
Abstract
Introduction
Pediatric cataract is still a major cause for childhood visual impairment. The goal of our study was to analyze the prevalence of children with impaired vision (6/15 or worse) after surgery for bilateral cataract, to evaluate factors associated with it and to emphasize the importance for visual rehabilitation including the use of visual aids, educational measures, and social worker services.
Methods
Retrospective analysis of medical records from children who underwent surgery for cataract up to age 6 years, with a follow-up of at least 4 years. Clinical characteristics retrieved from medical records included visual acuity, presence of nystagmus and/or strabismus, age at surgery, intraocular lens (IOL) implantation, and others.
Results
Fifty-five children were included in the study. Follow-up ranged from 4 to 13 years (Mdn = 6.8). Visual impairment was found in 15/24 (62.5%) of children operated on before the age of 6 months (group 1), and in 7/31 (22.5%) n those operated after the age of 6 months (group 2; p = .019). Thirty-eight of the 55 children had a primary IOL implantation; nystagmus and microphthalmos were also associated with higher rates of visual impairment.
Discussion
Despite early and modern surgery, long-term visual outcome remains poor in children undergoing bilateral cataract surgery at young age. When discussing visual prognosis with parents, it is important to recognize factors associated with visual impairment, such as need for surgery before age 6 months, nystagmus and microphthalmos, as well as the importance for early visual rehabilitation services when needed.
Implications for Practitioners
Our study aims to highlight the high number of children left with visual impairment and blindness following modern and timely treatment for early cataract. Early referral for visual rehabilitation will optimize quality of life in these children and will probably allow a wider range of opportunities as adults.
Keywords
Despite being treatable, pediatric cataract remains a primary cause of visual impairment (i.e., blindness and low vision) in children across the world (Foster, Gilbert, & Rahi, 1997; Gilbert & Foster, 2001; Lundwall & Kugelberg, 2002). Based on this fact, the World Health Organization’s VISION 2020 program, “The Right to Sight,” has as a main priority to reduce the consequences of cataracts in children worldwide (Gilbert & Foster, 2001). Congenital cataracts are present in between 1 and 6 out of 10,000 live births in developed countries and between 5 and 15 out of 10,000 births in developing countries (Berry et al., 2020).
At least 50% of the congenital cataracts are characterized as inherited (mainly autosomal dominant); they can either develop as isolated cataract or as part of a syndrome. In recent years, knowledge about inherited diseases has advanced significantly, allowing greater understanding of the molecular basis of cataract (Berry et al., 2020; Zetterström et al., 2005). Panel testing allows a rapid evaluation of several potential cataract-causing genes. Identification of disease-causing gene variants may confirm the diagnosis, guide management decisions, and inform recurrence-risk assessments and genetic counseling.
In general, visual outcome following cataract surgery in children is worse than in adults, with visual deprivation due to early cataract onset, associated ocular developmental disorders, and delayed presentation being among the principal causes (Chaudhary, Lavaju, Shrestha, Shah, & Chaudhary, 2017). The intensive and prolonged treatment of children with congenital cataract is challenging and expensive (Wu, Long, Lin, & Liu, 2016). In the last few decades, visual outcome in children undergoing surgery for bilateral congenital cataract has improved notably due to early detection and modern surgical treatments (Bonaparte, Trivedi, Ramakrishnan, & Wilson, 2016; Gelbart, Hoyt, Jastrebski, & Marg, 1982; Kugelberg, 1992; Ledoux, Trivedi, Wilson, & Payne, 2007; Lloyd et al., 2007; Rogers, Tishler, Tsou, Hertle, & Fellows, 1981; Taylor, VaeganMorris, Rodgers, & Warland, 1979). However, visual impairment is still present in large numbers of children. Previous studies have suggested that several clinical factors may influence the visual outcome, including age at presentation and age at surgery, cataract type, whether or not an intraocular lens was primarily implanted, presence of nystagmus, developmental disorders of the eye, systemic conditions, and others (Bowman, Kabiru, Negretti, & Wood, 2007; Khan & Al-Dahmesh, 2009; Lambert et al., 2006; Lesueur, Arné, Chapotot, Thouvenin, & Malecaze, 1998; Lloyd et al., 2007; Trivedi, Wilson, & Golub, 2006).
Childhood visual impairment affects the child, their family, and society. It also interferes with the child’s development, education, and future life as an adult (Rahi & Cable, 2003). Recognizing factors related to visual impairment in children with bilateral cataract can help us predict the long-term visual outcome.
This study aims to report the prevalence of visual impairment in children undergoing early surgery for bilateral cataract in our population, to evaluate the multiple factors associated with poor visual outcomes, and raise awareness for referral to visual rehabilitation centers for children by physicians, educational practitioners, social workers, and nonmedical rehabilitation professionals.
Materials and Methods
We conducted a retrospective study with review of medical records from children who underwent bilateral cataract surgery between the years 2003 and 2012 at the Center for Pediatric Ophthalmology in coordination with the Michaelson Institute for Rehabilitation of Vision, at Hadassah-Hebrew University Hospital in Jerusalem, Israel. Approval for this study according to the Helsinki tenets was obtained from the Institutional Review Board at Hadassah-Hebrew University Medical Center, Jerusalem.
Inclusion criteria included all children who underwent surgery for cataract up to age 6 years, with a follow-up of at least 4 years and who were able to participate in visual acuity tests in order to quantify vision at the last follow-up visit. Details extracted from files included bilateral best corrected visual acuity, presence of nystagmus or strabismus or both before and after surgery, stereo vision, presence of microphthalmos, age at surgery, intraocular lens (IOL) implantation versus aphakia, number of additional surgeries, associated ocular or systemic disorders or both, and family history of congenital cataract. The surgical technique that was used in all cases was lensectomy through corneal approach, with or without IOL implantation, followed by posterior capsulotomy and anterior vitrectomy.
The primary outcome measure was final bilateral best corrected visual acuity using Snellen linear optotypes. Visual acuity was then categorized in two main groups: vision within typical limits (equal or better than 6/12) and visual impairment (6/15 or worse). Aphakic correction was done using contact lenses or glasses or both starting 1 week after surgery of first eye. Data were analyzed using IBM SPSS statistics 22 software. A descriptive statistics analysis was performed along with normality tests. A chi-square test was used for nominal variables and Kruskal–Wallis (nonparametric test) was used for quantitative variables.
Results
Fifty-five children were included in the study, 23 girls (41.8%) and 32 boys (58.2%). Follow-up ranged from 4 to 13 years (M = 7.7 years). The mean age at last examination was 9.33 years, with a standard deviation of 2.75 (M = 9.33, SD = 2.75).
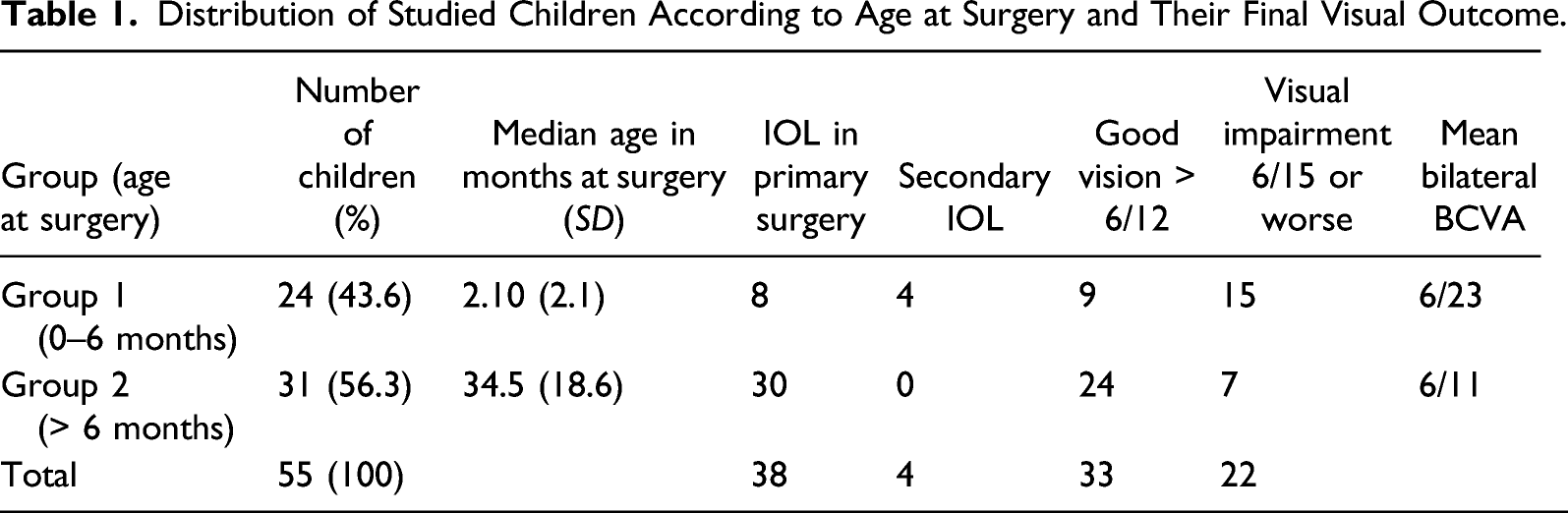
Distribution of Studied Children According to Age at Surgery and Their Final Visual Outcome.
Clinical Characteristics of Studied Children According to Age at Surgery Across Other Variables.
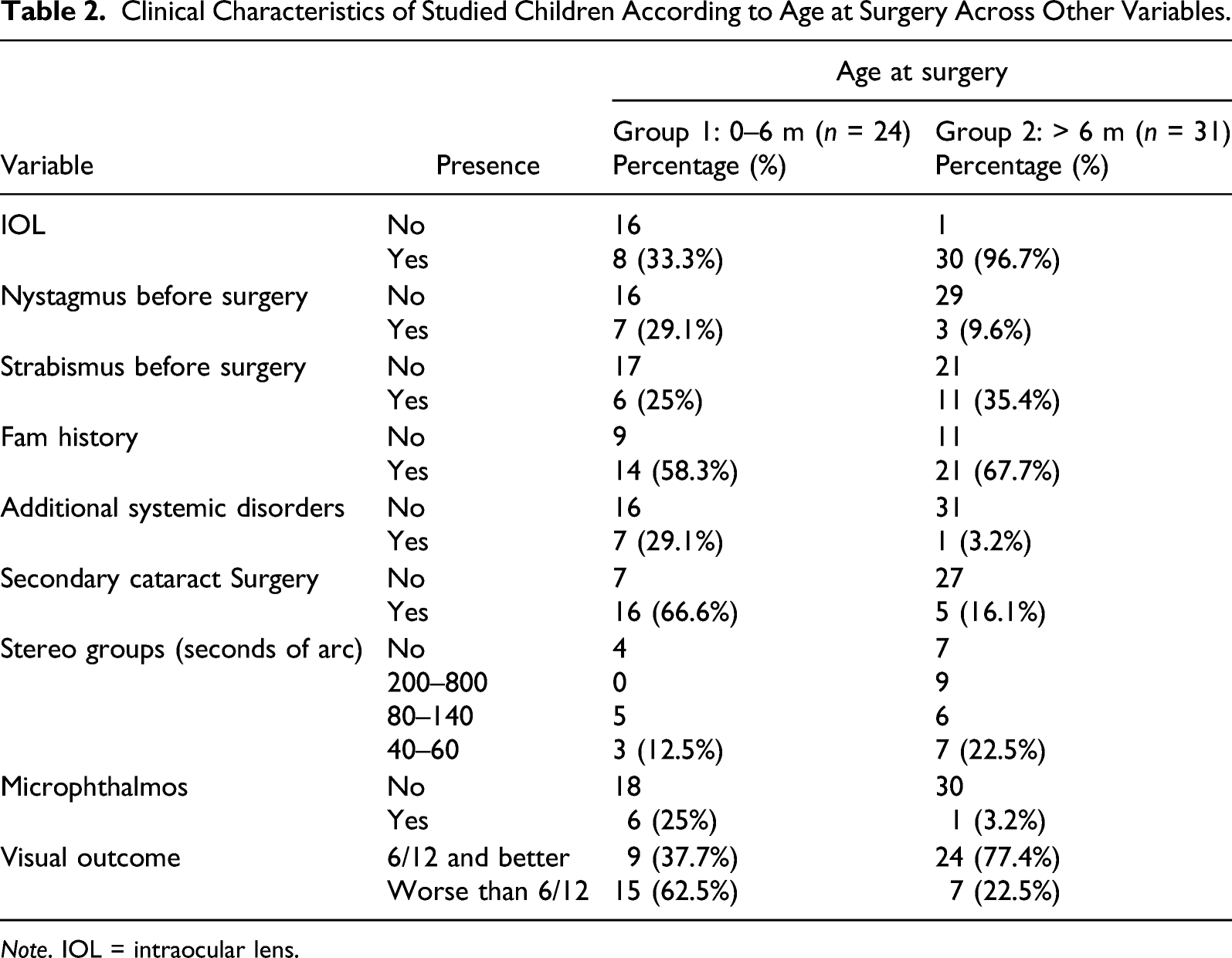
Note. IOL = intraocular lens.
Multiple Logistic Regression Model for Factors Associated With Visual Impairments.
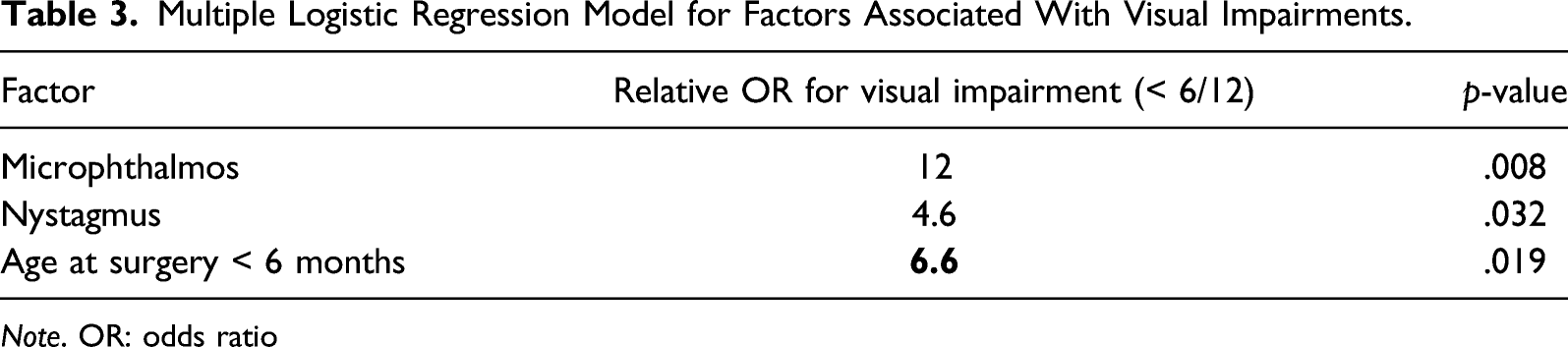
Note. OR: odds ratio
Visual Outcomes
Sixty percent of the children showed good visual acuity (6/12 or better) in their last examination and 40% of the children showed visual impairment (6/15 or less). Among girls, 39.1% had visual impairment compared to 40.6% in boys. Visual impairment was found in 15 of the 24 (62.5%) children who were operated on before the age of 6 months, and in 7 of 31 (22.5%) of those operated after at more than 6 months of age (X2(1) = 3.841, p = .019). Logistic regression analysis shows that the children who had surgery before the age of 6 months had 6.6 times higher risk of poor visual outcome compared with those who had surgery after 6 months of age.
Only four children had a visual acuity of 6/60 or lower (7.2%). All of them underwent early surgery (less than 6 months), two of them had nystagmus and two had microphthalmos. All of them had a history of systemic disorders. Mean visual acuity was worse in children who underwent surgery at a younger age. Fisher test p value = .019; linear-by-linear association p = .003.
IOL Implantation
Thirty-eight of the 55 (69%) children underwent a primary IOL implantation (8 of 24 from group 1; 30 of 31 from group 2). Later in life, four children from group 1 got a secondary IOL implanted. All but one of the aphakic children belonged to group 1. In group 1, from eight children who got a primary IOL implantation, 75% resulted in visual impairment; in the remaining 16 aphakic children in the same group, only 56% had visual impairment, suggesting that IOL implant before the age of 6 months might be related to higher chances for visual impairment in the future.
All aphakic children were corrected by contact lenses or glasses or both with excellent treatment compliance.
The association between the presence of an IOL implantation and visual outcome was not statistically significant (χ2 (1, N = 55) = 0.089, p = .766).
Nystagmus
Ten children (18.2%) had nystagmus before surgery, 7 of whom were left with visual impairment. At final follow-up examination, 15 children (27.3%) had nystagmus.
The association between the presence of nystagmus and visual outcome was significant: χ2 (1, N = 55) = 4.583, p = .032. Logistic regression analysis showed that children who had nystagmus had 4.6 times higher chances of developing visual impairment compared to those without it. Among children in group 1, 30% had nystagmus previous to surgery, compared to only 9% of children in group 2 (see Table 2).
Microphthalmos
Seven children (12.7%) had microphthalmos, 6 of whom developed visual impairment (85.7%), as compared with 33.3% among children without microphthalmos. The association between microphthalmos and the visual outcome was significant: χ2 (1, N = 55) = 6.984, p = .008. Six of the 7 children with microphthalmos belonged to group 1, as compared with only 1 child in group 2. Logistic regression analysis shows that the children who had microphthalmos had significantly poorer visual acuities (Wald = 4.899, p < .05) with an odds ratio of 12 times higher chances to develop visual impairment that children without it.
Strabismus
Seventeen children had strabismus before cataract surgery (Esotropia: 10 and Exotropia: 7); 11 of these children were in group 2. At last follow-up examination, 23 children had strabismus (esotropia, 8; exotropia, 15). The association between the presence or type of strabismus and visual outcome was not significant: χ2 (1, N = 55) = .511, p = .475.
Systemic Disorders
Eight children (14.5%) were found to have systemic disorders, including Fanconi syndrome, cerebral palsy, Lowe syndrome, and Cockayne syndrome, among others. Seven of the eight children were included in group 1. Among children with associated disorders, 71.4% had visual impairments, as compared to 35.4% among the children with no systemic disorder. However, this finding was not statistically significant: χ2 (1, N = 55) = 1.975, p = .160. Interestingly, all children with the poorest visual outcome in terms of visual acuity (< 6/60, 4/55) also had additional systemic disorders.
Additional Ocular Surgeries
The most common cause for additional surgeries was secondary cataract in 21/55 (38.1%), followed by strabismus (27.3%), secondary IOL implantation (7.2%), and glaucoma (7.3%).
In general, the children with visual impairments had undergone a higher number of additional surgeries (M = 2.36) as compared to those with good visual outcomes: χ2 (1, N = 55) = 10.065, p = .002.
The mean frequency of secondary cataract surgery is 0.75 per child (SD = 1.22) ranging from 0 to 6 surgeries per child. Children in group 1 had secondary cataract surgery in 66.6% of cases compared to only 16.1% of children in group 2.
Other Factors
Thirty-five children (63.6%) had a positive family history of congenital cataract, but it was not found to be associated with visual outcome. Forty-one children complied with stereo testing and results were distributed almost equally regarding different stereo ranges among the children. There was a tendency toward better stereo acuity among children in group 2.
Discussion
We have analyzed different factors associated with visual impairments in young children who underwent surgery for bilateral cataract. The children we studied included only those who could cooperate verbally during visual acuity tests at the last follow-up examination.
Among 55 children who underwent bilateral cataract surgery before the age of 6 years, we found that children who were younger than 6 months of age at the time of cataract extraction had 6.6 times higher risk of poor visual outcomes, compared with those who had surgery after the age of 6 months.
It has been previously shown that cataracts that appear during early infancy (i.e., in the first weeks of life) affect visual development much more than cataracts that develop after the most sensitive period of visual maturation in older children (Bonaparte et al., 2016). Delay in surgery during the first 3 months of life will further decrease the final visual outcome. Loss of one line in best corrected visual acuity for every 3 weeks of delay in surgery (up to age 14 weeks) has been reported (Birch, Cheng, Stager, Weakley, & Stager, 2009). It is therefore crucial to minimize deep deprivation amblyopia by early surgery in children born with dense bilateral cataracts. Removal of cataracts that develop in older children after the early stage of visual development often results in good visual outcomes (Birch et al., 2009). Bonaparte et al. published a study in 2016 with 157 children up to age 17.5 years who had received operations for bilateral cataracts with a minimal follow-up of 6 months. He found that the vision of 78% of the children who received operations was good enough to allow them to drive a vehicle (Bonaparte et al., 2016). (We surmise these findings show better visual results because of the inclusion of older children in comparison with our study.)
The study presented here shows that, among pre-operative risk factors, children with nystagmus were 4.6 times more likely to develop visual impairments (< 6/12), compared to those presenting without nystagmus. This finding is in accordance with previously published studies and might suggest that nystagmus appears as the consequence of an early and severe disruption in visual development (Bonaparte et al., 2016; Lambert et al., 2006; Robb & Petersen, 1992). Furthermore, its presence also affects the early critical period of visual development, which results in further visual impairment. Interestingly, despite early surgery, some children developed nystagmus later in life, most probably related with early visual deprivation.
Our study shows that children with microphthalmos have 12 times higher chances to develop visual impairments compared with children without this condition. Even though it is well known that microphthalmos is associated with a poorer prognosis for vision, we did not find any specifics in the literature on how this quantitatively affects visual outcome.
Among surgical factors, we have noticed that aphakia was apparently associated with higher rates of visual impairment in accordance to previous publications (Bonaparte et al., 2016). We believe that since all but one child with aphakia in our cohort had undergone cataract extraction before the age of 6 months, it is likely that the young age at surgery and not the aphakia itself is the cause for visual impairment. The young age at surgery in itself could be an indicator of those children with dense cataracts or microphthalmos. Thus, a poorer visual outcome may in fact be related to the type of eyes left aphakic more than the aphakia itself.
There is no agreement in the literature regarding the optimal age at which to implant an IOL in young children. Several authors report that primary IOL implantation appears beneficial over aphakia, in terms of visual outcomes (Bonaparte et al., 2016; Lesueur et al., 1998). In our cohort, we found that children who had received operations when they were younger than 6 months of age, those with an IOL implant, had higher incidence of visual impairment. On the other hand, we found a clear tendency toward better visual outcomes with IOL implantation in children who were older than 6 months of age. It has been previously published in the literature that IOL implantation can be done with manageable side-effects in children older than 6 months of age as previously suggested for unilateral congenital cataract (Infant Aphakia Treatment Study Group et al., 2014; Lambert et al., 2019). A recently published prospective study, conducted by the British Isles Congenital Cataract Interest Group, found that an IOL implant in primary surgery does not confer better vision or protect against secondary glaucoma in children operated under the age of 2 years (Solebo, Cumberland, & Rahi, 2018).
Glaucoma was observed in 7% of operated children and was not related with significant poorer visual outcome. This rate of secondary glaucoma is low compared to the study by published by Scott, where the frequency of developing glaucoma following early cataract surgery was 2/3 of operated children (Scott, Purohit, Superak, Lynn, & Beck, 2013). Similar to our data, in their study, glaucoma was not associated with poor visual outcome.
Our study found that children who underwent several surgical procedures were at a higher risk to develop a poorer visual outcome. The younger the child at cataract extraction, the higher the number of additional surgeries.
Finally, in our cohort, we did not find any significant correlation between gender, presence of strabismus prior to surgery, family history of congenital cataract, or associated systemic abnormalities with final visual outcome.
Limitations of our study include the retrospective nature of the study that limited us in obtaining important information such as type of cataract, percentage of visual axis obscured, time elapsed between secondary cataract and re-operation, and others. Our study sample did not include children with more severe disabilities who could not verbally respond to the visual acuity tests, limiting our findings only to the sampling frame. Also, surgeries were performed by one of three different surgeons. However, all surgeons were trained pediatric ophthalmologists with special expertise in pediatric cataracts.
The strength of this study is based on a long-term follow-up of 55 treated children who were cooperative with visual tests, making it possible to consider our findings reliable.
In conclusion, visual impairment was found in 62.5 % of children with dense bilateral cataract requiring early surgery (< 6 months). Other pre-operative factors related to visual impairment were microphthalmos and nystagmus. These data will aid us to better predict the expected visual outcome, assist physicians when discussing the future of children diagnosed with cataract at an early age, and raise awareness of the need for referral of these children to visual rehabilitation as early as possible. Even children who have severe visual impairment without any further medical treatment available can be assisted with visual devices, educational guidance, governmental aid, and support groups to help improve their quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.