
Abstract
We report an unusual case of hypocalcemia and respiratory distress related to acid-suppressive therapy. The patient was a 50-year-old woman with bilateral laryngeal paralysis and hypoparythyroidism resulting from a thyroidectomy performed more than 30 years previously. She required large doses of calcium supplementation to maintain a normal calcium level. Her airway had been marginally adequate. A few weeks prior to presentation, she began to experience increasing dyspnea. Examination was suggestive of laryngopharyngeal reflux, and she was started on a therapeutic trial of esomeprazole 40 mg twice daily. Three days later, she presented to the emergency room with airway distress. Laboratory studies indicated that the patient had hypocalcemia. The esomeprazole was discontinued, and she was treated with intravenous calcium; her symptoms resolved. We attribute the airway distress to tetany in synkinetically reinnervated laryngeal adductor muscles. We recommend that acid-suppressive therapy should be used with caution in patients with hypoparathyroidism or hypocalcemia.
Introduction
Proton pump inhibitor (PPI) therapy has found a strong niche in the armamentarium of the practicing otolaryngologist, as gastroesophageal reflux disease (GERD) and laryngopharyngeal reflux (LPR) have been implicated in several otolaryngologic conditions, including otitis media, sinusitis, and laryngitis.1,2 Development of vocal fold granuloma has been similarly regarded as a manifestation of GERD. 3 LPR produces characteristic symptoms that may include frequent throat clearing, mild dysphonia, cough, globus, vocal fatigue, or cervical dysphagia.4,5 LPR is found in 75% of patients with asthma, and treatment with a PPI provides improvement in both asthma and LPR symptoms. 6
Acid suppression is not without risk. Gastric–acid–suppressive therapy has been associated with increased risk of community-acquired pneumonia; it was postulated that this increased risk might be attributed to an elevated gastric pH. 7 Furthermore, use of acid-suppressive agents, particularly PPIs, has been associated with increased risk of community-acquired Clostridium difficile infection.8,9 More recently, long-term PPI therapy has been associated with an increased risk of hip fracture. 10 We report an unusual complication of hypocalcemia related to PPI therapy, and briefly review the literature to further elucidate this problem.
Case Report
A 50-year-old woman presented to our clinic with complaints of dyspnea that had been worsening. A few weeks earlier, she had noted that she became winded when going up stairs, and the problem had been increasing. Her airway was adequate at rest. She had a history of follicular carcinoma of the thyroid that had been treated with total thyroidectomy when she was 16 years of age. This was complicated by long-standing hypoparathyroidism and bilateral vocal fold paralysis. Her vocal fold paralysis had been treated with arytenoidectomy and a vocal fold medialization procedure more than 10 years earlier. Her airway, although not normal, had been stable and adequate for her activity level for many years, and her long-standing hypoparathyroidism and hypocalcemia had been treated with 0.25 μg of calcitriol and 2.8 g elemental calcium daily for many years, as well.
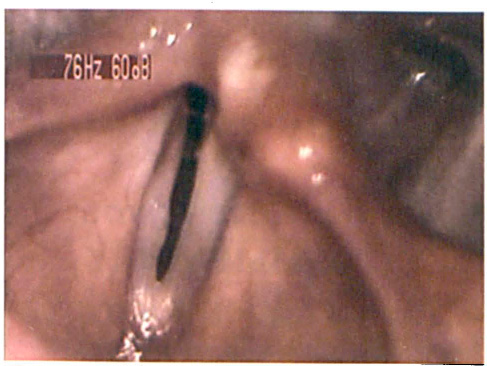
Flexible laryngoscopy revealed bilateral vocal fold motion impairment with a narrow glottic chink. No inspiratory abduction on either side was observed, but there was phonatory adduction of the left vocal fold, and with deep inspiration there was some paradoxic adduction of the right vocal fold. The interarytenoid region was erythematous and edematous, and mucus was stranding between the vocal processes (figure). It was postulated that edema from LPR was compromising her marginal airway.
The patient was started on a therapeutic trial of esomeprazole 40 mg twice a day. On the third day of treatment, she began to experience parasthesias in her hands, which quickly evolved into respiratory distress with stridor. She was taken to the emergency room and found to have an ionized calcium level of 0.8 mmol/L (normal range: 1.1 to 1.4 mmol/L) and a total calcium level of 6.4 mg/dl (normal range: 8.4 to 10.5 mg/dl). It was recognized that the esomeprazole was interfering with her calcium absorption.
The patient's hypocalcemia was treated with intravenous calcium and magnesium, and the esomeprazole was discontinued. The patient's symptoms abated, with no recurrence of hypocalcemia at the 1-year follow-up. Her airway is still marginal, but adequate for most daily activities.
Discussion
Our case illustrates the need for caution in prescribing acid-suppressive agents in patients with a history of hypoparathyroidism. Calcium absorption is pH-dependent and decreases significantly in the presence of achlorhydria.11,12 A previous report described hypocalcemia and tetany in a patient with a previous subtotal thyroidectomy who had been treated with lansoprazole for GERD. 13 Our case, to our knowledge, is the first report of PPI-related hypocalcemia with associated stridor. Laryngospasm is a recognized complication of hypocalcemia; however, our patient had bilateral laryngeal paralysis. She had been noted to have inspiratory laryngeal adduction on her examination prior to beginning esomeprazole, indicating that she had synkinetic reinnervation rather than complete denervation.
Figure. Image of the patient's larynx at the time of the initial laryngoscopy demonstrates interarytenoid edema and erythema with associated mucus stranding between the vocal processes.
Hypocalcemia is one of the most common complications of thyroid surgery. Many patients require large doses of calcium supplements to maintain a normal blood level of calcium. Therefore, it is logical that any agent that impairs calcium absorption could result in hypocalcemia. Animal studies have demonstrated 100% mortality due to hypocalcemia in rats that are rendered hypoparathyroid and then undergo gastrectomy and fundectomy. In contrast, no mortality was observed in rats with parathyroidectomy alone. 14
Clinical studies have shown that elderly women on calcium carbonate supplements and PPIs show significantly decreased calcium absorption after an overnight fast and on an empty stomach. 15 Also, an increased risk of hip fractures has been reported in patients on long-term therapy with PPIs. 10 However, another study reported that patients on PPIs were able to absorb calcium from foods without any evidence of malabsorbtion. 16 These findings indicate that hypocalcemia and/or bone loss are potential complications of PPI therapy. It would be prudent to avoid PPIs in patients with a history of hypoparathyroidism or, at the very minimum, to use them with caution.
If PPIs are prescribed for patients who require calcium supplements, the calcium should be taken with food to improve absorption. 17 In patients with osteoporosis, PPI could hasten bone resorption and increase the risk of fracture. Therefore, caution should be used in these patients, as well, with PPI therapy limited to the shortest possible duration and the lowest effective dose. Guidelines need to be established for monitoring serum calcium and/or bone density during PPI therapy. Furthermore, if taking PPIs and calcium carbonate supplements is necessary, again, the calcium should be taken with food to avoid malabsorption.
LPR requires more frequent and intensive PPI therapy than that used to treat GERD. Therefore, the risk of calcium malabsorption is likely to be proportionally higher. It is imperative that risk factors such as hypocalcemia and hypoparathyroidism be taken into account in these patients. Furthermore, recent reports of increased risk of hip fractures, 10 community-acquired pneumonia, 7 and community-acquired C difficile infection8,9 suggest that PPI therapy may not be so innocuous. It is recommended that patients on long-term PPI therapy be monitored, and that PPI be limited to the shortest duration and lowest effective dose.