
Abstract
Ameloblastomas are locally aggressive gnathic tumors with a high propensity for recurrence. Presentation of an ameloblastoma exclusively in the sinonasal tract is extremely rare, with few reported cases in the literature. Management involves surgical excision and close follow-up. We report a case in which the patient had complete unilateral nasal obstruction caused by an ameloblastoma. The tumor was completely excised endoscopically, and at the 12-month follow-up, there was no evidence of recurrence.
Introduction
Ameloblastoma is a benign odontogenic tumor, usually occurring in the maxilla or mandible. 1 Presentation exclusively in the sinonasal tract is extremely rare, with few reported cases.2–5 Schafer et al reviewed nearly 20,000 sinonasal tumors over a 40-year period and reported only 24 cases of ameloblastoma. 6
The clinical presentation of odontogenic ameloblastoma is normally nonspecific (facial pain, numbness, toothache, mobile teeth, ill-fitting dentures, malocclusion, ulcerations) and is often asymptomatic and found incidentally on routine dental x-rays. Sinonasal ameloblastoma may present as sinusitis, nasal obstruction, and/or epistaxis.
Case Report
A 61-year-old man presented with a 3-month history of progressive left-sided nasal obstruction, recently associated with the discharge of blood-stained mucus. He had no associated history of epistaxis, pain, or anosmia and was otherwise healthy, with no previous sinonasal disease.
On presentation, the patient's left nasal cavity was completely obstructed by an exophytic lesion originating from the middle meatus. The lesion was smooth, lobulated, and had a vascular appearance. Biopsies were consistent with plexiform ameloblastoma. The patient subsequently underwent endoscopic resection of the tumor and middle meatal antrostomy. The tumor did not extend into the maxillary antrum.
The patient is currently on bimonthly follow-up, and at the 12-month follow-up there was no evidence of recurrence.
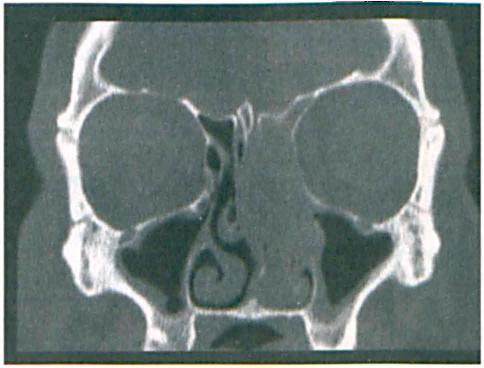
Coronal CT shows complete obstruction of the left nasal cavity by the ameloblastoma. The septum is deviated to the right, and the middle turbinate is completely obliterated.
Discussion
Sinonasal ameloblastomas are often indistinguishable from benign nasal polyps or chronic sinusitis on computed tomography (CT) (figure 1). Although the presence of unilateral involvement and bony erosion on CT should raise suspicion for ameloblastoma or inverted papilloma, because of the lack of pathognomonic radiologic characteristics, a definitive diagnosis of sinonasal ameloblastoma requires biopsy. In contrast to sinonasal ameloblastomas, ameloblastomas arising from the mandible have been reported to show irregular cortical sclerosis, well-defined edges, and cyst formation, and to exhibit an overlapping, multilocular soap-bubble or honeycomb appearance.
Although ameloblastomas originate from odontogenic epithelium, they do not progress to form enamel. Sinonasal ameloblastomas probably originate from the bony structure of the middle turbinates. Microscopically, the ameloblastoma is composed of nests, strands, and cords of ameloblastic epithelium, all separated by relatively small amounts of fibrous connective-tissue stroma. Two predominant patterns are seen: follicular and plexiform.
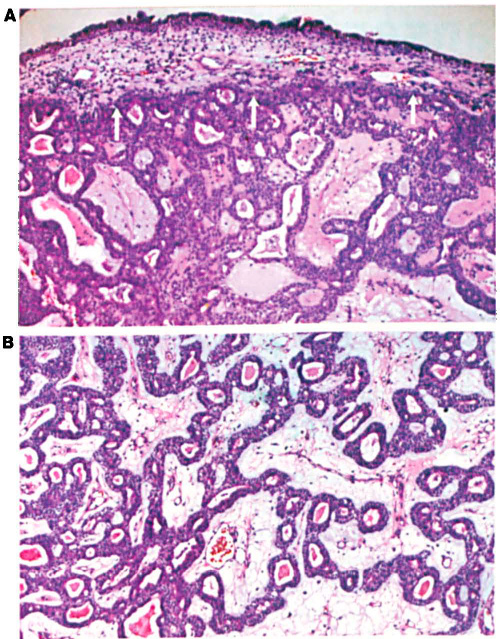
In the follicular form, the epithelial islands contain central portions composed of a loose network resembling that of the enamel organ. The epithelium at the periphery is composed of tall, columnar cells with hyperchromatic nuclei. In the plexiform type, the epithelium is arranged in interconnecting strands and cords of epithelium in loose, vascular, sparsely cellular connective-tissue stroma (figure 2). The epithelial cells are in close juxtaposition and appear basaloid or cuboidal. Other histologic subtypes also occur, often in the same tumor, including basal cell, granular cell, desmoplastic, and acanthomatous types.
Although this slow-growing tumor is benign, it is locally aggressive and has a high rate of recurrence. Malignant transformation has also been reported. 7
At the moment, there are too few reported cases to make a definite recommendation regarding treatment. There is no consensus on management, although radiotherapy seems to be of limited value. The combination of endoscopic removal and endoscopic surveillance in the outpatient setting is a less radical approach than radiotherapy while still resulting in decreased morbidity and better tumor control. Close periodic reassessment of the patient is mandatory.