
Abstract
Previous research has shown that injuries are a global burden, and people with different disabilities, impairments, and chronic diseases are especially vulnerable to injury events (e.g., Clarke, Ailshire, Nieuwenhuijsen, & de Kleijn – de Vrankrijker, 2011; Percival, Hanson, & Osipovic, 2006; Worth, 2013; Xiang, Kidwell, & Wheeler, 2008). However, there is a lack of research related to this subject and, therefore, a need to further develop knowledge in order to ensure safe surroundings for everyone (Kulmala et al., 2008; Legood, Scuffham, & Cryer, 2002). In view of this need, the present study contributes by examining the experiences and knowledge of hospital social workers in Sweden concerning injury risks, injury events, and injury prevention for individuals with visual impairments (i.e., those who are blind or have low vision).
Aim and research questions
This study was designed to survey a total sample of hospital social workers specializing in visual impairment. The aim of the study was to examine hospital social workers’ experiences of injury events and to identify prevention strategies based on their professional practice. There were two research questions which are as follows: To what extent do hospital social workers meet with patients who have undergone an injury event in the residential environment? In what ways do hospital social workers think they can work more preventively against injury events?
Framework
The study framework was based on two parts: the professional role of a hospital social worker, and a brief overview of previous research on injury prevention.
Hospital social workers as a profession in Sweden
Hospital social workers in health and medical care have an important task and role not only in supporting people in vulnerable life situations by providing social support, guidance in different societal support systems, and support and advice in how to use assistive devices, but also by supporting the individual and their rights (United Nations General Assembly, 2006, 2015; United Nations High Commissioner for Human Rights, 2014). In short, the hospital social worker’s main role is to enable good social living conditions (cf. World Health Organization, 2011). In Sweden, the importance of hospital social workers has been acknowledged in various studies (Olsson, 1999; Sernbo, 2019; Sjöström, 2013).
Moreover, the Swedish welfare system has institutionalized specific supports for individuals with visual impairments. It is estimated that there are approximately 200,000 individuals who are visually impaired in Sweden (Specsaver and the Swedish Association of the Visually Impaired, 2018). Low vision work has been conducted in Sweden since the 1950s, and today, each region or county council has a center for people with visual impairments (Bäckman et al., 2015; Ståhl, 2018). In line with the development of low vision work, different devices or aids have been developed and used by persons with visual impairment in Sweden such as talking books, computer-based assistive technologies, optical and electronic-optical devices, long canes for mobility, dog guides, and transportation services (Bäckman, 1994).
In addition to vision centers, Sweden also has 34 low vision clinics, located at general and university hospitals. These clinics are responsible for both habilitation and rehabilitation for people with visual impairments of all ages. In order to receive support and rehabilitation at a low vision clinic, a referral from an ophthalmologist is required. The clinics are regulated by the Health and Medical Services Act (1982:763).
The rehabilitation and habilitation at low vision clinics are conducted by multidisciplinary specialist teams. These teams include hospital social workers, psychologists, physiotherapists, orthoptists, optometrists, occupational therapists, and low vision therapists. The role of the hospital social worker at a low vision clinic is, for example, to help the patients or parents and family members with different contacts with authorities, applications for funding and personal counseling, and to give social support to the patients, parents, and other family members.
Even if these support systems are institutionalized in the welfare context, however, previous research has found that individuals with different disabilities and impairments perceived social workers as untrustworthy, mainly because they felt that the social workers had not paid attention to them and their story (Lundälv, 2018). A study found that social workers are stressed and seldom have time to listen to patients' stories about accidents, but also that people with visual impairments sometimes did not want to talk about accidents, since they wanted to be able to move on from the incidents (Lundälv, 2018, p. 93). Consequently, it is not only the institutionalization of the professional role that is of importance but also the concept of trustful dialogues (Buber, 1970; Erikson, 1950; Hanssen, 2007). Trustful dialogues are here defined as a specific form of relation between the care giver and the patient that will lead to a positive outcome for both parts. The trustful dialogue is focused on acknowledgment, respect, and trust; one that is meaningful for both the care giver and the receiver of care (Larsson & Lundälv, 2019:77). In combination with basic trust and intersubjectivity, trustful dialogues are important in establishing relations and interactions in which the patient feels safe, understood, and listened to.
A brief summary of injury prevention
Many studies have examined and discussed injury prevention for individuals with visual impairments. In this section, we will briefly summarize some of these findings; we do not aim to provide a comprehensive overview of all literature in the field.
It is important to acknowledge that the pattern of injury occurrence differs between individuals with and without disabilities, which makes it harder to define general recommendations (cf. Thodelius, Ekman, Lundälv & Ekbrand, 2017). Prevention can be aimed at the individual or environmental factors in the individual’s vicinity. For individuals with vision loss, the prevention literature primarily focuses on environmental modifications. For example, modifying housing designs and interior layouts, which are beneficial prevention measures for people with different degrees of visual impairment (Bowes, Dawson, Greasley-Adams, & McCabe, 2016; Brunström, Sörensen, Alsterstad, & Sjöstrand, 2004; Den Brinker et al., 2005; Ehrlich, Hassan, & Stagg, 2019; Imbrie, 2004; La Grow, Robertson, Campbell, Clarke, & Kerse, 2006; Nguyen, Vu, Tran, & Nguyen, 2016; Paterson, 2011; Yonge et al., 2017).
To enable effective environmental strategies, however, it is important to work with the knowledge and engagement of different stakeholders and health professionals (Rooney et al., 2016). The article presented here examines the experiences and knowledge of hospital social workers in Sweden regarding meetings with visual impaired patients who have experienced injury events in residential environments, to enable a firmer discussion of prevention in line with the arguments of Rooney et al. (2016).
Method
The method was chosen in relation to the study’s dual aim: to examine hospital social workers’ experiences of patients' injury events and to identify prevention strategies based on their professional practices. To achieve this aim, a questionnaire was designed and distributed to hospital social workers who specialized in working with patients with visual impairments (cf. Mathers, Fox, & Hunn, 2007, p. 5).
Data collection and analysis
The questionnaire was distributed in October 2017, when hospital social workers from all over Sweden gathered for two days of supplementary training (i.e., quota sampling; see Mathers et al., 2007, p. 13). One of the authors participated in this training and informed the hospital social workers about the study. This direct notification about the study seemed to have a positive effect on both the response rate (67%; 30 of 45 participants answered the survey) and the construct validity (Heale & Twycross, 2015), since it made it possible for the respondents to ask questions and make clarifications if necessary.
The questionnaire covered both comparable numeric data and subjectively perceived experiences and opinions (Bryman, 2016). Of the 14 questions included, 9 were constructed as fixed-response questions and five as free-text answers (see Supplementary Appendix A).
The data were analyzed in line with what Creswell defines as a convergent parallel mixed method (2014, p. 267). The numeric data were descriptively summarized and interpreted via frequency tables, while the free-text answers were qualitatively coded and analyzed with a content analysis (Krippendorff, 1980; Nolan & Heinzen, 2014, p. 3).
Ethical considerations
The study was approved by the Ethical Review Board in Gothenburg (ref: 366–16, 2016), and the data collection, analysis, and presentation of the results adhered to the ethical principles discussed in the literature (Beauchamp & Childress, 2013; Swedish Research Council, 2017). During data collection, the respondents were informed that their participation was optional, that they would be anonymous, and that the researchers were interested in their professional experiences and not their personal opinions (Barron, 1999; Cöster, 2014).
Results
Before we present the main results of the study, we will give a brief summary of the respondents’ professional background. A majority had long professional experience in the visual field; approximately 80% (24 respondents) had worked in this field for more than five years. The respondents also had experience in working with patients of various ages; 67% had worked with both younger people and those older than 65 years. They had received supplementary training regularly; 50% during the last 36 months. The respondents therefore seemed to have the experience and knowledge that are crucial for development of efficacious preventive work.
Risks and injury events in residential settings
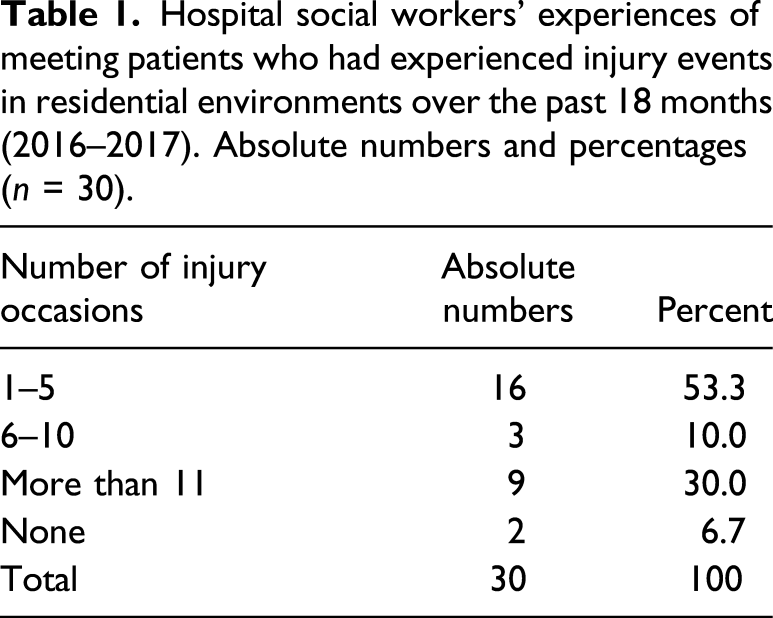
Hospital social workers’ experiences of meeting patients who had experienced injury events in residential environments over the past 18 months (2016–2017). Absolute numbers and percentages (n = 30).
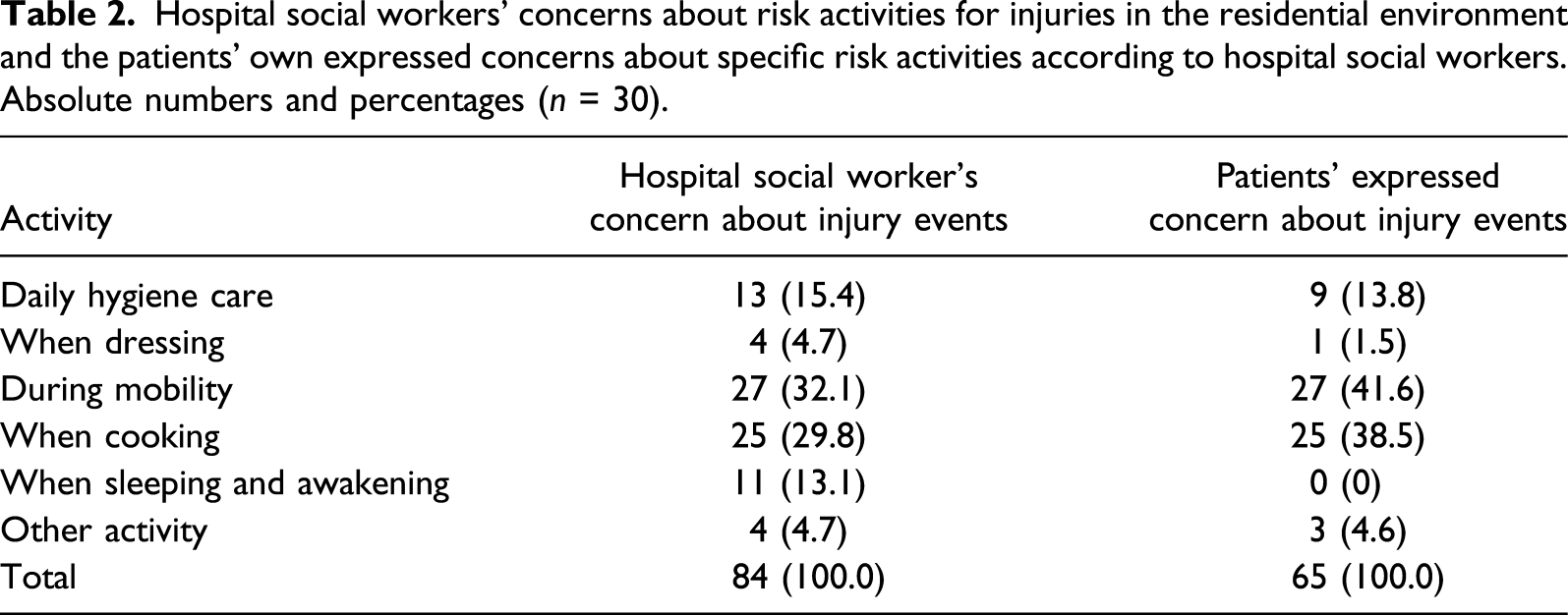
Hospital social workers’ concerns about risk activities for injuries in the residential environment and the patients’ own expressed concerns about specific risk activities according to hospital social workers. Absolute numbers and percentages (n = 30).
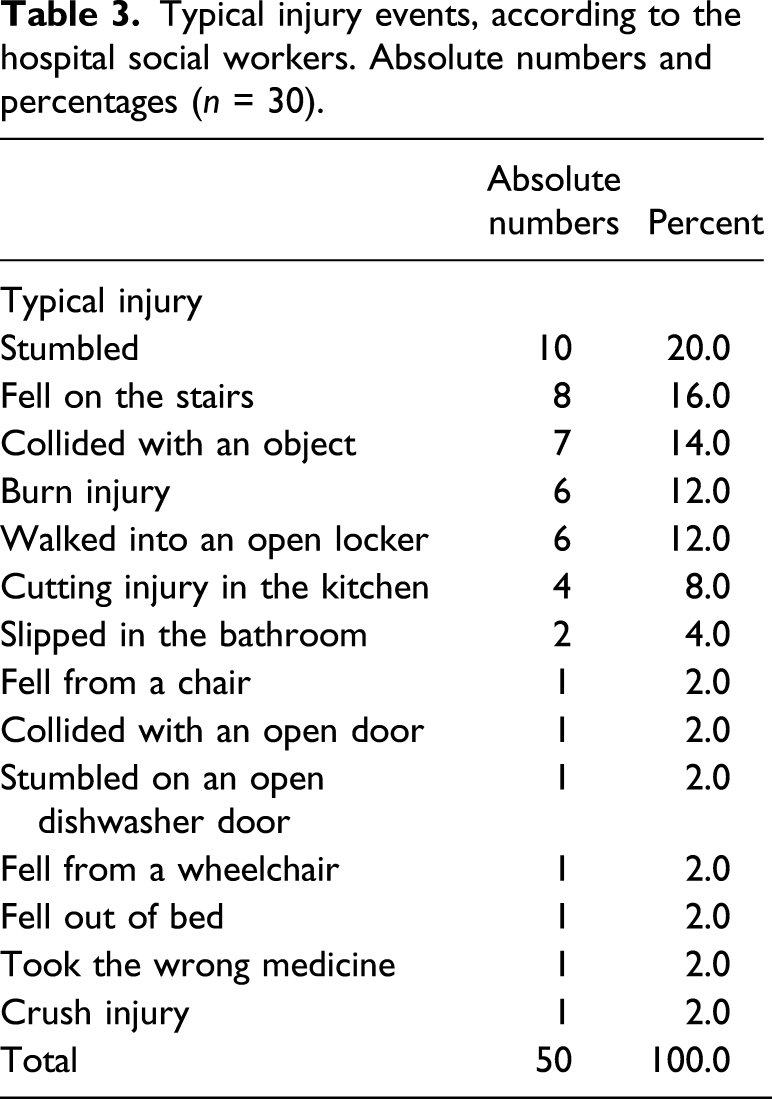
Typical injury events, according to the hospital social workers. Absolute numbers and percentages (n = 30).
Risk factors of injury events according to hospital social workers. Absolute numbers and percentages (n = 30).
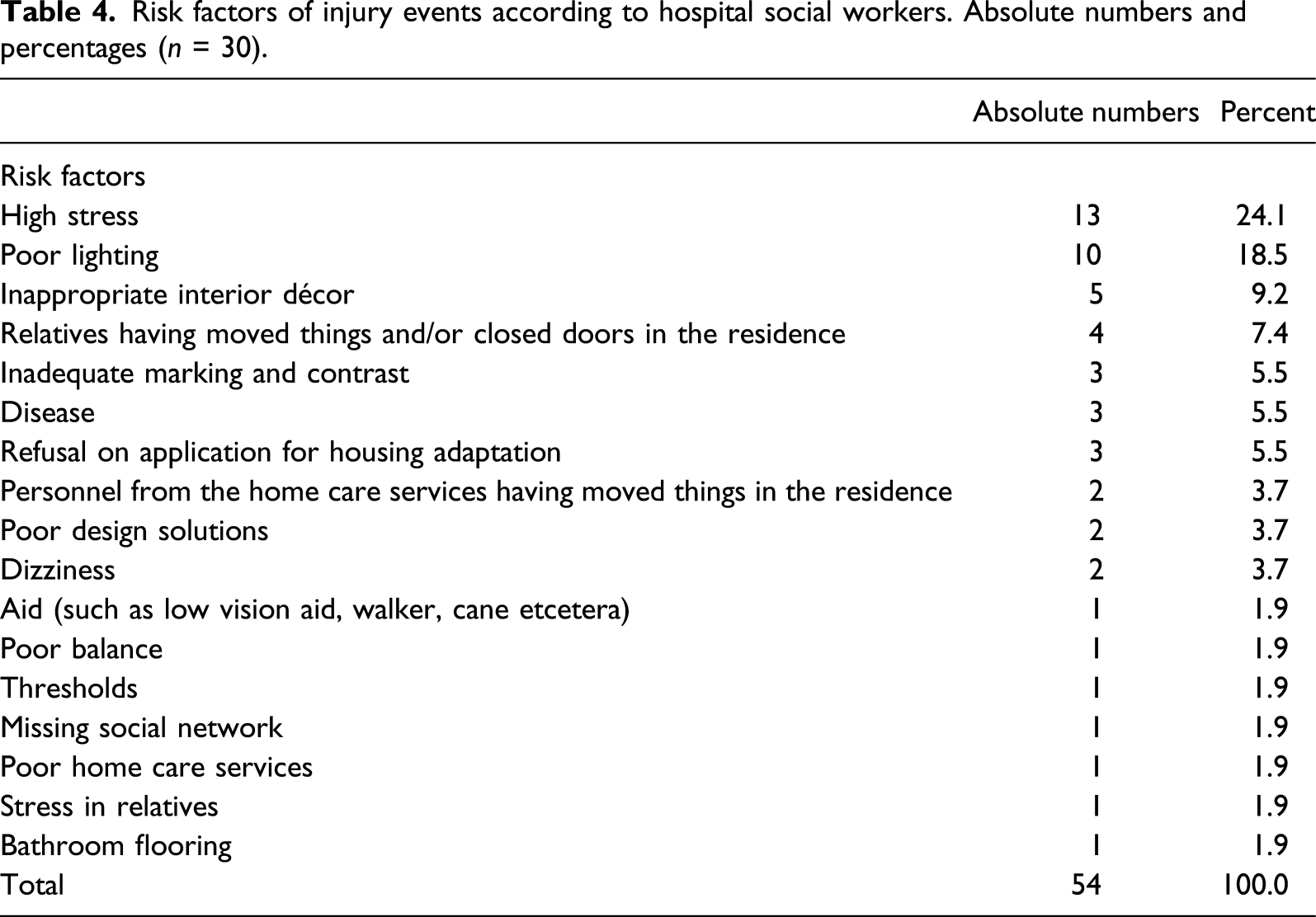
These results make it clear that injury events in residential settings are due to the interrelation between intrinsic (or personal) factors such as age, stress, or disease and extrinsic (or environmental) factors relating to design, lightning, or flooring. Injury occurrence is therefore closely related to everyday activity rather than to extraordinary conditions or activities. It is important to acknowledge this in preventive work.
On prevention: The role of hospital social workers’ experience
Most of the respondents (70%) thought that their patients were actively preventing injury events in the residential setting in different ways, but they still saw a need for more tailored information and education about risks targeting this patient group. As one respondent said: “We need to encourage solutions, information, and motivation.” Preventive work also included identifying risks in the residential environment by offering home visits and making suggestions for modification or improvement. However, this approach could also be counterproductive, as one respondent stated: “Talking to the patient about feelings and risks in the residential environment, to reduce anxiety, can lead to the onset of injuries and stress.” Preventive work included a broad spectrum of strategies targeting actors and stakeholders on the individual level, group level, and community level, mainly by having contact with other professions, working in teams, and developing their own networks. One respondent highlighted the importance of “networking with other actors such as occupational therapists, relatives, assistance officers and others,” mentioning “[o]ur teamwork/other professions and opticians (employer), housing adaptation, home visits, certificates, group activities, municipality.” However, strategies were also related to challenges in everyday work, mainly on an organizational level. As one respondent stated, the care organization as whole needed to “[c]ollaborate more in the teams around the user, make sure that the influence of the hospital social worker, and our observations, are acknowledged in the organization.”
Discussion
We return to our two research questions: To what extent do hospital social workers meet with patients who have experienced an injury event in the residential environment? And in what ways do hospital social workers think they can work more preventively against injury events? This study clearly shows that hospital social workers have extensive experience and knowledge of both injury risks and injury events. These results are in line with previous studies and also confirm that injury events among individuals with visual impairments are quite common (Clarke et al., 2011; Percival et al., 2006; Worth, 2013; Xiang et al., 2008).
The hospital social workers in this study had experience and knowledge of both risky activities and intrinsic and extrinsic factors, which can be formulated as distinctive ideas for preventive work. As seen in the results, injuries tend to occur because of an interrelation between individuals’ personal traits, environmental factors, and sometimes other actors such as relatives or other professionals, a finding that emphasizes the point that injury prevention needs to target both actors and environmental factors. The knowledge from hospital social workers needs to be communicated not only to the patient but also to other caregivers, relatives, and family members. As seen in the results, the question of networking and working with other professionals was one part in the preventive work, a finding that is in line with Bolin Björklund’s study (2014), which showed the need for more cooperation in multidisciplinary teams, especially at low vision clinics.
Preventive work needs to acknowledge the fact that individuals with visual impairments have a different perception of the spatial environment (Berndtsson & Kroksmark, 2008, p. 38), which can be hard to grasp from an outside perspective. It is important to be able to change perspective and work intersubjectively, and hospital social workers need to set aside time for patients to talk about risks and injury events in the residential environment. Along these lines, it is equally important to discuss experiences of “near-risk situations” and coping strategies (Lundälv, 2018). Letting patients with visual impairments talk about their experiences during visits with hospital social workers can help both the patient and others in the same situation, by extending patients’ and professionals’ knowledge of situations and useful strategies. Trustful dialogues such as these also offer a way to handle discrepancies in risk estimation between patients and professionals. If these discrepancies are not correctly handled, there may be consequences. It is possible that the preventive measure will fail since the individual does not adhere to it. The measure may be counterproductive if it leads to overprotecting (Shakespeare, 2013, p. 220); a healthy amount of risk-taking can both emancipate individuals with disability and impairment and let them live independently.
Conclusion
The present results highlight three important findings. First, injuries occur in everyday activities, they are not rare events conditioned by extraordinary circumstances. Second, injury occurs when internal and external factors emerge, which can be prevented by both working with environmental external factors and providing information to patients and their relatives. Third, it is important to perform preventive work collaboratively. Interdisciplinary collaboration among professionals can be challenging, but it is also a route to success, since different actors have different knowledge that can strengthen preventive work. It is not only collaboration between different health care actors that is necessary but also collaboration between health care and patients’ advocacy organizations. Since hospital social workers work alone to a large extent, it is important for them to keep in touch with each other through telephone and various networking meetings. By keeping in touch and exchanging information and experiences, a sharing of their tacit knowledge can take place.
Limitations and suggestion for further research
This study has two limitations. We did not ask any questions regarding similarities and differences between people with congenital and acquired visual impairments. We also did not investigate regional differences; thus, we were not able to examine within-region variation on a national level. Future research should analyze any similarities and differences between people with congenital and acquired visual impairments, which are of importance for preventive work. In addition, regional differences in praxis and relations should be investigated in order to understand and improve the communication between hospital social workers, patients, relatives, and caretakers. Especially the role of relatives needs to be explored further in the future, since the results of this study suggest that they have a significant role in both injury occurrence and in preventive work.
Supplemental Material
sj-pdf-1-jvb-10.1177_0145482X211046666 – Supplemental Material for Risk of Injury Events in Patients With Visual Impairments: A Swedish Survey Study Among Hospital Social Workers
Supplemental Material, sj-pdf-1-jvb-10.1177_0145482X211046666 for Risk of Injury Events in Patients With Visual Impairments: A Swedish Survey Study Among Hospital Social Workers by Jörgen Lundälv and Charlotta Thodelius in Journal of Visual Impairment & Blindness
Footnotes
Acknowledgements
This study is a part in a research project concerning risks and injury events in residential environments (ArchSafe) during 2014–2018 at Chalmers University of Technology, Gothenburg, Sweden and University of Gothenburg, Gothenburg, Sweden. The authors would like to thank all the study participants who contributed their knowledge and experience. The authors would also express our gratitude to the Swedish Civil Contingencies Agency (MSB), who funded the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.