
Abstract
Extramedullary plasmacytomas most commonly occur in the nasal cavity, nasopharynx, paranasal sinuses, and larynx. Thyroid involvement is rare, as fewer than 75 cases have been previously reported in the literature. We report a new case of disseminated plasmacytoma of the thyroid, which occurred in a 68-year-old woman. The diagnosis was made with an incisional biopsy. The patient initially experienced a complete response to radiotherapy (46.8Gy in 26 fractions), but she developed multiple metastases at distant sites, including the breast, abdominal wall, and buttock despite various chemotherapy regimens. Ultimately, she was placed on palliative radiotherapy. We also briefly review the diagnostic and treatment options for patients with extramedullary plasmacytoma.
Introduction
Extramedullary plasmacytomas are immunoproliferative monoclonal B-cell malignancies. These tumors may occur as either a solitary plasmacytoma or as a manifestation of multiple myeloma. They account for about 3% of all plasma cell tumors and 1% of all head and neck tumors. 1
Eighty percent of extramedullary plasmacytomas occur in the head and neck—within mucosal and submucosal lymphoid tissue. 1 The most common sites include the nasal cavity, nasopharynx, paranasal sinuses, and larynx. Plasmacytomas of the thyroid gland are rare; to the best of our knowledge, fewer than 75 cases have been previously reported in the international literature. In this article, we report a new case of thyroid plasmacytoma that developed into systemic disease.
Case report
A 68-year-old woman with a history of hypothyroidism presented to our institution with a midline neck mass and associated dysphagia. She had no history of irradiation. Her family history was significant for her brother having had lymphoma.
Physical examination revealed nodularity of the lower neck without adenopathy. Ultrasonography demonstrated a multinodular thyroid gland with a dominant 4.7-cm nodule on the left. Fine-needle aspiration biopsy yielded an atypical lymphoplasmacytic infiltrate without any identifiable thyroid tissue. Noncontrast computed tomography (CT) of the neck showed that the thyroid mass had caused tracheal deviation (figure 1). A total thyroidectomy was offered for diagnostic and therapeutic reasons.
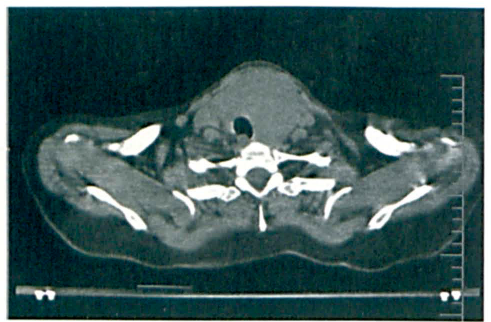
Noncontrast axial CT of the neck shows the tracheal deviation.
In the operating room, the thyroid gland was found to be very adherent to the strap muscles; extensive neovascularization was also found. Frozen-section analysis suggested that a malignancy was invading the muscle—possibly a lymphoma, plasmacytoma, or medullary or anaplastic carcinoma. The operation was concluded after incisional biopsy.
Permanent pathology identified the mass as an extramedullary plasmacytoma (figure2). Flow cytometry revealed 67% B cells with kappa light-chain restriction and CD 19+ and CD38+ expression. Serum immunofixation revealed an elevated IgG level with monoclonal gammopathy; no monoclonal gammopathy was evident in the urine. The medical and radiation oncology services were consulted. The results of a bone survey were normal, and a bone marrow biopsy yielded no evidence of multiple myeloma. The patient was administered definitive radiotherapy with 46.8 Gy in 26 fractions.
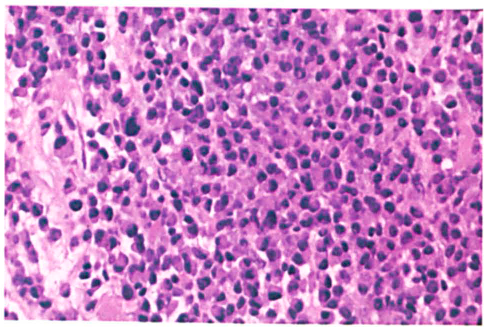
Biopsy shows the cells with plasmacytoid features (H&E).
Initially, the patient experienced a complete clinical and radiographic response. However, 2 months after the cessation of treatment, she developed multiple subcutaneous nodules in her left breast, abdominal wall, and buttock. CT showed no lung, hepatic, or adrenal metastasis. A core biopsy identified the breast nodule as a metastatic plasmacytoma. The patient was started on thalidomide and dexamethasone for disseminated disease. Again, she responded initially, but her nodules recurred 3 months later. She was switched to bortezomib, a proteasome inhibitor, but her disease continued to progress. She was treated next with high-dose cyclophosphamide and an autologous stem cell transplant, and her nodules regressed completely. Unfortunately, nodules eventually developed in her right breast, and she was started on dexamethasone and lenalidomide; the latter is a member of a newer class of immunomodulatory drug. Yet her disease continued to progress, and 14 months after diagnosis of her disseminated disease, she was started on palliative radiotherapy.
Discussion
The differential diagnosis of a neoplasm with plasmacytoid features should include a poorly differentiated carcinoma, lymphoma, melanoma, paraganglioma, and other neuroendocrine neoplasms. Extramedullary plasmacytomas are more common in men than in women, and their peak incidence occurs in the sixth decade of life. 2 Serum protein electrophoresis, a urinalysis for Bence Jones protein, a skeletal survey, and a bone marrow biopsy should be performed to rule out multiple myeloma. Monoclonal gammopathy occurs in about one-half of patients with extramedullary plasmacytoma. Autoimmune thyroiditis has been associated with plasmacytoma confined to the thyroid gland. 3
No randomized clinical trials have been conducted to determine the optimal treatment for extramedullary plasmacytoma. The current management strategy is to administer a moderate dose of radiotherapy (40 to 50 Gy administered continuously once daily at 1.8 to 2.0 Gy/fraction). 4 Elective irradiation of the cervical nodes is controversial, and this decision is currently made on an individualized basis. Surgery may be successful in eradicating the occasional well-localized tumor if no functional deficit is expected. Aggressive subtotal resection followed by postoperative radiotherapy offers no advantage in terms of local control; local control rates after radiation alone and after surgery alone are similar, ranging from 80 to 90%. 4 Although there is no evidence that adjuvant chemotherapy improves local control or survival, it may be beneficial in patients with recurrent or disseminated disease.
If serum and/or urine levels of monoclonal proteins are initially elevated, periodic retesting may be helpful in assessing the response to treatment and in monitoring for recurrence. 5 Most recurrences manifest as progression to multiple myeloma. Such progression has been reported to occur months to years after diagnosis in approximately one-third or less of patients with extramedullary plasmacytoma. 6 Survival at 10 years is 70%, and it is related to progression to multiple myeloma. 6 Therefore, long-term follow-up should be extended to these patients.
The treatment for disseminated plasmacytoma may include melphalan (an alkylating chemotherapeutic agent) and VAD (vincristine, doxorubicin [Adriamycin], and dexamethasone). In addition to high-dose chemotherapy, stem cell transplantation may be employed. Other drug therapies may include bortezomib, the immunomodulators thalidomide and lenalidomide, and inhibitors of fibroblast growth factor receptor 3, insulin-like growth factor 1 receptor, and vascular endothelial growth factor. These noncytotoxic biologicals have been shown to be active and tolerated by patients with recurrent and/or refractory disease. 7 In fact, bortezomib and lenalidomide have been approved by the federal Food and Drug Administration as a treatment for recurrent myeloma. Other treatment options include radiotherapy and supportive care. The mechanism of metastasis to subcutaneous tissues is not well understood.