
Abstract
An estimated 40 million people worldwide live with blindness, and a further 218 million live with moderate to severe visual impairments (Allen, 2019). Unlike other types of disability, people with visual impairments (i.e., those who are blind or have low vision) need more direct assistance from sighted people to manage health and illness in their daily lives (Bodenheimer et al., 2002). In addition to the individual's challenges in sensory dysfunction, various social and environmental factors are also contributing to unhealthy lifestyles and chronic illnesses (Hwang et al., 2009).
Compared to sighted people, people with visual impairments have multiple comorbidities and early mortality (Jacobs et al., 2005); they have higher rates of obesity, diabetes, cardiovascular disease, depression, and anxiety (Globe et al., 2005). Most chronic conditions are relevant to problematic health behaviors such as a lack of physical activity (Marmeleira et al., 2014), unhealthy eating behaviors (Bilyk et al., 2009), sedentary lifestyles (Surakka et al., 2008), weak social networks (Bhagotra et al., 2008), alcohol consumption (Weiland et al., 2014), and smoking (Weiland et al., 2014). In addition to these previous findings, low scores on health-related quality-of-life measures have been reported from the national surveys (Park et al., 2015).
Although some disability and rehabilitation studies have examined the health concerns and healthcare service utilization of people with visual impairments, there is a limited number of studies addressing the mechanisms of health behaviors of this marginalized population. Most studies focused on the health behaviors (i.e., smoking, medication adherence, physical activity, and vaccination) of older adults with age-related vision loss (Jones et al., 2009; O’Conor et al., 2018; Tatsuta et al., 2022). However, in public health, understanding health behaviors and their mechanisms in younger populations should be prioritized since health-related professionals and health policymakers can get an insight to support the development of health education programs and to reform healthcare systems to identify illnesses in early stages and to prevent chronic illnesses (Fulkerson et al., 2004).
To fill the gap in health behavior research on people with visual impairments, this study explored the constructs and patterns of health behaviors of young adults who are blind living in South Korea. In South Korea, which has a population of 51 million, about 252,632 individuals have visual impairments and 38,380 people are diagnosed with severe vision loss (Kim & Hwang, 2019). In this study, we specified the scope of people with visual impairments as persons who cannot see even with low-vision assistive devices (e.g., magnifying spectacles, hand-held magnifiers, correctly refracted glasses) (Vashist et al., 2017), and focused on employed young adults aged between 20 and 30 years. Finally, the purpose of this multiple case study was to explore the constructs and patterns of health behaviors of young adults who are blind in community settings.
The following research questions guided this study:
What are the constructs of health behaviors (i.e., perceived health risk, experiential attitude, health belief, facilitator, or barrier) of young adults who are blind? What are the patterns of the health behaviors of young adults who are blind?
Method
Multiple Case Studies Design
The present study employed a multiple case studies design (Figure 1). Case study designs have been commonly selected by researchers to collect rich and vivid descriptions of the phenomena of interest from the participants (Zach, 2006). Delineating and elucidating the phenomenon induces the researchers to achieve a deep understanding of a relatively small number of individuals, events, or situations (Patton, 1990). Unlike most case study designs focusing on a single case, the multiple case studies design employs a replication strategy to identify consistent patterns of behavior and to uncover new and/or divergent themes (Eisenhardt, 1989). In the multiple case studies design, replication is carried out in two stages: (a) a literal replication stage searching for the shared patterns and (b) a theoretical replication stage confirming the patterns identified in the previous cases (Yin, 1994).
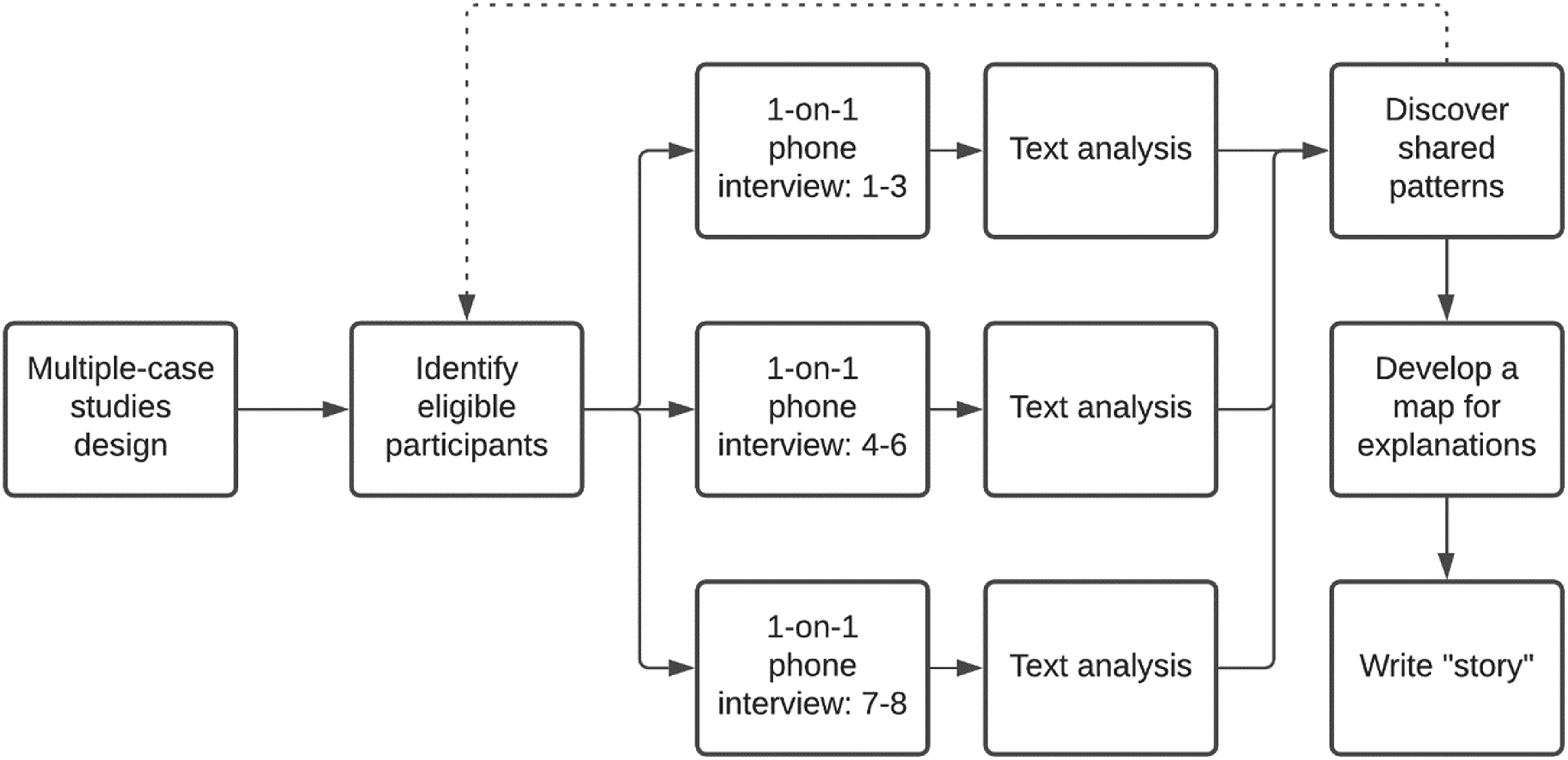
The Multiple Case Studies Design.
Ethical Considerations
The IRB approval (No. 2021-0361-001) of this study was obtained from the Institutional Review Board of Yonsei University Health System in Severance Hospital. All participants were provided with an electronic version of informed consent prior to enrollment in the study. The informed consent and research overview were sent to the participant's primary email address. Each participant was informed that they could withdraw from the research at any time, and the collected data would be secured by the research team to protect privacy.
Participant Recruitment
The sample size of this research was determined by adopting Yin’s (1994) recommendations for the replication strategy: 6–10 cases are required to provide compelling support for the initial propositions. Moreover, the final number of cases was finalized after confirming that there were no significant new findings from the data collection. For this study, access to the research participant pool was gained through personal contacts and recruitment postings on websites for people with visual impairments. The research team contacted the individuals who expressed an initial willingness to participate in the study via telephone calls, although some of them withdrew their willingness due to scheduling constraints. To explore participants’ health-related experiences in depth, the homogeneous sampling strategy was employed to the sample design. The homogeneous group was selected by following the selection criteria: (a) those with full vision loss or light perception only; (b) aged between 19 and 40 years; (c) those who have a job and are engaged in economic activities; (d) people residing in South Korea; and (e) those who can communicate in Korean without mental illness, cognitive impairment, or developmental disability.
Data Collection
For the study, a “case” was defined as a single, in-depth one-on-one phone interview with a research participant. The contacts between the research team and participants were conducted by email, telephone call, and mobile text messages. All of the data were collected from eight participants over a 2-month period using a pre-tested interview protocol. The questions included in the interview protocol were developed based on previous qualitative findings (Bilyk et al., 2009; Johnston et al., 2015). The interview protocol was pilot-tested on a young adult who is blind and a sighted counterpart independent of the study and then revised. Each question was matched to one or more of the research questions. An interview per case was conducted for 50–60 min. All interviews were conducted by one researcher and recorded with the permission of the participants. The participants were contacted until data saturation when the research team failed to find new information during the interview (Guest et al., 2006). The recorded interviews were automatically transcribed using an AI-based speech recognition service (Naver Corporation, n.d.), and the research team anonymized the transcribed interview transcripts. To disseminate findings from the study, the finalized codes, themes, and quotes were translated into English by a professional translation service.
Data Analysis
Data analysis was concurrent with the data collection to determine the point of data saturation. Among the various types of qualitative data analysis methods, thematic analysis combining inductive and deductive coding was selected (Braun & Clarke, 2006). To obtain the unique and distinctive themes from the interview transcripts, two researchers simultaneously created and evaluated the themes.
Literal Replication Stage
In the initial stage, the interviewer's notes made during the interview were collected and summarized. After that, each interview script was reviewed and analyzed independently by two researchers. During the initial open coding, each researcher initially coded three interview transcripts, then, applied the identified codes to the next three interview transcripts. Next, all identified codes from a total of six interview transcripts were listed. Next, each researcher independently coded all interview transcripts based on the amalgamated codes. Finally, the researcher compared each interview to the previous ones to confirm evidence and discover themes from the transcripts. When a new theme or themes emerged in later interviews, the earlier interviews were reanalyzed. By repeatedly confirming the evidence between earlier interviews and later ones, the internal validity of the data interpretation was strengthened.
Theoretical Replication Stage
To suggest plausible explanations of the identified patterns of participants’ health behaviors, the conceptual map was illustrated. At the same time, additional interview questions were reflected in the interview protocol to confirm the evidence. During the theoretical replication stage, any new themes conflicting with the predictable patterns were not discovered. To minimize bias in qualitative data analysis, all research team members performed ongoing checks in the text analysis process and conducted group analysis for member checks with each case of the study.
Results
Participant Characteristics
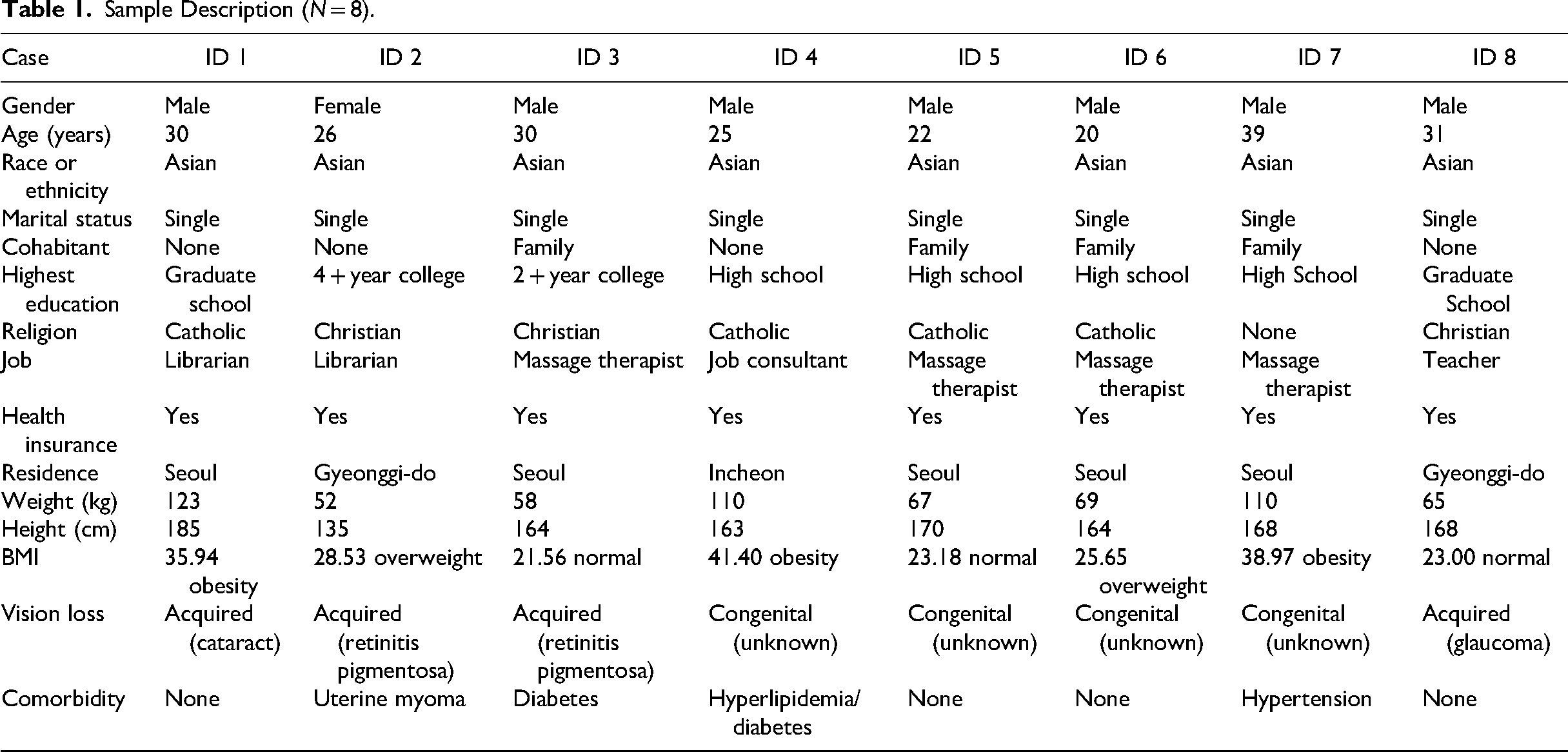
With the confirmation of data saturation at eight participants, the research team discontinued the data collection. Finally, seven males and one female completed the phone interviews, and the mean age was 27.43 years, ranging from 20 to 39 years. All participants were single Asians, and four of them lived with their families. Four participants were highly educated, and the others’ highest education was high school graduation, which meets the Korean required mandatory education level. However, all blind participants finished their basic mandatory education at a special education school for people with visual impairments. When they entered the special education school, they learned braille and were provided orientation and mobility training. In addition, when they were educated in the use of computers, they undertook a self-directed study to master the use of screen-reader software programs to read the text on a computer screen or mobile telephone. In relation to their physical appearance, five out of eight were obese or overweight. The individual characteristics are summarized in Table 1.
Sample Description (N = 8).
The Discovered Constructs of Health Behaviors
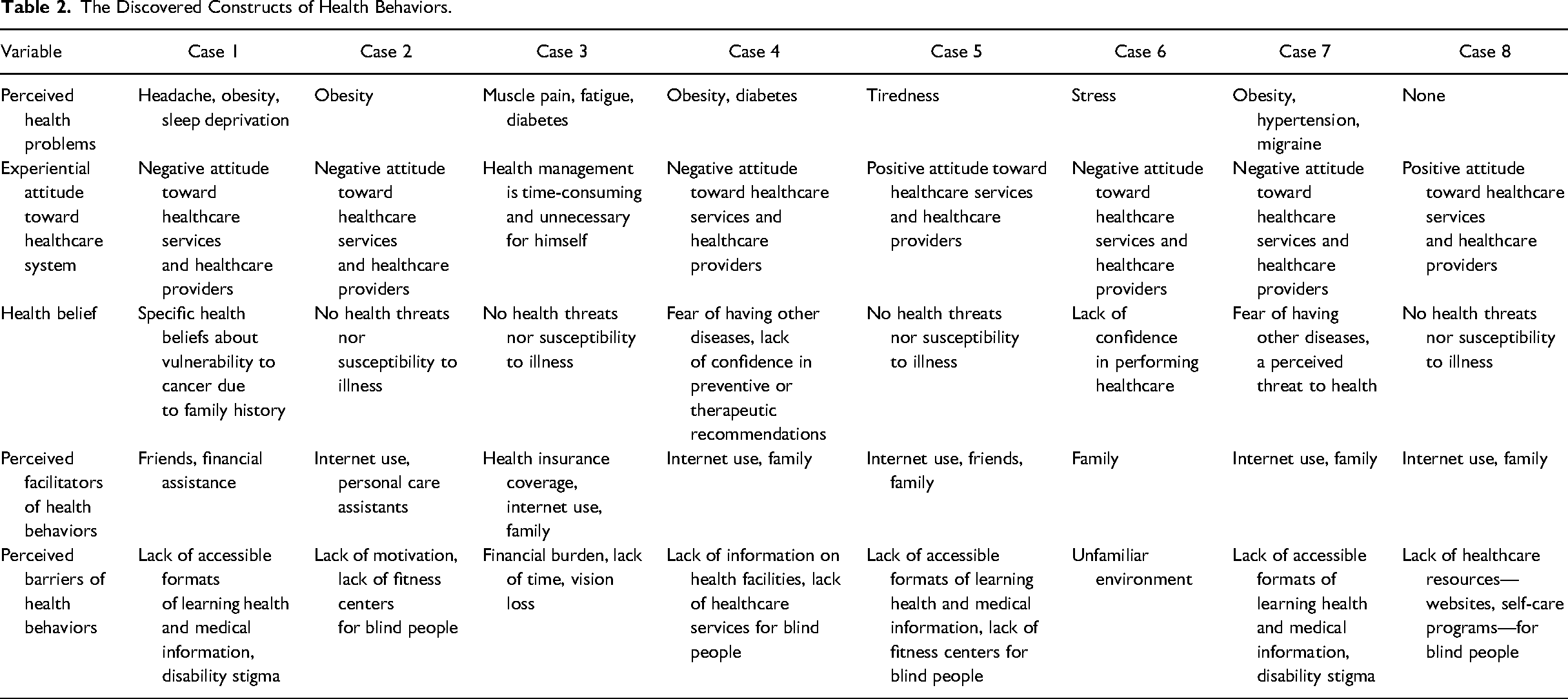
The hidden constructs—perceived health risk, experiential attitude toward health care system, health belief, facilitator, barrier—of health behaviors of participants are summarized in Table 2.
The Discovered Constructs of Health Behaviors.
The Patterns of Health Behaviors
During the participant interviews and subsequent text analysis of the interview transcripts, including the categorizing of dominant topics, revisiting the participants’’ narratives, and creating maps for conducting the data analysis, eight major themes emerged in relation to the original research questions: (1) leading a sedentary lifestyle with physical inactivity, (2) eating irregularly and not cooking, (3) avoiding uncertainty and illness, (4) facing disability stigma in health care services, (5) seeking online information related to medical care, (6) sharing health-related information within the blind community, (7) receiving unreadable formats of health-related information, and (8) aiming for independence and autonomy in self-care. The identified themes were explored in depth during the theoretical replication stage, and the discovered patterns of health behaviors and evidence are described as follows.
Pattern One: Leading a Sedentary Lifestyle With Physical Inactivity
In discussing sedentary lifestyles, the participants could not specify the difference between physical inactivity and sedentary behavior; they regarded the two concepts as having the same meaning and the main contributing factors as work-related factors. For example, several participants expressed their wish to exercise after work, but have to remain home due to the limited opening hours of gyms for blind people in their residential areas. Their working hours and the lack of support from their workplace and society conflict with their desire for physical activity. Some participants mentioned motivation as another main reason for physical inactivity: There is one fitness facility operating for blind people in my residence. It opens at 9 am and closes at 5 pm on weekdays. But I must work from 8:30 am to 5 pm. If we have exercise facilities at work, I think I can go for a quick workout during lunch or after work. (Case 1) I think doing regular exercise will decrease the risk of cardiovascular diseases, diabetes, and other types of chronic illnesses. I also think that my stress and depression can be prevented if I do some exercises. When I am continuously sitting, I frequently experience headache and dizziness. (Case 3)
Pattern Two: Eating Irregularly and Not Cooking
Most participants said they disliked cooking and did not engage in grocery shopping or making healthy food choices. In addition, most individuals were not provided any educational opportunities to learn how to do grocery shopping or prepare meals. They tended to eat meals prepared by family members or personal care assistants and displayed irregular eating patterns with unusual mealtimes; these were frequent observations for the participants involved in shift work as massage therapists. Several participants explained that they are not able to enjoy cooking due to numerous obstacles, such as blindness, safety considerations, laziness, and limited time: For me, it would take three hours for preparing a meal. It's time-consuming.… (Case 6) Typically, I start my work at 9 pm and it is 5 am when I return from work. I take some coffees and snacks during my working hours. Instead, I skip my breakfast. (Case 7)
Pattern Three: Avoiding Uncertainty and Illness
The avoidance of uncertainty and illness was commonly observed across the interviews. When asked the reason for not receiving yearly health screening tests, the participants mainly stated that they do not wish to know about their hidden diagnoses and exacerbations of their eye health or visual function. Some participants answered quickly and focused on surface-level concerns, believing that the topic was not very important. One participant felt uncomfortable when the interviewer asked about his eye health history: I mean I’m not going to do any health screening tests by myself. If my workplace requires the test results, then I think I will do. But I would not pay my money for it. I don’t want to know about my bad situations. I don’t know how to manage whole things again. You know … I have already spent my teenage [years experiencing] multiple eye surgeries and hospital admissions and rehabilitation. I don’t even care to think about other health problems. (Case 1) Well … I don’t know, I think I am not ready to take anything about my health. Because I have already lost my vision since I was 8 [years old]. Being blind is something I’ve walked through since I was 8. So if other medical problems were newly discovered, it would depress me the most I guess. Yeah … it would not be a life-changing thing for blind persons, but I am not ready to take it in. (Case 4)
Pattern Four: Facing Disability Stigma in Health Care Services
The majority of the participants were aware of the stigma associated with their blindness and mentioned that disability stigma is a significant factor discouraging individuals with visual impairments from using medical services when needed. In detailing their previous encounters with disability stigma, the participants’’ commonly shared experience was that health care providers, physicians, and nurses consider that blind people are entirely reliant on sighted people for assistance and that they also have low intellectual ability. Due to these stereotypes, physicians and nurses engaged in patronizing communication and offered inappropriate care to people with visual impairments. When the participants visit hospitals, they have to acknowledge their disability and experience amplified feelings of being different from sighted people: Doctors and nurses tend to see blind people as mentally handicapped and annoying patients. They treat me like a child. I realize the fact that I need so much help from others and I am different from other people. (Case 5)
Pattern Five: Seeking Online Information Related to Medical Care
The participants gain most of the information pertaining to medical care and medical decision-making from online searches, many of which are conducted to investigate their symptoms and treatments. Even when attending medical appointments with physicians, they tend to research their symptoms, medications, and other treatment options in advance. Naver (https://www.naver.com/) is the most frequently used Korean search engine, but some participants prefer YouTube (https://www.youtube.com/). Most participants trusted online information and frequently used the Internet to navigate medical knowledge and health care services. This behavior of seeking health information extends from their own health to that of their family members with health problems: My mother is suffering from her rheumatoid arthritis. So I went to Naver and researched what the symptoms are, how to manage it, and what's the best way to relieve pain. I also found the contact information for her medical consultation. (Case 7)
Pattern Six: Sharing Health-Related Information Within the Blind Community
Most participants are members of the Korea Blind Union and the Siloam Center for the Blind, which are the largest blind communities in South Korea. Using the websites of these two institutes, the participants search for and retrieve health-related information, including medical care resources. Since the size of the Korean blind community is small, most people with visual impairments in similar age groups tend to know each other. The participants sometimes join exercise programs designed for people with visual impairments and share health-management strategies, hospital and ophthalmological information, and nutrition supplements. They feel strong social connectedness with other people who are blind and are eager to have many opportunities for social activities. Some participants mentioned that the interactions between persons with visual impairments regarding medical issues are useful and reduce their feelings of anxiety and loneliness. Some blind friends introduced me [to] my current ophthalmologist. My doctor knows all of my blind friends. (Case 3)
Pattern Seven: Receiving Health-Related Information in Inaccessible Formats
Regarding health-related information, all the participants expressed negative attitudes toward its format, indicating that they have never received any accessible medical information about their health conditions, test results, medications, and self-management. Most medical information from primary physicians is delivered to their main family caregivers. When the participants have undergone surgeries, health care providers neither read aloud the contents of informed consent forms to them nor provided them with audio-recorded files containing this information. Some participants indicated they needed to ask for help from sighted family members or friends to learn about written medical documents: Most physicians don’t really know how to deal with blind patients. They routinely provide printed information about medications and educational materials. Of course, those are not [in] braille. Most materials from hospitals are rarely provided in accessible formats. (Case 3) Sometimes, pharmacists tell me to read and follow the instructions on the pill bottle. For example, whether to take it with food or not. It would be really helpful if they read aloud and explain those instructions too. (Case 6)
Pattern Eight: Aiming for Independence and Autonomy in Self-Care
Multiple participants stressed that they wish to have independence in everyday activities and tasks, using the terms “independence” and “autonomy” frequently across the interviews. According to them, the dominant stereotype about people with visual impairments in society is that they cannot completely perform daily life activities; that is, they cannot realize self-reliance and self-care. However, most participants mentioned that they can care for themselves if environmental barriers are sufficiently resolved: It would help me if others guided and explained me about the physical environment. . . . If someone teaches me yoga, I will really enjoy that. (Case 2)
The availability of fitness facilities and the residency of personal trainers for blind people would support me to do exercise on a daily basis. (Case 7)
Discussion
Adulthood, comprising the age range from 25 to 40 years, involves the years of peak professional career development and financial achievement when most individuals establish their self-identity, autonomy, family integration, and social network (Strnadová & Cumming, 2016). This study focused on young individuals who are blind at the developmental and early midlife stages of adulthood to understand their health behaviors and discover the social and environmental factors influencing their unique health behavioral patterns. In line with theories related to health behavior, the individual beliefs and attitudes, subjective norms, personal agency, and environmental contexts mentioned by the young adults who are blind in this study were interrelated.
Demographically, all the study participants were single, and half of them lived with their parents. Within the family–centric Korean culture, parents frequently extend their caregiving role to children with disabilities, maintaining this support even following the children's marriage (Lee & Oh, 2013). Primary caregivers are responsible for preparing most meals for the participants, and the findings indicate that young adults who are blind do not have enough time for engaging in grocery shopping and learning about healthy food choices and preparation. Previous research has also mentioned the identified obstacles (Bilyk et al., 2009); however, the issue of limited time seems to be considered more significant for workers who are blind. Moreover, most participants seldom understood the significance of healthy food choices and regular mealtimes. To prevent nutrition-related chronic illnesses in middle adulthood, providing healthy diet programs and hands-on cooking classes in the workplace for employees with disabilities can be considered (Celeste-Williams et al., 2010).
For people with disabilities, fitness facilities are one of the representative avenues providing equal opportunity and accessibility in public accommodation (Rimmer et al., 2017). Nevertheless, the number of accessible fitness facilities providing services to people with disabilities has plateaued (Johnston et al., 2015). Across all interviews, the participants mentioned the lack of fitness facilities, including personalized exercise prescriptions for people with visual impairments, as a key barrier. Even when they are willing to carry out daily regular exercise, the typical fitness facilities are inaccessible without the assistance of sighted people. In addition, without a certain degree of guidance from professional trainers, customized exercise programs and equipment selections cannot be realized, which can result in low satisfaction and performance. Carpenter (2010) and Harrison et al. (1992) stated that perceived barriers are the single most powerful factor leading to problematic health behaviors. Therefore, examining the independent effects of the physical environment of accommodation facilities (e.g., pictorial and braille instructions, tactile indicators, universally designed equipment, and guidewire installments) on the physical activity and health outcomes of individuals with visual impairments is needed. A successful exercise intervention can contribute to reducing the high prevalence of cardiovascular diseases among people with visual impairments (Kim et al., 2021).
People with visual impairments, including blindness, are particularly marginalized in society, and they frequently encounter social inequalities when using healthcare services (Shandra, 2018). Previous literature has called into question the efficacy of hospitals’ discretionary policies and disability education in health curricula considering health care disparities and disability stigmatization (Havercamp et al., 2021). Persistent disability stigmatization contributes to individuals with visual impairments avoiding the use of health care services; dissatisfaction with such services lowers the rate of preventive health screenings and timely health consultations. Notably, feelings of being denied by healthcare systems frequently emerged from not feeling acknowledged by health professionals. Multiple participants reported feeling frustrated when they were not provided accessible formats of medical documents and were not properly informed in clinical settings. To facilitate the use of healthcare services among individuals with visual impairments, we need to sufficiently provide continuing educational programs for healthcare professionals to reduce healthcare disparities and disability-related stigmatization in clinical practice.
Another crucial factor leading to discomfort in health care services from the perspective of young adults who are blind is the violation of their privacy as patients in healthcare settings. When the participants attend medical consultations with family members, the physician–patient relationship is formed with their sighted caregivers, not the person who is blind. The participants mentioned that healthcare professionals initiate and terminate conversations with the accompanying sighted caregivers in most cases. Considering the climate of medical ethics, healthcare professionals should consider protecting the privacy and confidentiality of people with visual impairments (Latibjonovna, 2021).
Self-regulatory skills and strategies should first be developed to initiate or maintain a person's health behaviors (Schwarzer et al., 2011). Informational social support, which can include removing barriers or promoting resources to initiate or maintain health behaviors, is needed (Schwarzer et al., 2011). Many young adults who are blind in this study had the ability to navigate the Internet using search engines on their personal computers or smartphones. The education and information science spheres have explored the information-seeking behavior of students with visual impairments (Li & Li, 2014; Sahib et al., 2012); however, scientific literature on such behavior related to health information is still lacking. Unlike other categories of online material, medical or health-related information should be thoroughly reviewed and evaluated by experts (Swire-Thompson & David, 2019). To prevent the sharing of health misinformation between people with visual impairments, in addition to restructuring the online information ecosystem, assessing and evaluating digital health literacy skills are needed (Estacio, Whittle & Protheroe, 2019).
Limitations
Firstly, the results are not applicable to other races, ethnicities, countries, and individuals with chronic health conditions other than those who participated in this study. The findings of this study should be interpreted with consideration of the social services that are provided to citizens in South Korea and the country's inherent cultural background; the different extent and scope of disability-related social services and health insurance coverage may affect the health behaviors of people with disabilities. Secondly, minimal sources were available for developing the interview protocol due to a lack of previous literature on the health behaviors of people with visual impairments. Moreover, the interview protocol of the study was not validated by external experts. Thirdly, most narratives in the interview transcripts were collected from male participants, which may not reflect the effect of gender differences on health-related experiences. Lastly, the qualitative research results are not generalizable; however, this study sheds light on disparities in health care from the perspectives of young adults who are blind.
Conclusion
In summary, the present research investigated the problematic health behaviors of young adults who are blind and the critical factors influencing their behavioral choices. First of all, health professionals need to regard people with visual impairments as individuals who value independence, autonomy, human dignity, self-determination, and privacy in the utilization of health care services. To motivate young adults who are blind to carry out physical activity, more accessible fitness facilities and personalized exercise programs should be provided in their workplaces and communities. Finally, to prevent the spread of online health misinformation, people with visual impairments should be alerted about the risks of unverified online health information.
Footnotes
Authors’ Contribution
Soyoung Choi contributed to conceptualization, research design, data collection, and data analysis. Arum Lim contributed to data collection and data analysis. Hyangkyu Lee contributed to research design and data analysis. All authors contributed to manuscript writing and submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.