
Abstract
Lymphangioma is an uncommon benign pathology, usually reported in children and rarely in adults. In the past, the definitive diagnosis was made intraoperatively and was usually an unexpected finding. However, with today's modern imaging technologies, such as computed tomography and magnetic resonance imaging, the diagnosis can he assumed before intervention, even though the final diagnosis still can be reached only via histopathologic examination. Imaging techniques also can aid in the precise mapping of the lesion and in defining its boundaries with the surrounding vital structures, improving therapeutic success. Various therapeutic options are reported in literature, but complete surgical excision is still considered the best approach. We report a case of cervical lymphangioma of unknown etiology in an 18-year-old man and discuss the presentation, diagnosis, and management of this lesion.
Introduction
Cervical lymphangioma is a benign hamartomatous hyperplasia of lymphatic vessels, and it accounts for up to 90% of all lymphangiomas in the head and neck region. 1 It occurs most frequently in the posterior triangle, but when it occurs in the anterior triangle, it tends to be more problematic, interfering with the patient's ability to breathe or swallow.
Cervical lymphangioma is well recognized in pediatric practice but seldom presents de novo in adulthood. It usually presents as a progressive and painless growth, although occasionally growth may be sudden. Diagnosis in children is usually straightforward, but it can be problematic in adults because of its rarity. Clinical features, together with a high index of suspicion and computed tomography (CT) or magnetic resonance imaging (MRI) findings, can aid in the diagnosis of these neck masses. The final diagnosis is based on postoperative histopathology.
Surgical excision remains the most widely accepted treatment2,3; surgical removal is technically less difficult in adults than in children. However, when the lesion infiltrates vital neurovascular neck structures, complete excision is difficult. If only partial excision is achieved, the recurrence rate is between 15 and 53%. 4
Case Report
An 18-year-old man was referred to our hospital with a history of a right-sided neck mass present for 1 year that had increased in size over the previous few months. The patient was completely asymptomatic apart from the cosmetic aspect of the mass. It was mainly the rapid increase in size that prompted the patient to visit his general surgeon.
The surgeon planned excision of the mass but perioperatively encountered profuse bleeding and hence abandoned the procedure and referred him to our hospital. On clinical examination, a smooth-surfaced, diffuse, firm, nontender, immobile swelling measuring 5 × 4 cm was found in the right posterior triangle, It was nonpulsatile, with no regional lymphadenopathy. A 2-cm horizontal scar was visible over the neck mass (figure 1).

Photograph Shows the Right-Sided Swelling and Scar in the Patient's Neck.
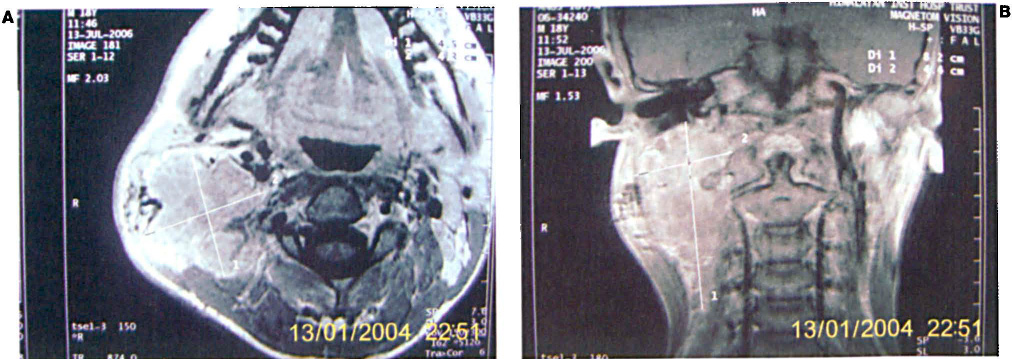
Cytology performed in the pathology clinic demonstrated lymphoid cells but no malignant cells. MRI showed a lobulated mass in the right posterior cervical region of the neck (figure 2, A). The mass exhibited intermuscular plane extension with multiple hemorrhagic levels (figure 2, B), and mild heterogenous enhancement with no intrathoracic extension. A provisional diagnosis of cervical lymphangioma was made.
The mass was excised under general anesthesia. Intraoperative findings revealed a lobulated mass extending beneath the sternocleidomastoid and adhering to the surrounding structure (figure 3). The postoperative period was uneventful, and the histopathology report confirmed the diagnosis of lymphangioma. The patient was disease-free at the 2-year follow-up.
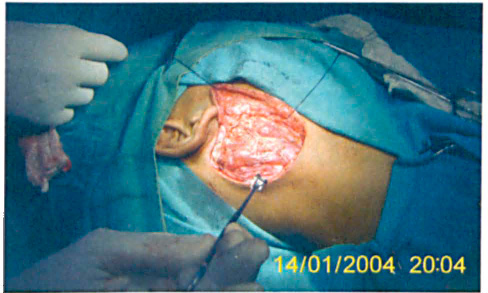
Intraoperative Photo Shows the Lobulated Appearance of the Mass.
Discussion
Lymphangiomas are malformations of the lymphatic system, the majority of which appear in the head and neck area, particularly in the posterior triangle. Other common sites include the axilla, chest wall, shoulder, mediastinum, abdominal wall, and thigh.
These lesions can be classified in to four categories: superficial cutaneous lymphangioma (composed of small, thin-walled lymphatics), cavernous lymphangioma (composed of dilated lymphatic vessels with surrounding adventitia), cystic lymphangioma (consisting of huge, macroscopic lymphatic spaces with surrounding fibrovascular tissues and smooth muscle), and diffuse systemic lymphangioma (in which lymphatic channels appear to be dissecting dense collagen bundles). 5 These categories are somewhat artificial, however; many lesions are combinations of the four types.
Cervical lymphangioma accounts for up to 90% of all lymphangiomas in the head and neck region. 1 This lesion occurs in regions with a predominance of fascial planes and lax tissue, such as the neck, where it can expand and create large cystic spaces. Depending on the cystic space size, cervical lymphangiomas are classified as macrocystic, microcystic, or mixed.4,5 In our patient, the lesion was of the mixed type.
In congenital cases of cervical lymphangioma, the most prominent sign is a mass, which can be present at birth or noticed later, usually in the first 5 years of life. The lesion can be completely asymptomatic or can present with mechanical symptoms of respiratory obstruction, dysphagia, and/or feeding problems, as well as associated infection, abscesses, or sepsis. The diagnosis of cervical lymphangioma is usually made easily when the lesion is noted at birth. The mass is generally soft, fluctuant, and transilluminating.
In adults, the diagnosis can be more difficult to determine and depends on a high index of suspicion. The differential diagnosis includes branchial cyst, thyroglossal cyst, dermoid cyst, lipoma, laryngocele, thyroid mass, and hemangioma. Only a few cases in adults have been reported in the literature, suggesting an acquired rather than a congenital etiology. Kennedy et al, in their large, retrospective review of 46 patients with cystic lymphangioma, found four possible cases with acquired causes. 6 Such causes can include trauma, infection, and neoplasia, or they can be idiopathic or iatrogenic. In the two adult acquired case series of cervical lymphangioma reported in the literature, an asymptomatic mass or an unexpected intraoperative finding was the most common presentation of cervical lymphangioma.7,8
Although cervical lymphangioma tends to enlarge progressively over months, a relatively rapid increase in size has also been described, 9 as was seen in our patient. In adults, the sudden appearance is frequently related to a history of trauma or acute infectious processes in the upper respiratory tract.10,11 In our case there was no history of this nature; therefore, we consider the etiology unknown.
CT or MRI can aid in the diagnosis and define the extent of the lesion and its surrounding vital structures. MRI in particular can give a clear definition of the structures involved, which is useful in the planning of surgery. Many authors stress the importance of preoperative imaging to look for intrathoracic extension, which is present in 10% of cases. 12 In our patient, we performed MRI to determine the depth and extension of the lesion, including a thoracic study to rule out any possible extension to the mediastinum. Fine-needle aspiration cytology (FNAC) is also essential to confirming the final diagnosis. In our case, the FNAC result coincided with the final pathology report of lymphangioma.
The most acceptable management approach to cervical lymphangioma is complete surgical excision of the lesion, although a careful wait-and-see policy may be indicated in a few asymptomatic cases, as spontaneous regression has been reported. 5 Surgical success is improved by preoperative CT/MRI imaging. When excision is complete, the lesion rarely reappears. However, when the lymphangioma infiltrates important vascular and nerve structures, complete excision is difficult and the recurrence rate can be as high as 50%.3,4 Such recurrences generally take place within 1 year, and they are often associated with an upper respiratory tract infection. 13 Therefore, a 2-year postsurgical follow-up period is recommended. Postoperative complications (e.g., infections, fistulae, anti-aesthetic scars, etc.) are frequent, occurring in 19 to 33% of cases. 14
Other treatment modalities include aspiration, radiation, and intralesional injection of sclerosing agents such as fibrin sealants, triamcinolone, bleomycin, hydrocolloid dental impression material, and the agent OK-432. OK-432 is derived from a strain of Streptococcus pyogenes and has been used successfully, especially in macrocystic lymphangiomas and in patients who are at increased risk from anesthesia. 15
In conclusion, cervical lymphangioma, although rare in adults, should be included in the differential diagnosis for a neck swelling in an adult. Surgical removal is technically less difficult in adults than in children. Preoperative imaging is essential to the successful management of these lesions. Our case was unusual in that a large cervical lymphangioma presented de novo in an adult with no history of trauma or upper respiratory infection. Complete excision was successful, and the patient's prognosis is good.