
Chart depicts the statistically significant difference (p = 0.026) in mean operating times between the PK group (88.9 min) and the control group (101.4 min).
Discussion
This pilot study demonstrated a 30% decrease in blood loss as well as a 12% reduction in surgical procedure time when the bipolar microdebrider was used instead of a microdebrider that did not have hemostatic capabilities. However, while these results are statistically significant, they may not be clinically significant.
The blood loss experienced by patients in both study groups was not extensive, and it was obviously not associated with a demonstrable decrease in complications since no complications occurred in either group. However, it is widely accepted that complication rates from ESS are greatly impacted by bleeding and the accompanying obstruction of vision.9,10 When considered in this context, any reduction in bleeding would be advantageous because it may serve to improve intraoperative orientation and maintain the continuity and pace of the operation.
The reduction in bleeding noted with the use of the bipolar microdebrider likely accounted for the decrease in OR time. Shortening an operation by 12.5 minutes may not seem consequential in a major tertiary care hospital, but at Saint Louis University Hospital, the estimated cost of running an OR is roughly $1,500 per hour, so the savings accrued over time can become meaningful. Also, routinely shortening case times to this degree may result in increased surgical throughput in high-volume settings such as ambulatory surgery centers, for example. 11
Another cost consideration is the price of blades. Bipolar blades are slightly more expensive than standard microdebrider blades (currently ∼$45 more), and they require a console that supports the newer technology. By factoring in both the higher cost of the blade and the reduction in operating time, we estimated that the overall savings achieved by using the bipolar microdebrider was approximately $267.50 for each sinus surgery performed.
Intuitively, taking the opportunity to control bleeding during polyp surgery by using a bipolar microdebrider seems like a worthwhile endeavor. Although other techniques are used to achieve hemostasis during sinus surgery (e.g., topical agents, temporary packing, and suction cautery), no other method provides for simultaneous dissection and hemostasis in one device.
There are several drawbacks to using topical agents or temporary nasal packing to control bleeding intraoperatively. These methods can take some time to work, and they can significantly disrupt the flow of the procedure. They are also usually not as effective as, for example, more definitive techniques such as cautery.
Suction (monopolar) cautery has its own drawbacks in that it requires the use of another instrument and it generates a significant amount of heat. This is of particular concern when operating on or near the skull base and orbit, where the use of monopolar cautery is relatively contraindicated.
Commercially available since 2005, the PK diego is the only microdebrider currently on the market that offers a means of hemostasis in addition to the shaving and suctioning features common to this class of instrument. It differs from other microdebriders in that its blades contain insulation and electrode layers that deliver bipolar energy (figure 3). The bipolar function is achieved by radiofrequency manipulation of small pulses of energy at a high, medium, or low setting (40, 20, or 10 W of power, respectively). Compared with monopolar energy, it significantly limits the transmission of heat to adjacent intraorbital and intracranial structures.
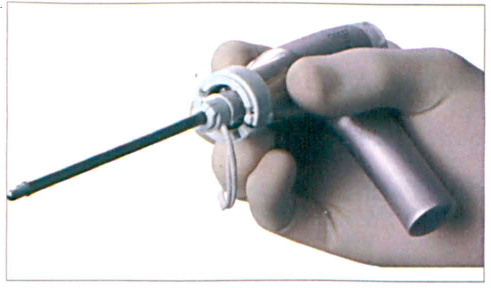
The PK diego employs bipolar energy between two electrodes to achieve hemostasis. Several layers of insulation are present.
The application of this instrument is also well suited for submucosal inferior turbinate reduction because bleeding from the turbinate interior, as well as the entry site, can be controlled. We have also had favorable experiences with using this technology for endoscopic removal of other vascularized tissues such as adenoids, tumors, and encephaloceles.
In addition to higher costs, the disadvantages of the use of microdebriders in general for ESS include a lack of tactile feedback and ineffectiveness at removing thick bone. It behooves surgeons who use any microdebrider to bear in mind that although major complications of ESS are rare, 12 those that do occur when a microdebrider is employed tend to progress more quickly because of the powered nature of this device.
This study has several significant limitations. These include the retrospective design, the relatively small patient population, the lack of randomization, and our reliance on the medical record for evaluation of blood loss. Thus, our methodology did not allow us to arrive at firm conclusions, and our findings should be regarded as representing the personal experience of a senior surgeon with an emerging technology.
Having said this, we note that it is exciting to consider that in addition to the established advantages of conventional microdebriders, newer generations of microdebriders may also reduce blood loss and shorten OR times during surgery for nasal polyps. Further investigation is needed to examine the evolving role and impact of this innovative technology.
Footnotes
Financial disclosure: Drs. Kumar and Sindwani had no financial relationships relevant to this study at the time it was performed and accepted for publication. Dr. Sindwani is now a consultant for Gyrus ACMI of Bartlett, Tenn., the parent company of the manufacturer of the PK diego bipolar microdebrider, but he received no funding for this study. The company had no role whatsoever in the design or execution of this study, the data management, or the decision to publish it.