
Abstract
Kimura disease is an uncommon chronic, benign, inflammatory condition of unknown etiology. It occurs endemically in Asia and sporadically in the West. Because it often imitates neoplastic or inflammatory processes of the head and neck, otolaryngologists and head and neck surgeons should be aware of its clinical presentations. In this article, the author reports 2 cases of Kimura disease—1 that was characterized by an unusual bilateral presentation and 1 that was managed conservatively—and he briefly reviews the literature on this entity.
Introduction
Kimura disease is a rare idiopathic condition that usually affects adolescent boys and young men of Asian descent.1–3 It is a form of chronic inflammatory disorder that involves subcutaneous tissue, primarily in the head and neck, and it is frequently associated with lymphadenopathy and/or salivary gland enlargement. 1 The only reported systemic manifestation is renal involvement leading to nephrotic syndrome.2,4,5
Bilateral involvement is rare. 3 In this article, the author reports a case of Kimura disease that manifested as bilateral postauricular masses and another case that manifested as a submandibular swelling. He also provides a brief review of the literature.
Case Reports
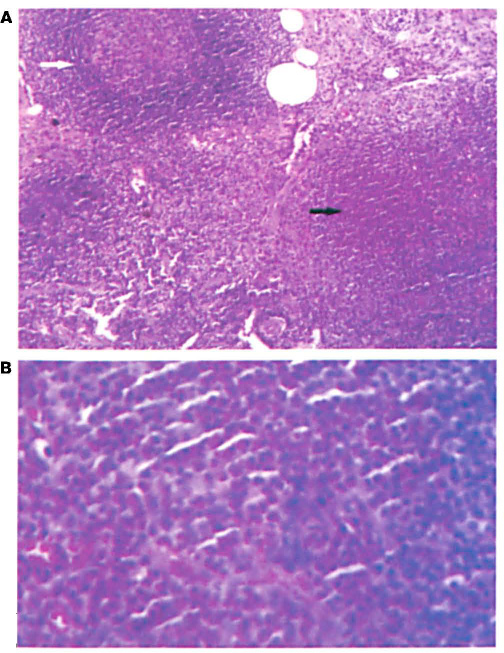
With the patient under local anesthesia, an excision biopsy was performed on the left-sided mass. The resected specimen was found to be a firm, enlarged lymph node. Histopathologic examination of the node revealed reactive germinal follicles (figure 1, A). Interfollicular areas were expanded by a dense eosinophilic cell infiltrate that formed abscesses in places (figure 1, B). The specimen was reported as Kimura disease. A follow-up blood examination revealed an eosinophil concentration of 21% and a serum IgE level of 650 IU/ml (normal: <150). A urine protein estimation and renal function test results were normal.
Patient 1.
The right-sided mass was excised 15 days after the left-sided excision, and the histopathologic findings were similar. The patient was followed up for 1 year, and he showed no evidence of recurrence.

Patient 2. Photograph shows the swelling in the right submandibular area at presentation.
A biopsy of the mass was done with local anesthesia. Histopathology of the specimen identified it as a follicular hyperplasia that involved the skin and salivary gland, with diffuse proliferation and eosinophilic infiltration. Occasional eosinophilic abscesses were seen. Based on these characteristic histopathologic features, a diagnosis of Kimura disease was established. Follow-up blood testing revealed an eosinophil concentration of 18% and a serum IgE level of 960 IU/ml. The results of renal function testing were normal.
The patient was not willing to undergo surgery, so he was started on oral prednisolone at 1 mg/kg in a tapered dose over 4 weeks. One month later, he returned for follow-up with a marked reduction in the size of the swelling. During 3 months of continued follow-up, he exhibited no increase in the size of the swelling and his renal function test results were normal. We decided to maintain a conservative approach to management and further treat the patient only if the mass resumed growing or caused a significant deformity.
Discussion
Kimura disease was first described in China in 1937 by Kimm and Szeto, who called it an eosinophilic hyperplastic lymphogranuloma. 6 In 1948, Kimura et al described it as an abnormal granuloma with proliferation of lymphoid tissue. 7 In 1959, Iizuka named the disease after Kimura. 8
Clinical features
Kimura disease is most commonly seen in Chinese and Japanese males in the second and third decades of life.1-3, 9,10 Sporadic cases have been reported in non-Asians. 1 The most common clinical feature of Kimura disease is a painless unilateral soft-tissue mass in the head and neck; a major salivary gland and lymph nodes are frequently involved, as well. Kimura disease is associated with eosinophilia and an increased level of serum IgE.1-3 It has predilection for the scalp and periauricular area. 11 Infrequently, axillary, inguinal, and epitrochlear lymph nodes are involved.2,10 In some cases, isolated lymphadenopathy is the only manifestation of Kimura disease. 1 It may mimic an inflammatory or neoplastic lesion.1,3,9,12
In 1999, Hiwatashi et al were the first to report a case of Kimura disease presenting as bilateral auricular masses. 3 In 2005, Tseng et al reported a rare case of Kimura disease presenting as bilateral parotid masses. 13 Kimura disease should be suspected when a patient—particularly an Asian male—exhibits the clinical triad of a painless head or neck mass, eosinophilia, and an elevated IgE level.2,12
Kimura disease is a distinct reactive process. Its etiology and pathogenesis are unclear.3–5,11 Among the possible causes that have been postulated are trauma, an abnormal autoimmune reaction, and an allergic reaction to a parasite, virus, fungus, or toxin.1,3 The presence of peripheral eosinophilia and an elevated IgE level suggest an abnormal T-cell stimulation to a hypersensitivity reaction.1,3,4 Kimura disease is a benign chronic disorder with an indolent clinical course that frequently waxes and wanes over time. 1 Left untreated, these masses tend to slowly enlarge, and they may eventually become disfiguring. Over the long term, affected patients appear to do well, although about 10% develop a steroid-responsive nephrotic syndrome. 2
Diagnosis
The differential diagnosis of Kimura disease includes such entities as eosinophilic granuloma, Mikulicz disease, acute nonlymphocytic leukemia, Hodgkin disease, follicular lymphoma, angioimmunoblastic lymphadenopathy, and angiolymphoid hyperplasia with eosinophilia. 2 Despite its rarity, Kimura disease should be considered in the differential diagnosis of any lymphadenopathy that demonstrates an eosinophilic infiltrate and prominent follicular hyperplasia. Since Kimura disease is a distinctive clinicopathologic entity with characteristic histologic features, it is important to distinguish it from a drug reaction, hypersensitivity, or response to infectious agents. 1
The spectrum of cytologic features observed in Kimura disease on fine-needle aspiration are nonspecific and similar to those seen in a variety of other lesions. 12 While the diagnosis may be suggested by fine-needle aspiration, it is established by biopsy. 9 Pathologically, nodular lesions usually affect the lymph nodes, although skin or salivary tissues are occasionally affected. The normal tissue architecture is usually preserved, but follicular hyperplasia of lymphoid tissue with infiltration of lymphocytes, histiocytes, and large numbers of eosinophils is typical. Germinal centers may be necrotic and feature central eosinophilic abscesses. 2
Treatment
Management strategies range from conservative observation for asymptomatic patients to surgical excision, steroid therapy, or radiotherapy for symptomatic patients. 5 Complete surgical excision whenever feasible is the preferred treatment.2,9,11 Resection may be effective in permanently eradicating a mass if the entire lesion can be removed, but complete resection can be difficult because of the diffuse nature of the disease.
Local irradiation has also been shown to be effective in shrinking the lesion, but radiation is generally not advocated for younger patients.2,10 Radiotherapy may be considered for recurrent cases. 3 Systemic and intralesional corticosteroid therapy has been shown to reduce the size of lesions, but tumors tend to recur when steroids are discontinued.1,2,10 In fact, recurrences are common with all modalities of treatment (15 to 40%), although the relapse rate is lower when two or more therapies are combined.1-3,10,12 Watchful waiting may be preferred for selected patients, with treatment being instituted only if the mass continues to grow or causes a significant deformity. 2 These lesions are not fatal and they do not undergo malignant transformation. However, many patients with Kimura disease develop renal involvement.2,4,5
The case of patient 1 described herein was exceptional for three reasons: (1) the disease presented as a primary lymphadenopathy, which is unusual considering the diffuse nature of Kimura disease; (2) there was bilateral involvement; and (3) the findings on histopathology led us to perform a retrospective investigation to arrive at the diagnosis.
Otolaryngologists and head and neck surgeons in the West should be aware of Kimura disease, especially in view of the growing number of susceptible Asian males who live in the West and because sporadic cases have been reported in non-Asians. 1 It should be strongly considered in any patient who presents with a painless head or neck mass in association with marked eosinophilia and an elevated serum IgE level.