
Abstract
Keywords
Sleep is a fundamental biological process in children that is critical to their health and well-being, and it both influences and is influenced by physical functioning (Dahl, 1996; Tubbs et al., 2019). One of the key processes that support sleep is the circadian rhythm, a system governed by the hypothalamus that is dependent on visual input (Borbély et al., 2016). Sleep is thus dependent on vision, and visual impairment (ie, blindness or low vision) can serve to disrupt sleep-related processes (Emens et al., 2013; Hou et al., 2023). Building on this connection, recent research has documented the robust links between sleep and physical activity (Antczak et al., 2020). Physical activity can promote better sleep (Antczak et al., 2020; Lang et al., 2016), but it is also affected when sleep is disrupted (Yoong et al., 2016). Given the essential nature of sleep to functioning, it is important that research documents the diverse links among these disparate processes. In the case of the current scoping review, an exploratory project that systematically maps the literature available on a topic (Peters et al., 2020), we aimed to assess the state of the literature that has examined sleep, visual impairment, and physical activity specifically in youths (i.e., ages 18 years and under).
There are many diverse influences on sleep, but the effect of light is vital to sleep through its effect on circadian entrainment. Alterations in light signal to an area of the hypothalamus called the suprachiasmatic nucleus, which is responsible for the pineal gland's production of melatonin, a hormone that helps to regulate sleep–wake states (Lockley et al., 2007). Obstacles to the sensation of light (e.g., visual impairment) can thus disrupt this neurophysiological process and affect the sleep–wake cycle. Depending on the extent of an individual's visual impairment, those with the lowest capacities to sense the presence of light have the highest prevalence of circadian rhythm disorders (Lockley et al., 2007). Specifically, research suggests that the majority of totally blind individuals (i.e., visually impaired individuals without light perception) have difficulty maintaining sleep, and approximately 30% of visually impaired individuals (with or without light perception) report irregular sleep–wake patterns (Tamura et al., 2016) as compared to approximately 8% in the general population (Paine et al., 2014). Although light is central to circadian rhythm entrainment, there are also non-photic cues that support the sleep–wake cycle. Specifically, time cues (also called zeitgebers) include exercise, scheduled activities (e.g., work, school), and meals (Mistlberger & Skene, 2005). Taken together, the confluence of light exposure and time cues serve to entrain the circadian rhythm to run on an approximately 24-hr cycle and support a regular sleep–wake cycle. This process can be disrupted for individuals with visual impairments, and the consequences of sleep problems include adverse mental and physical health outcomes (Augestad, 2017; Brian et al., 2019).
Generally speaking, physical activity is linked to the sleep of youths, although many complexities remain in explaining this relationship. First, physical activity is often encouraged for individuals with sleep problems because of its positive effects on sleep (Lang et al., 2016). However, this effect is more strongly associated with adolescents and early adults than it is in children, and research suggests that the effect is most often found in studies of vigorous forms of exercise's effect on sleep (Antczak et al., 2020; Lang et al., 2016). Despite a relative paucity of research on children in this area, it is possible that the different physiological processes present in older youths (e.g., pubertal change, changes in circadian rhythm) play a role in the effect of physical activity on sleep (Kalak et al., 2012). Second, there is little evidence to suggest that a bidirectional relationship exists between children's physical activity and sleep (Antczak et al., 2020; Vincent et al., 2017). Although Niederer et al. (2009) found that a multidimensional intervention focusing on physical activity, nutrition, media use, and sleep resulted in increased aerobic fitness, it was unclear to what extent the focus on sleep improvement might have led to this result (Niederer et al., 2009). Although multiple studies have identified links between sleep and visual impairment in children and adolescents (Lazreg et al., 2011; Leger et al., 1999; Okawa et al., 1987), more extensive research is needed to discern the interrelations between sleep and physical activity in youths, especially given the known differences between its effects in children and adolescents.
Children with visual impairments face numerous barriers and challenges in pursuing physical activity (Augestad & Jiang, 2015). Not only are there lower levels of participation in physical activity for children with visual impairments, but these children also tend to exhibit poorer physical fitness and higher rates of obesity than children without visual impairments (Haegele & Porretta, 2015; Piva da Cunha Furtado et al., 2015). Despite these negative health outcomes, Lieberman et al. (2014, 2018) have found that engaging in physical activity may positively affect both the physical and mental health of children with visual impairments (Lieberman et al., 2014; Lieberman & MacVicar, 2019). However, preventing children with visual impairments from engaging in physical activity, for example, due to parental overprotection, lack of time, or fear of injury (Linsenbigler et al., 2018) may contribute to their lack of physical fitness and higher rates of obesity (Physical Activity Guidelines Advisory Committee, 2018). Although research has documented some of the challenges children with visual impairments tend to experience with sleep (Emens et al., 2013), there is a paucity of research linking physical activity and sleep in children with visual impairments. Accordingly, there is a critical need to address this gap in understanding if we are to develop more effective methods for addressing sleep and physical activity in children with visual impairments. Therefore, the purpose of this scoping review is to examine the current literature related to the relationship between sleep and physical activity for youths with visual impairments.
Methods
Study Objectives
The objective of the study presented here was to summarize the available evidence regarding the relationship between physical activity and sleep of children and adolescents who are blind or have low vision.
Guiding Framework
A scoping review of the literature was selected as the most appropriate method of assessing the literature as it makes it possible to examine the nature and scope of evidence available and identify any gaps evident in the literature (Peters et al., 2020). This study followed the five-stage approach for scoping reviews set out by Arksey and O’Malley (2005), namely (a) identifying the research question, (b) identifying relevant studies or articles, (c) study or article selection, (d) charting the data, and (e) collating, summarizing, and reporting the results (Arksey & O’Malley, 2005).
Stage 1: Identifying the Research Question
The review questions for this scoping review were guided by the PICO (population, intervention, control, and outcomes) analysis (Santos et al., 2007; see Table 1).
PICO (Population, Intervention, Context, and Outcome) Design and Description.
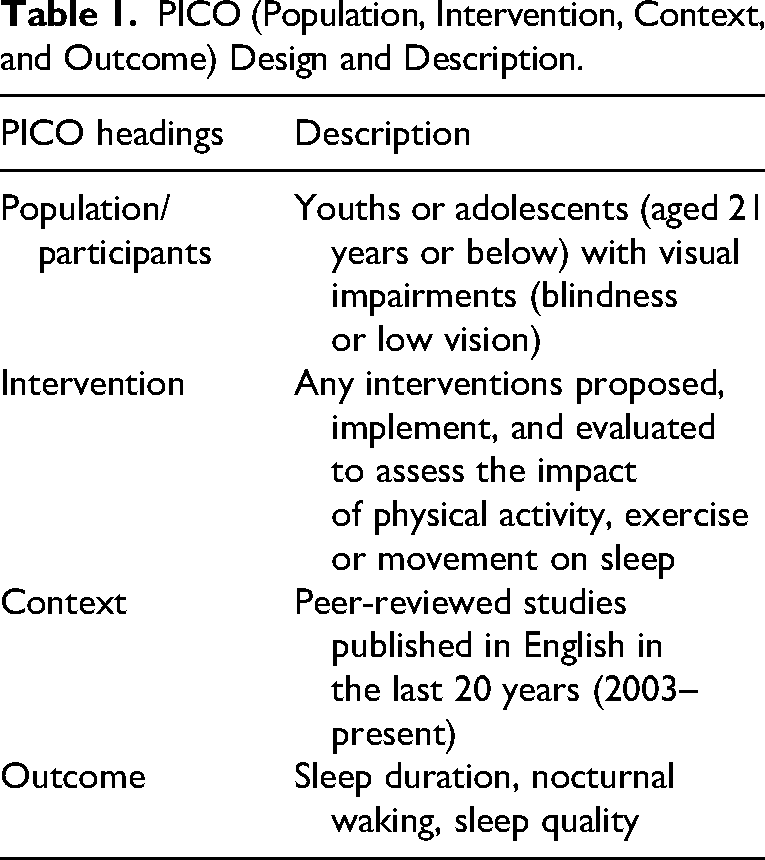
Based on the effect of pubertal changes on adolescents’ sleep, the two specific research questions identified are as follows: What is the impact of physical activity on the sleep of (a) children and (b) adolescents who are visually impaired (ie, blind or have low vision)?
Stage 2: Identifying Relevant Studies or Articles
The search strategy was developed collaboratively by the research team. A search of published peer-reviewed articles available in PubMed, SCOPUS, Web of Science, Sports Discus, and Embase was conducted using the following keywords which were deemed relevant to the project: (“youth” OR “adolescence” OR “child”) AND (“blind” OR “low vision” OR “visual impairment”) AND (“physical activity” OR “movement” OR “fitness”).
Following completion of the search, citations from each database were uploaded to Covidence, a web-based program that identifies and removes duplicate entries (Veritas Health Innovation, 2024). The title and abstract of each citation were screened by two reviewers. Reference lists were additionally searched for possible additional studies. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrating the data charting process of this scoping review is presented in Figure 1 (Tricco et al., 2018).
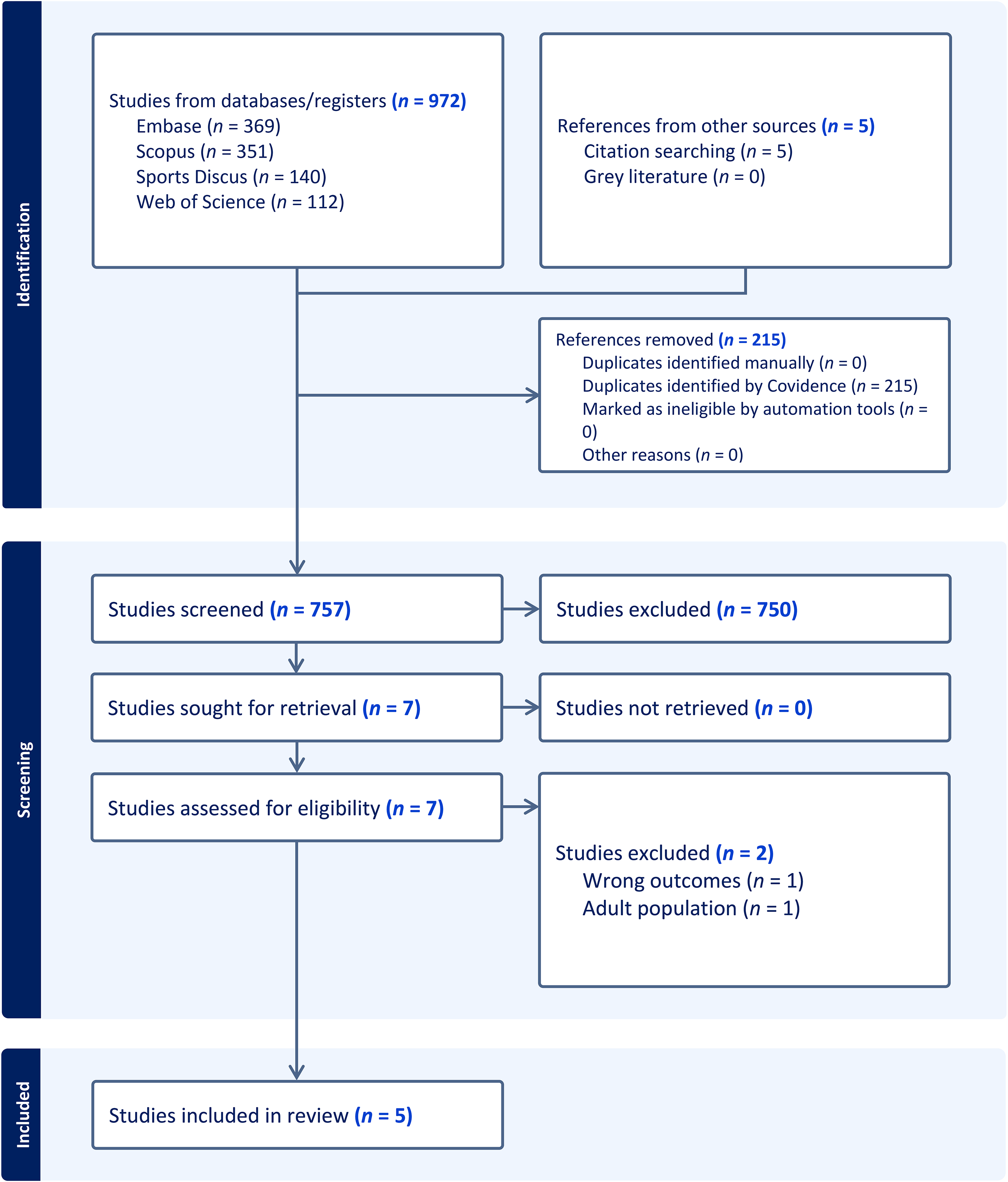
PRISMA Diagram. Note. (alt text) 972 references imported for screening as 972 studies; 0 duplicates identified manually; 15 duplicates identified by Covidence. 757 studies screened against title and abstract; 750 studies excluded. 7 studies assessed for full-text eligibility; 2 studies excluded; −1 adult population; −1 wrong outcomes; 0 studies ongoing; 0 studies awaiting classification. 5 studies included.
Stage 3: Study or Article Selection
The screening of titles, abstracts, and full text of citations was conducted by two reviewers. Disagreements were resolved through discussion until a decision on the inclusion or exclusion status was reached. The population of interest for this study was defined as youths (18 years of age or younger) who are blind or have low vision. Studies were included if they met the following inclusion criteria;
published between 2003 and October 2023, published in the English language, and reported issues relating to the effect of physical activity on sleep in children and adolescents who are blind or have low vision.
Stage 4: Charting the Data
Five studies were included in the final analysis from the 972 unique studies screened. Characteristics from each paper including study methods, design, participants, measures, and findings were recorded. Table 2 presents the key data extracted including author identification, year of publication, study design, and the aims and objectives of each study.
Summary of Studies Included in the Scoping Review.
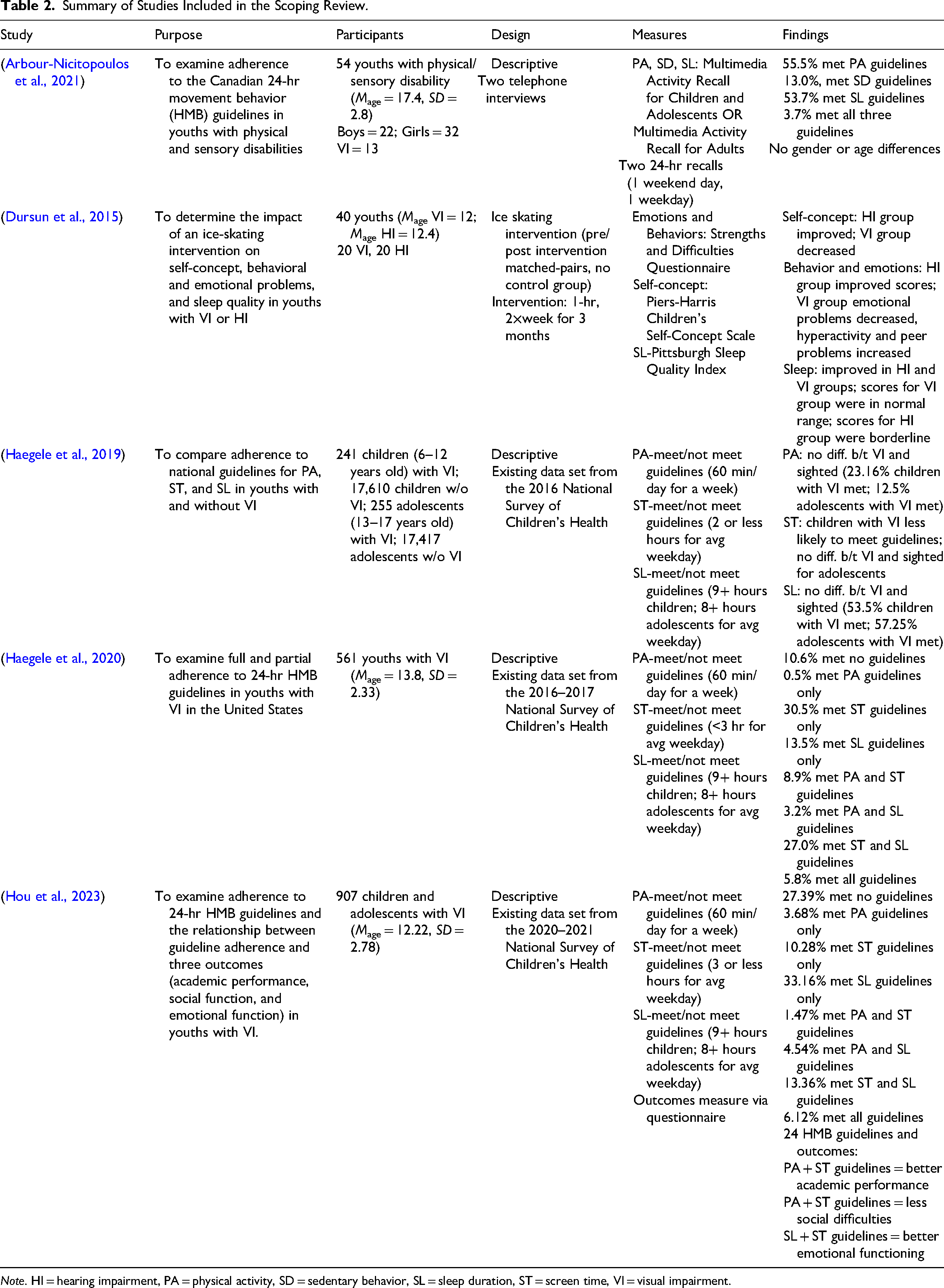
Note. HI = hearing impairment, PA = physical activity, SD = sedentary behavior, SL = sleep duration, ST = screen time, VI = visual impairment.
Findings
In this scoping review, five studies were identified that examined physical activity, sleep, and screen time in youths with visual impairments. A total of 972 articles were identified in the search, and an additional five were identified through citation search. After removing 215 duplicates, the title and abstract of 757 studies were screened. Following the exclusion of 750 studies, the full text of seven articles was reviewed, and two were excluded (see Figure 1). After reviewing these manuscripts, the reviewers determined there were two main findings related to these studies: (a) meeting the guidelines and (b) intervention effects.
Meeting the Guidelines
Four of the five studies examined how well youths with visual impairments were meeting established guidelines for physical activity, sleep, and screen time. The studies differed slightly on the source for their guidelines. Haegele et al. (2019) used guidelines from the U.S. Department of Health and Human Services for physical activity, the American Academy of Pediatrics for screen time, and the American Academy of Sleep Medicine for sleep (Haegele et al., 2019). Two studies used the 24-Hour Movement Behavior guidelines (Haegele et al., 2020; Hou et al., 2023), and one study used the Canadian 24-Hour Movement Guidelines (Arbour-Nicitopoulos et al., 2021)
Two studies used the 2016–2017 National Survey of Children's Health (Haegele et al., 2019, 2020). In the first study, Haegele et al. (2019) compared children (aged 6–12 years old) and adolescents (aged 13–17 years old) with visual impairments to sighted peers in the United States on how well they met the guidelines. The authors found no statistically significant differences between groups for meeting the physical activity and sleep guidelines, though potentially clinically meaningful differences (5.35–5.98%) were identified (Haegele et al., 2019). For physical activity, 23.16% of children and 12.5% of adolescents with visual impairments met the guidelines while 28.51% of sighted children and 18.34% of sighted adolescents met the guidelines. For sleep, 53.5% of children and 57.25% of adolescents with visual impairments met the guidelines, while 64.01% of sighted children and 70.28% of sighted adolescents met the guidelines. The authors did find that children with visual impairments (69.92%) were less likely to meet the guidelines for screen time than their sighted peers (79.59%); however, there was no difference between the adolescents with visual impairments (70.7%) and sighted peers (71.71%).
The second study that used the 2016–2017 National Survey of Children's Health (Haegele et al., 2020) examined the proportion of 561 youths with visual impairments (Mage = 13.8 years, SD = 2.33 years) in the United States who met all or some of the physical activity, sleep, and screen time guidelines. The results revealed that only 5.8% of participants met all three guidelines, while 10.6% met none of the guidelines. For participants meeting partial guidelines, 3.2% met both sleep and physical activity guidelines, 8.9% met both physical activity and screen time guidelines, 27% met both screen time and sleep guidelines, 0.5% only met physical activity guidelines, 13.5% only met sleep guidelines, and 30.5% only met screen time guidelines. Hou et al. (2023) conducted a similar study using the 2020–2021 National Survey of Children's Health (Hou et al., 2023). They found that out of the 907 youths with visual impairments (Mage = 12.22 years, SD = 2.78 years) included in the survey, 6.12% met all three guidelines, while 27.39% met none of the guidelines. For participants meeting partial guidelines, 4.54% met both sleep and physical activity guidelines, 1.47% met both physical activity and screen time guidelines, 13.36% met both screen time and sleep guidelines, 3.68% only met physical activity guidelines, 33.16% only met sleep guidelines, and 10.28% only met screen time guidelines.
The authors also looked at the relationship between guideline adherence and three outcomes: (a) academic performance, (b) social function, and (c) emotional function. They found that adherence to physical activity and screen time guidelines was associated with better academic performance and less social difficulties while adherence to sleep and screen time guidelines was associated with better emotional functioning.
The data from preceding studies came exclusively from a national survey in the United States; however, one study did examine individuals outside of the United States. Arbour-Nicitopoulos et al. (2021) surveyed 54 Canadian youths (Mage = 17.4 years, SD = 2.8 years) with physical or sensory disabilities using the Multimedia Activity Recall to assess how well the participants met the Canadian 24-hr guidelines for children and youth (Arbour-Nicitopoulos et al., 2021). Of the 54 participants, 13 (24.07%) had visual impairments (Arbour-Nicitopoulos et al., 2021). The results indicated that 55.5% of participants met the physical activity guidelines, 53.7% met the sleep guidelines, 13.0% met the sedentary guidelines, and only 3.7% met all three guidelines.
Intervention Effects
One study examined the effect of a physical activity intervention on sleep in youths with sensory impairments in Turkey (Dursun et al., 2015). Forty youths (aged 8–16 years old) who were either visually impaired (VI group; n = 20) or deaf and hard of hearing (HI group; n = 20) participated in an ice-skating program for 1 hr two times each week for 3 months. Participants worked with the same trainer throughout the program and worked on skills such as balance, stopping, and speed control. Participants completed pre- and post-program measures to assess any changes in their sleep, self-concept, and behavior and emotions as a result of the intervention. The results revealed that both groups improved their sleep following the intervention, with the visually impaired group reaching the typical range. The visually impaired group also showed decreased emotional problems following the intervention; however, their self-concept decreased, and they had increased problems with hyperactivity and peers.
Discussion
The purpose of this scoping review was to examine the available literature regarding physical activity and sleep of children and adolescents who are blind or visually impaired. Visual impairment was defined by individual studies included in this scoping review. Two studies used the 2016–2017 National Survey of Children's Health (Haegele et al., 2019, 2020), in which participants with visual impairments were identified as those whose parents answered “yes” to the following question: “Does this child have any of the following: Blindness or problems with seeing, even when wearing glasses?” Hou et al. (2023) similarly used a single-item question obtained from parents and guardians (i.e., “Does your child have any kind of blindness or problems with seeing, even when wearing glasses?”) (Hou et al., 2023). One study recruited participants through a school for visually impaired students, whereby acceptance into the school required an ophthalmologic examination in a hospital (Dursun et al., 2015). The remaining study identified visual impairment via self-identification or parent report, though the phrasing of the question used was not included in that paper's methodology (Arbour-Nicitopoulos et al., 2021).
The screening criteria for this scoping review included articles on physical activity and sleep in youths aged 18 years or younger that have been published in English over the past 20 years. Five articles met the inclusion criteria and were used in the present study. The two main findings from this scoping review included (a) meeting the guidelines and (b) intervention effects.
Sleep and physical activity are lifestyle behaviors that are associated with health indices and quality of life (Carson et al., 2017). Four of the five research studies included in this scoping review examined the guidelines for physical activity and sleep in youths with visual impairments (Arbour-Nicitopoulos et al., 2021; Haegele et al., 2019, 2020; Hou et al., 2023). The guidelines were the same for each study, with the exception of screen time. To meet the physical activity guidelines, participants had to participate in at least 60 min of physical activity each day during the week. To meet the sleep guidelines, children had to get at least 9 hr of sleep on an average weekday, and adolescents had to get at least 8 hr of sleep on an average weekday. To meet the screen time guidelines, participants could use screens (e.g., television, video game, cell phone) for non-school purposes for 2 hr or less (Arbour-Nicitopoulos et al., 2021; Haegele et al., 2019) or 3 hr or less (Haegele et al., 2020; Hou et al., 2023) on an average weekday. It should be noted, however, that the screen time guidelines used within these studies are not specifically designed to apply to visually impaired youths, who likely make use of assistive technology for other purposes (e.g., to access printed materials). The Canadian-24 Hour Movement Guidelines, used by Arbour-Nicitopoulos et al. (2021), as well as Haegele et al. (2019), were developed for use in “apparently healthy children” (Arbour-Nicitopoulos et al., 2021; Haegele et al., 2019; Tremblay et al., 2016), while guidelines issued by the American Academy of Pediatrics selected by Haegele et al. (2020) were initially developed for use in “well child” visits to physicians (Haegele et al., 2020; Strasburger et al., 2013). Chosen papers that make use of these guidelines each acknowledge the need for further evidence to identify optimum guidelines for youths who are blind or have low vision.
Sleep guidelines included a minimum of 9 hr of sleep on an average weekday for youths and 8 hr of sleep per day on an average weekday for adolescents. Few youths with visual impairments (9.0%, according to Haegele et al., 2020; and 10.66%, according to Hou et al., 2023) met the sleep and physical activity guidelines. Perhaps, more concerning were the percentage of youths with visual impairments who did not meet any of the guidelines including sleep, physical activity, or screen time (10.6%, Haegele et al., 2020; 27.39%, Hou et al., 2023). The findings of Hou et al. (2023) indicated that perhaps this trend is worsening, with proportionally fewer of the 907 youths with visual impairments meeting guidelines in the 2020–2021 National Survey of Children's Health in comparison to the 561 youths with visual impairments surveyed in the 2016–2017 data (Hou et al., 2023). It should be noted, however, that the second data analysis conducted by Hou et al. (2023) was conducted during the global pandemic that began in 2020. Physical activity in youths with visual impairments was significantly reduced during the COVID-19 pandemic due to additional barriers including the closing of schools, recreation centers, and gyms, as well as restricted access to outdoor recreational facilities such as parks and playgrounds (Maniu et al., 2022; Richardson et al., 2023).
Reduced physical activity participation in youths with visual impairments in comparison to youths without visual impairments has been widely documented (Augestad, 2017; Haegele & Porretta, 2015). Many physical benefits can result from a physically active lifestyle, while low levels of physical activity and high levels of sedentary behaviors are associated with adverse health-related outcomes (Brunes et al., 2015) and health-related fitness (Brian et al., 2019), placing individuals with visual impairments at risk for obesity and morbidities associated with obesity (Augestad & Jiang, 2015; Lawrence & Kopelman, 2004; Lieberman et al., 2010).
Benefits of physical activity have also been linked to sleep. However, such benefits tend to differ developmentally, with strong associations between increased physical activity and sleep in adolescents and young adults and weak evidence supporting the benefits of physical activity and sleep in youths (Antczak et al., 2020; Lang et al., 2016). Currently, there is no research examining the relationship between physical activity and sleep in youths or adolescents with visual impairments. Additionally, only a few studies have examined physical activity and sleep, with four studies focusing on meeting the guidelines and one study conducting an intervention. The one intervention study conducted on the benefits of physical activity with ice skating across a period of 3 months revealed promising results, with improvements in sleep following the 3-month intervention (Dursun et al., 2015). It is important to note that there was no control group for this study; however, the findings provide some preliminary support for the influence of physical activity on sleep in youths with visual impairments.
Conclusion
Children and youths with visual impairments are not achieving minimal guidelines for sleep or physical activity. Sleep and physical activity have long-term consequences if the minimum guidelines are not met. Through increased physical activity, it is possible to improve the sleep of youths with visual impairments, as found in one intervention study where the mean age of visually impaired participants was 12 years. This scoping review reveals the dire need for more research on sleep and physical activity in youths with visual impairments. Research must be conducted to understand the association between physical activity and sleep. Additionally, controlled intervention research should be conducted to determine how to effectively improve sleep through physical activity in youths with visual impairments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication has emanated from research supported by Vision Sports Ireland (VSI) and Science Foundation Ireland (SFI) under grant no. SFI/12/RC/2289_P2 (Insight SFI Research Centre for Data Analytics), co-funded by the European Regional Development Fund.