
Abstract
Neurofibroma of the parotid gland is extremely rare. When it does occur, it is usually seen in patients with neurofibromatosis type 1 (NF-1). We encountered a case of intraparotid neurofibromatosis that arose in the absence of a definitive diagnosis of NF-1.
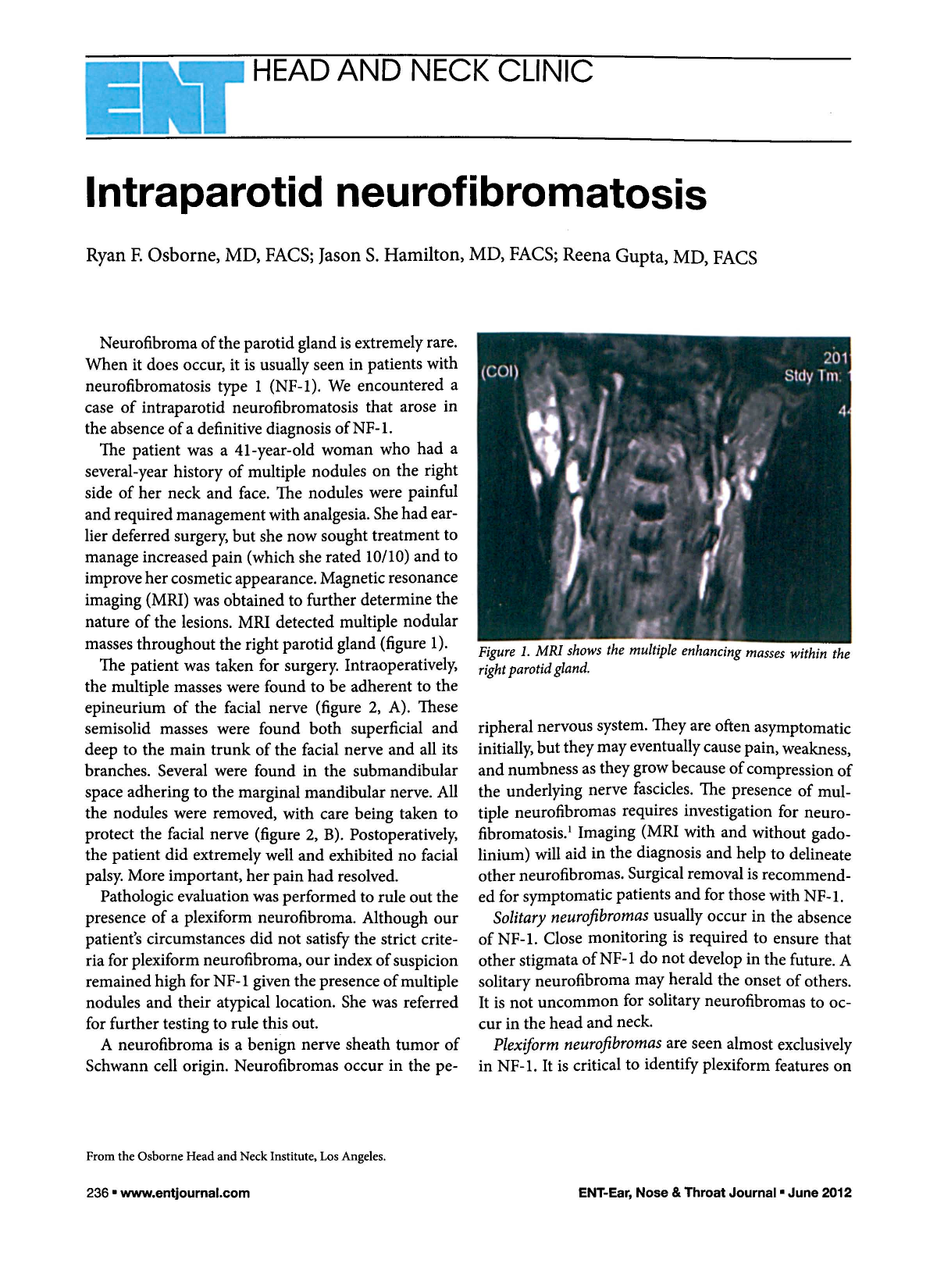
The patient was a 41-year-old woman who had a several-year history of multiple nodules on the right side of her neck and face. The nodules were painful and required management with analgesia. She had earlier deferred surgery, but she now sought treatment to manage increased pain (which she rated 10/10) and to improve her cosmetic appearance. Magnetic resonance imaging (MRI) was obtained to further determine the nature of the lesions. MRI detected multiple nodular masses throughout the right parotid gland (figure 1).

MRI shows the multiple enhancing masses within the right parotid gland.
The patient was taken for surgery. Intraoperatively, the multiple masses were found to be adherent to the epineurium of the facial nerve (figure 2, A). These semisolid masses were found both superficial and deep to the main trunk of the facial nerve and all its branches. Several were found in the submandibular space adhering to the marginal mandibular nerve. All the nodules were removed, with care being taken to protect the facial nerve (figure 2, B). Postoperatively, the patient did extremely well and exhibited no facial palsy. More important, her pain had resolved.

Pathologic evaluation was performed to rule out the presence of a plexiform neurofibroma. Although our patients circumstances did not satisfy the strict criteria for plexiform neurofibroma, our index of suspicion remained high for NF-1 given the presence of multiple nodules and their atypical location. She was referred for further testing to rule this out.
A neurofibroma is a benign nerve sheath tumor of Schwann cell origin. Neurofibromas occur in the peripheral nervous system. They are often asymptomatic initially, but they may eventually cause pain, weakness, and numbness as they grow because of compression of the underlying nerve fascicles. The presence of multiple neurofibromas requires investigation for neurofibromatosis. 1 Imaging (MRI with and without gadolinium) will aid in the diagnosis and help to delineate other neurofibromas. Surgical removal is recommended for symptomatic patients and for those with NF-1.
Solitary neurofibromas usually occur in the absence of NF-1. Close monitoring is required to ensure that other stigmata of NF-1 do not develop in the future. A solitary neurofibroma may herald the onset of others. It is not uncommon for solitary neurofibromas to occur in the head and neck.
Plexiform neurofibromas are seen almost exclusively in NF-1. It is critical to identify plexiform features on pathology because patients with NF-1 and plexiform neurofibromas have a 10 to 15% risk of malignant transformation. 1 This transformation most commonly occurs in the third decade of life. 2 Although surgery is recommended for treatment, its success is somewhat limited by the multifocal nature of the disease; as a result, the recurrence rate is relatively high. 3