
Abstract

Endoscopic treatment for Zenker diverticulum (ZD) has become the method of choice in most patients.1,3 The endoscopic technique is faster and safer, allows early resumption of diet, and reduces hospital stays. 4 The critical aspect of all endoscopic techniques is the accomplishment of a complete cricopharyngeal (CP) myotomy. In most cases, dividing the cricopharyngeus muscle provides excellent symptom relief and allows the pouch to empty completely with swallowing.
The CP myotomy method varies. Originally, Dohlman and Mattsson described the use of electrocautery to divide the diverticular-esophageal party wall. 5 CO2 laser division, originally described by van Overbeek, has been widely reported, as have stapler-assisted techniques using disposable surgical devices (EndoGIA-30 Stapler; U.S. Surgical Corp.; Norwalk, Conn.).6–8 The advantage of the stapling device is that it simultaneously divides and seals the party wall between the esophagus and diverticulum by cutting between a double row of staples. Sealing of the divided party walls is thought to reduce complications such as perforation and leakage of intraluminal contents resulting in mediastinitis.4,8
Access is one of the limiting factors in endoscopic ZD surgery. If the patient has unfavorable anatomy, trismus, or poor range of motion of the cervical spine, then placement of rigid endoscopes may prove difficult. Furthermore, if the pouch is shallow (<2 cm), the use of a stapling device is limited because the jaws of the stapler cannot fit around the small party wall/cricopharyngeus muscle. Options available for dividing the CP in this instance include electrocautery and the CO2 laser, which do not seal the mucosal defect and risk thermal injury to surrounding tissue.
Fama et al recently described use of the harmonic scalpel for division of the CP. 3 Harmonic scalpels utilize high-frequency sound wave oscillations to disrupt tissues and coagulate at low temperatures. Harmonic devices have been used in neck dissection, thyroidectomy, glossectomy, and parotidectomy. Sharp et al report a series comparing stapler-assisted to harmonic scalpel division in 50 patients. 2 No difference in complications was noted; however, the harmonic device was used in statistically smaller pouches. 2
We have employed a harmonic scalpel device (Harmonic ACE; Ethicon Endo-Surgery, Inc.; Cincinnati, Ohio) for endoscopic CP myotomy in several patients with a small (<2 cm) pouch. Our initial experience suggests that the harmonic scalpel is safe, easy to use, and provides excellent visualization for CP myotomy in patients with a small ZD. The device can be deployed multiple times, if needed, and seals the opposing mucosal edges, reducing the risk of mediastinal leak.
The procedure is performed under general anesthesia with a small endotracheal tube. The patient is laid supine with his or her head supported on a head ring. The teeth are protected with a rubber mouthguard. Our preference is to use either the Weerda Distending Diverticuloscope (Karl Storz; Tuttlingen, Germany) or the Holinger-Benjamin Slimline Diverticuloscope (Karl Storz; Tuttlingen, Germany). The Slimline diverticuloscope provides improved access for patients with a difficult exposure. The lumen of the Slimline is smaller and cannot accommodate a stapling device. The harmonic scalpel, however, fits easily through the device.
Once the bar is isolated, the microscope is positioned (figure 1, A) and the pouch suctioned of debris and inspected. The device is introduced to the level of the CP (figure 1, B). Under microscopic or endoscopic visualization, the jaws are positioned on either side of the CP muscle, and the device is closed and activated. The myotomy site is inspected for completeness and sealing of the wound edges (figure 2). If necessary, a second activation can be performed to divide any remaining CP fibers.
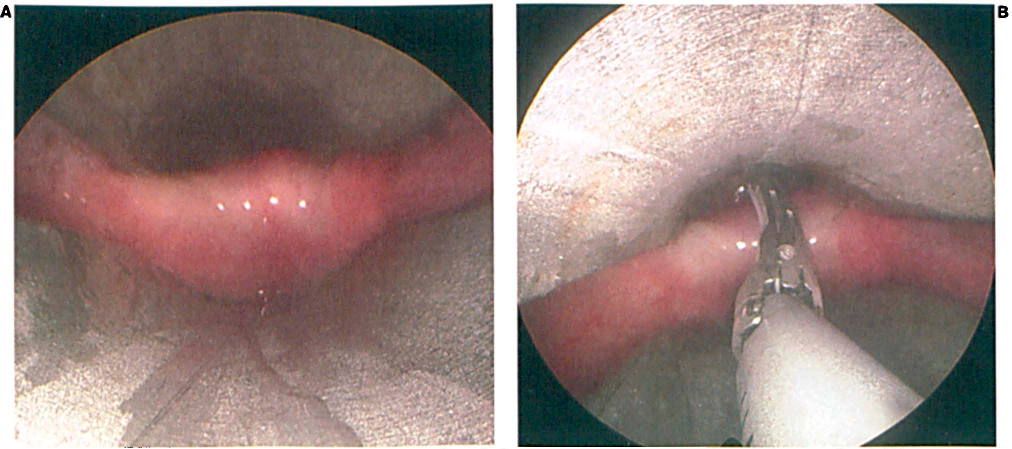
The Cricopharyngeus Muscle is Exposed with the Diverticuloscope (
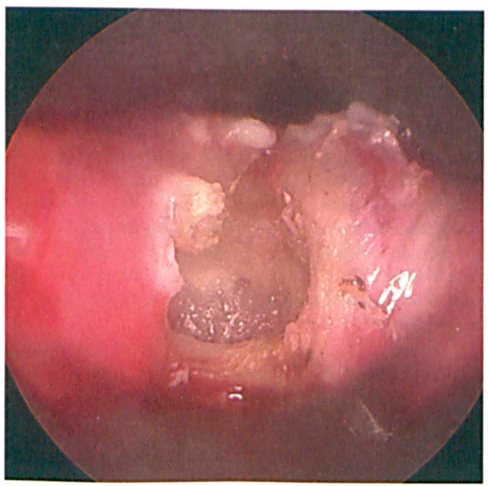
Endoscopic View Shows Intact Buccopharyngeal Fascia after Completion of the Myotomy.
Patients remain in the hospital overnight for observation. If they are afebrile and without chest pain or subcutaneous emphysema the following morning, they are discharged home on a liquid-puree diet for 1 week, increasing to a full diet the following week.