
Abstract

Graded cardiopulmonary exercise tests are necessary in clinical and research settings to calculate exercise capacity, determine exercise tolerance, and inform exercise prescription (Lima et al., 2019). Although laboratory assessments using a treadmill or cycle ergometer to measure VO2max and ventilatory threshold are considered the gold standard, they require dedicated equipment, space, and trained personnel to administer, and are therefore expensive (Beltz et al., 2016). For graded physical capacity testing in the community, tests need to be accessible, inexpensive, portable, and easily administered. Walking tests are therefore desirable for measuring cardiopulmonary capacity in the community, the most common being either the six-minute walk test (Enright, 2003) or the incremental shuttle walk test (ISWT) (Singh et al., 2008). The former is a self-paced measure of endurance and, therefore, may not produce a maximal effort, whereas the ISWT is externally paced via audible cues, producing a maximal effort (Singh et al., 2008). This test is validated in adults (Parreira et al., 2014) as well as children and adolescents (de Cordoba Lanza et al., 2015). It is performed by walking shuttles of a 10-meter track in response to pre-recorded beeps. The participants begin walking, performing one shuttle (10 m) at 0.50 m/s per beep. Each minute, the speed of walking increases, up to 2.37 m/s. The test ends when the participant fails to reach the turnaround cone before the next beep, becomes too fatigued, or completes the entire test (Lima et al., 2019).
The ISWT is a reliable test for healthy adults without vision loss (Harrison et al., 2013) but alterations that accommodate people who are blind have not been described. It is clear, however, that a person who is blind cannot see the turnaround cones nor the direction of the track between those cones. This case study describes a modification to the ISWT for a person who is blind, in support of access to services, facilities, or amenities for people of all abilities, as required by The Australian Disability Discrimination Act 1992. The parent study that generated this brief report used ISWT to facilitate fatigue in healthy, community-dwelling adults aged 40–74 years.
The accepted National Eye Health Survey definition for blindness is the inability to read a vision chart at 6 m, which a person with normal vision can read at 10 times that distance (60 m) (6/60). The equivalent definition for vision impairment is between 12 (6/12) and 60 m (6/60) (Foreman et al., 2016). The prevalence of blindness globally is 0.6% (Steinmetz et al., 2021).
Many people with vision impairment use no mobility device, relying on their remaining useful vision to navigate in public (Vision Australia, n.d.-b). Approximately 5% of people with vision impairment who require a safety mobility device may have a guide dog (Vision Australia, n.d.-b). The remainder uses long white canes to detect objects in their path. Various cane techniques include keeping the tip in contact with the ground to the front and side of the body, sweeping the cane from side to side, constant contact sweep, or ‘shoreline’ technique to follow path or curb edges (Vision Australia, n.d.-b). Secondary electronic devices such as hand-held ultrasound sensors, used to identify solid objects within a 4-meter range between knee and head height, augment the primary feedback information provided by dog guides or long canes.
Case Presentation
The 69-year-old participant was totally blind due to retinitis pigmentosa, a genetic condition causing the retina to degenerate with subsequent vision loss (Vision Australia, n.d.-a). The onset of the condition was at age 25 years, with total blindness from age 33 years. The participant experienced constant paroxysmal nystagmus from birth, resulting in central vision short-sightedness and glare sensitivity, prior to the onset of retinitis pigmentosa symptoms. From the age of 30 years, they used a long white cane as the primary mobility device, which is now supplemented by a hand-held ultrasound. The aim of this case study was to provide a safe and effective setup of ISWT for a person who is blind and uses a mobility cane.
Methods
Ethical approval was provided by the Flinders University Human Research Ethics Committee (#4084). The participant provided informed, signed consent to participate in the study and to have photographs taken.
For the parent study investigating fatigue effects on postural balance, community-dwelling adults aged 40 to 74 years were recruited through local government. Eligible participants had not fallen in the previous six months; could walk at least 10 m; had no pain, trauma, or surgery in past 3 months affecting their back or lower limbs; no diagnosed neurological condition; and no medical condition where active participation in exercise was contraindicated (Fletcher et al., 2013). Interested parties contacted the research team who confirmed eligibility, provided study details, and arranged a testing site and venue for an hour of testing which incorporated two attempts at the ISWT.
The setting for this case study was a community center for people aged 50 years and older, run by local government. The testing was undertaken in a cleared room measuring 13.6 × 5.7 m. The floor surface was concrete overlaid with linoleum. The usual setup for this test was as per ISWT protocol (Harrison et al., 2013). This process incorporated two cones spaced 9 m apart, providing a 1/2 m at either end to turn, thereby making the total 10 m distance. Audio of the recorded introduction and tonal beeps was provided on a USB from Pulmonary and Cardiac Rehabilitation at University Hospitals of Leicester NHS Trust and played through a Bluetooth speaker (Harrison et al., 2013).
However, this setup was inadequate for the participant who is blind. Cones placed on the floor were in danger of being swept aside by the long cane. There were no cues to gauge the distance between turning points, to find the starting position for each 10-meter repeat, nor to maintain a straight line without veering on a tangent. Subsequently, the setup was amended. Lines of rope that were 2 mm in diameter were laid on the floor between the two turn-around points (see Figure 1). Lines were parallel, spaced 1.25 m apart, and taped to the floor by wide masking tape. The choice of rope that was 2 mm in diameter rope provided a “bump” for the sweeping cane without creating a tripping hazard. The right-hand line provided the tactile feedback for the direction of each 10-meter repeat.
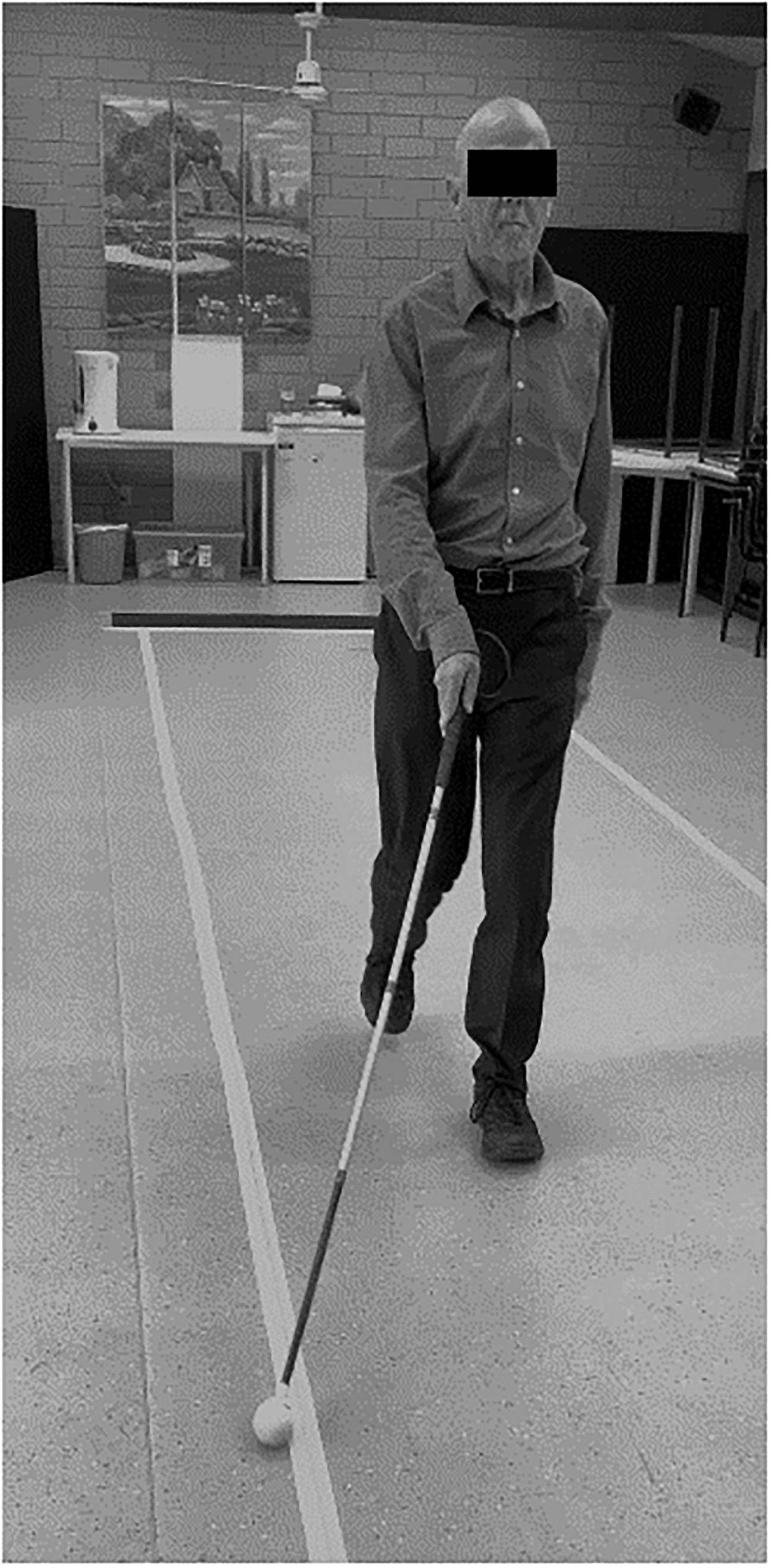
Illustration of the Walking Direction Guide: Photograph of a Person Using a White Mobility Cane and Taped-Down Rope to Guide Walking Direction.
The distance marker for turnaround was provided by carpet tiles that were 4 mm thick. Four tiles were laid side-to-side across the width of the walking track at the points usually marked by the two cones. The tiles were taped to the floor using wide masking tape to prevent the creation of a tripping hazard (see Figure 2). The tiles provided a change of surface texture underfoot, compared to all other areas of the room. The participant was instructed to walk onto the tiles to identify the correct distance, before turning 180° and negotiating the right side of the walking track for the return distance. This mimicked the additional half-meter accounted for walking around the cone in the usual setup.

Illustration of the Turning Guide: Photograph of a Person Using a White Mobility Cane Walking From Linoleum Onto Carpet Tiles That Are Taped to the Floor.
Results
There were no adverse events during testing. The participant completed two shuttle walk tests, per research protocol. The ropes and carpet tiles stayed in position during both tests, including when the participant was walking faster at 1.35 m/s (level 6). The participant's results (level 6, increment 3; and level 6, increment 8) were not statistically significantly different from the other participants (p > .05). At the end of the session, both rope and tiles were removed quickly and easily.
Discussion
The minor modifications to the floor setup enabled this participant to undertake the ISWT and participate in the research project, which would have been impossible without the amendments (Lima et al., 2019). The equipment required for the modifications (rope, masking tape, and carpet tiles) was inexpensive, easy to access, and straightforward to install. The ISWT was completed as per protocol with beeps indicating the timing for walking, and the test concluded when the participant was no longer able to make the 10-meter distance in the time required. Therefore, the taped-down rope for directional cues and tactile change to carpet tiles as the cue for turning did not change the integrity of the ISWT (Lima et al., 2019). Further consideration is required for people with low vision (for example, offering increased illumination or providing color contrast might indicate the edge of the walking track and turn-around points). Likewise, accommodating people who are blind using a high-bounce cane technique, or using marshmallow, roller, free-wheel, Dakota disc, or other cane tips may require a rope that is larger in diameter. Alternate considerations would be necessary for a person with low vision who does not use a cane or a blind person who uses a dog guide for mobility assistance. Also, for a person with dual-sensory impairment, a system that provides additional body-worn haptic feedback for the timing beeps would be required.
Limitations
Only one individual who is blind participated in this study; therefore, this article reports adaptation for this person, their preference for the use of a cane as a mobility device and their experience of the modifications. Permission for using tape on floors is recommended, since removing the tape from wooden floors may lift the varnish.
Footnotes
Acknowledgments
The parent study is a PhD research project undertaken by the primary author, who is funded by a scholarship from the ARC Digital Enhanced Living Hub. This work was possible thanks to consultation with Felicity Johnson, OAM, and Australian Paralympic cyclist.
Authors’ Note
The authors of this Practice Report made the following contributions: Nicky Baker—conceptualization, methodology, validation, investigation, analysis, writing original draft, review and editing, and visualization; Michael Taggart—resources and writing (review and editing); Winifred Taylor—investigation and writing (review and editing); and Sue Gordon—investigation, supervision, and writing (review and editing).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ARC Digital Enhanced Living Hub (PhD scholarship).