
Abstract

Auricular cartilage grafts may be the most frequently used autologous graft material in facial plastic surgery. These versatile grafts can be used to address both functional and aesthetic problems. They are nearly universally available, even in patients who have had prior nasal surgery, and they avoid the potential problems of graft rejection or extrusion that can occur with synthetic materials.
Often, insufficient cartilage is available in patients who have undergone prior septal surgery if grafts are needed for revision surgery, and the auricular site is a preferred source. Costal cartilage is an additional option, but most patients prefer the reduced morbidity of an auricular graft and the advantage of a hidden incisional scar.
Common uses for auricular cartilage grafts include alar batten grafts to treat nasal sidewall collapse; dorsal onlay grafts to treat the over-resected nasal dorsum or the low radix or, when shaved thin, to camouflage dorsal irregularities in rhinoplasty surgery; nasal tip grafts in primary and secondary rhinoplasty; postauricular perichondrium grafts to overlay the nasal tip and dorsum in the thin-skinned rhinoplasty patient; nasal alar reconstruction after skin cancer resection; lower lid space grafts to treat ectropian in the paralytic lower lid; and cartilage graft material to assist in repairing septal perforations.
While some surgeons prefer harvesting the auricular cartilage from an anterior approach, we favor a retro-auricular incision. The posterior approach minimizes visible scars and postoperative contour deformities and allows the harvest of perichondrium and soft tissue at the same time to use as a thin onlay graft.
Key steps in performing the procedure are as follows: First, place the incision high (laterally) on the retroauricular surface, avoiding placement in the auricular-temporal sulcus, which can produce a problematic incisional scar that traps epidermal debris (figure 1, A). Use copious amounts of epinephrine-containing local anesthetic posteriorly to produce a vasoconstricted field, but avoid injecting it into the anterior surface, which can result in a hydraulic fracture of the cartilage.
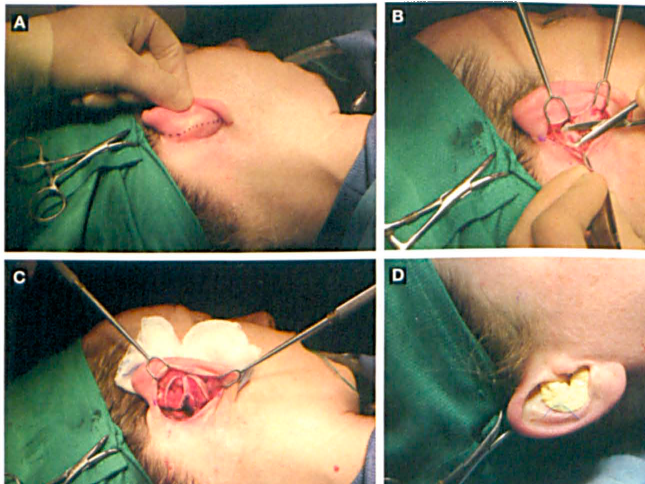
Next, elevate the flaps, exposing the perichondrium of the posterior auricular cartilage. This is easily performed using a pair of tenotomy scissors (figure 1, B). Some surgeons dissect in a subperichondrial plane, but we prefer to leave the perichondrium attached, which provides strength to the cartilage, or it can be carefully removed from the cartilage grafts after harvest.
The greater portion of both the concha cavum and cymba may be harvested. It is important to leave a strut of cartilage below the crus of the helix to maintain the shape and structural integrity of the ear and avoid deformity (figure 1, C) The cartilage is carefully freed from the anterior perichondrium, leaving it intact.
The incision is closed with one or two buried dissolvable sutures while the skin is approximated with 6-0 gut horizontal mattress sutures. A Xeroform gauze bolster is secured with a transcutaneous 2-0 suture on a large straight needle (figure 1, D); the bolster is removed in 6 days. This prevents the formation of seromas and helps ensure that the normal auricular contour is maintained.
The cartilage grafts can be shaped as needed (figure 2). We have achieved good graft retention by leaving the posterior perichondrium intact, which improves suture retention strength. The perichondrium can be carefully stripped from the cartilage to use as a facial onlay graft.

Cartilage grafts can be shaped as needed. On the left are perichondrial grafts; on the right, cartilage grafts from the concha cavum and cymha.
Patients are typically pleased with the well-hidden incisional scar (figure 3, A) and normal auricular contour (figure 3, B) after auricular graft harvest. Most patients will note that the ear is tender for 6 to 12 weeks after the resection, although pain is not a common complaint.
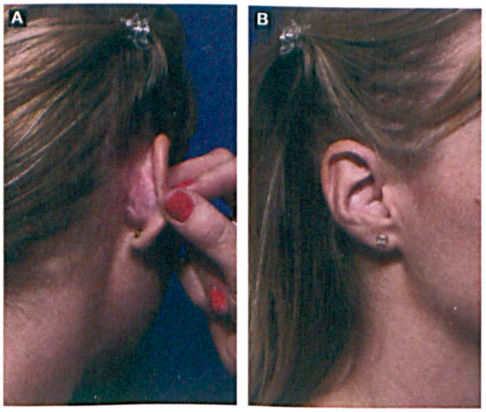
Patients appreciate the well-hidden incisional scar (
Using this technique, we have had only one seroma and one occurrence of a keloid in more than 400 cases.