
Abstract
Deficits in positive emotion regulation skills may be an important factor in the development and maintenance of anxiety and mood disorders. A treatment, which includes strategies to build and strengthen positive emotion regulation skills has been provided to patients primarily diagnosed with an anxiety and or mood disorder in an adult mental health outpatient service setting. To study the effects on positive and negative emotion, emotion regulation skills, emotional disorder symptoms, quality of life, and wellbeing during a new developed treatment. An exploratory clinical trial was used to conduct a preliminary assessment of a novel intervention. The intervention was provided in a group format over a 6-week period and independent practice over an 8-week period. Outcome variables were assessed pre- and post-treatment and at a 2-month follow up. Life quality, subjective wellbeing ratings, depressive and anxiety symptoms improved at follow up. The data suggests that the intervention may have the potential to produce desired change in positive emotion regulation. Preliminary findings suggest the intervention can have beneficial effects. These findings are promising and support the possibility that disturbances in positive emotion regulation may be a generative target for treatment research.
Highlights
An exploratory clinical trial was used to conduct a preliminary assessment of a novel group treatment intervention named “Building resilience.”
“Building resilience” includes strategies to build and strengthen positive emotion regulation skills.
Preliminary results across patients show improvements and the findings suggest the intervention can have beneficial effect on anxiety and depressive symptoms for individuals with a number of different principal and comorbid emotional disorders.
These findings are promising and support the possibility that disturbances in positive emotion regulation may be a generative target for treatment research.
Introduction
Positive Psychology
Clinical psychology and psychiatry has been focused on reducing suffering but mental health is more than just the absence of mental illness. There is a growing interest in understanding the cause and consequences of positive functioning, that is, behavior contributing to personal development, mental health and wellbeing. Positive psychotherapy is emerging as a new form of intervention and the techniques should teach people effective pathways to improved functioning and wellbeing (Seligman, 2011). Being able to handle negative events in ways that reduce distress does not guarantee that one will experience positive events in ways that promote wellbeing (Bryant & Veroff, 1984). Meta-analysis of randomized controlled studies of positive psychology interventions have shown small but significant effect sizes for subjective wellbeing and psychological wellbeing, as well as in helping to reduce depressive symptoms indicating that the effects are fairly sustainable (Boiler et al., 2013).
Emotion Regulation Theory
Research has shown that positive emotions, that is, emotions that we typically find pleasurable to experience are important to optimal health, functioning, and wellbeing and contribute to resilience against psychological dysfunction (Carl, 2015). Clinical disorders particularly anxiety and mood disorders are associated with deficits in positive emotionality (Carl et al., 2013), and may be an important factor in the development and maintenance of anxiety and mood disorders and hinder a complete recovery from mental illness (Barlow et al., 2011; Garland et al., 2010).
Emotion regulation theory suggests that people can maintain, increase or decrease emotions or attempt to cultivate specific emotions (Parrott, 1993). Facing the same positive event two individuals will anticipate, enjoy, and reminisce to different extents and therefore experience different levels of positive emotionality and wellbeing. It is not only the frequency of pleasant experiences or the ability to feel pleasure that matters to wellbeing but also the capacity to upregulate and savor positive emotions (Bryant, 2003). Csikszentmihalyi (2003) has in his research discovered that people were most creative, productive, and often happiest when they were in a state of flow. Flow he defines as “A state in which people are so involved in an activity that nothing else seems to matter; the experience is so enjoyable that people will continue to do it even at great cost, for the sheer sake of doing it.” Depression and anxiety hinder flow, intimacy, and personal development. Happiness is an internal state of being not an external one and happiness levels can be shifted through the introduction of more flow (Csikszentmihalyi, 2003).
Individuals with elevated symptoms of panic disorder, agoraphobia, obsessive-compulsive disorder, social phobia, generalized anxiety disorder, and unipolar depressive disorders all show increased tendencies to downregulate rather than upregulate positive emotions (Carl et al., 2013). Positive emotion regulation deficits likely contribute to differences in positive emotionality and may function as risk or maintaining factors in the onset and course of affective disorders. Positive emotion regulation deficits appear to represent promising therapeutic targets in the treatment of emotional disorders (Carl et al., 2013).
Resilience
The word resilience comes from the Latin verb resilire (to rebound). As a living system a human individual could be described as resilient when showing a pattern of adaptation or recovery in the context of potentially destabilizing threats. The study of resilience ultimately has a practical goal, to inform efforts to change the odds in favor of positive adaptation and development. Self-regulatory capacity including self-management of attention, arousal, emotions and actions appear to play a central role in human adaption, development, and resilience and this can fluctuate over one’s life course (Masten, 2014). There is little evidence to support the view that resilience is a trait (Masten, 2014). Resilience as a coping strategy can be trained and this training stems from cognitive behavioral psychology (Ivitzan et al., 2016; Masten, 2014).
Effective and evidence-based resilience programs have been found to include variables that not only focus on decreasing negative psychological and physical functioning in the face of stress and adversity but also increasing behavior leading toward personal development in daily life (Ivitzan et al., 2016).
Building a Treatment Intervention
Research on methods building and fostering resilience in adult mental health service settings is scarce. Clinical interventions generally work on positive emotionality in an indirect way (Carl et al., 2013).
The Unified Protocol for Trans diagnostic Treatment of Emotional Disorders (UP; Barlow et al., 2011) focuses on first enhancing awareness of the nature and function of emotions and then teaches skills for regulating one’s attention, interpretations and behaviors in the service of long-term goals. Such a model is readily adaptable to a focus on positive emotion regulation skills. Based on the UP method Carl (2015) developed a CBT intervention package addressing the specific deficits in positive emotionality in emotional disorders. This intervention was tested on a group of patients who had undergone prior treatment with CBT. Results support the potential utility of this intervention for addressing residual anxiety and depressive symptoms and increasing overall mental health. Moderate to large size effects were notable considering the participants had just received a full course of CBT. The interventions were found to be acceptable and feasible by the participants and could have beneficial effects for individuals with a number of different principal and comorbid emotional disorders. The treatment outline and techniques from the study by Carl (2015) were implemented in this group treatment program.
Overall the treatment program developed for this study is based on theory and research related to emotional regulation theory. Interventions from positive psychology (Ivitzan et al., 2016; Seligman, 2006, 2011; Seligman et al., 2005) were incorporated into the treatment program with the aim to build the ability to focus attention to what is good, increase awareness of mixed emotional states and expand focus from the self toward others generating a sense of belonging. To increase a sense of meaning and a focus on the present moment despite external circumstances attentional skills were trained according to flow theory (Csikszentmihalyi, 2003). This study anticipates to assess if introducing the focus on building these skills can alleviate some of the negative effects of mental illness, in particular depression and anxiety.
Study Aim
To study the effects on positive and negative emotion, emotion regulation skills, emotional disorder symptoms, quality of life and wellbeing during a new developed treatment.
Hypotheses
The intervention would generate improvement in participants’ positive emotion regulation skills (SBI).
Measures of positive emotion would improve from baseline after the intervention and follow up phases (SHI; BAS).
Depressive symptoms (BDI-II) and anxiety (BAI) would decrease from the baseline to intervention and follow up phases.
Improvements in positive emotion regulation skills (SBI) would be associated with beneficial changes in quality of life (BBQ) and life satisfaction (SWLS).
All outcomes would show continued improvement after the intervention until follow up.
The intervention would demonstrate feasibility and acceptability as assessed through retention of patients and patient ratings of acceptability and satisfaction on the Feedback form after the intervention.
Method
Study Design
This study used an exploratory clinical trial for conducting a preliminary assessment of a novel intervention. Primary outcome variables and major assessments were conducted at baseline, after treatment and at a 2-month follow up. These included self-report and independent evaluation rated components. The group treatment program was administered by a Clinical Psychologist with a post graduate diploma in CBT for complex cases and 19 years of clinical experience working in psychiatric treatment settings. Interventions have previously been found to be more effective if they were of longer duration (Boiler et al., 2013). As the target populations generally suffer from moderate to severe levels of depression and anxiety the interventions have been extended over a longer time frame compared to the study by Carl (2015). An open clinical trial was completed with repeated measures allowing for change to be tracked over time. The treatment program was provided in a group therapy format with six treatment sessions (90 min) and one post intervention follow up.
Participants
Participants were recruited from the adult outpatient mental health service in Sweden. Eligible individuals have been diagnosed with an anxiety and/or a mood disorder. The recruitment period was during 1 month. Information about the study was placed in the waiting room and staff would give out a standardized letter explaining the treatment procedure to all patients eligible to participate that had scheduled appointments during this time period. All participants who wanted to participate gave informed consent. Potential participants completed a brief screen to determine eligibility and interest in participation. Positive emotion regulation skills were assessed using the Savoring Beliefs Inventory (SBI; Bryant, 2003), a 24-item self-report measure that assesses attitudes regarding tendencies to maintain and upregulate positive emotions. Individuals with 34 or less on the SBI, who did not meet exclusion criteria, were eligible for the study, using the same initial screening instrument and cut off as in the study by Carl (2015). Exclusion criteria were the following: (a). Acute risk factors (suicidal or homicidal ideations or clinical condition requiring immediate treatment) and (b). The individual was unable or unwilling to commit to the duration of the study and study procedures.
Seventeen individuals were screened for the study and 15 (88%) were eligible. All those eligible selected to participate in the study. The recruitment goal was to have two treatment groups each comprising of six to eight participants. In the first group 6 participants completed the study and two dropped out. One dropped from the study after three sessions due to finding it too difficult to talk about emotions, and a second was unable to continue with the study after five sessions due to the emergence of acute personal issues. In the second group 4 completed the study and three dropped out. This group began in March 2020 at the time when Covid-19 regulations were set in place. One decided to leave the study directly due to the emergence of the pandemic requesting to be placed in a later study after the pandemic, the other two dropped out due to having flu like symptoms early in the study. Data from 10 study completers are included in the analyses (attrition rate 67%). They were not given any remuneration for participating in the study.
Description of Assessment Measures
Savoring Beliefs Inventory (SBI)
SBI is a 24 item self-reported measure designed to assess attitudes toward savoring positive experience within three temporal orientations: the past (reminiscence), the present moment (present enjoyment), and the future (anticipation). It is a valid and reliable measure for assessing personal beliefs about savoring capacity to help clinicians evaluate the relative strengths and weaknesses of their clients in managing positive affect (Bryant, 2003). SBI total score showed a very good internal consistency (Cronbach’s alpha between .88 and .94), and the three subscales generally showed good convergent and discriminant validity. Test-retest correlations indicated strong temporal reliability (SBI total score r = .85; Anticipating subscale, r = .80; Present moment subscale, r = .88; and Reminiscing subscale, r = .85, all p < .0001). This measure was given initially to screen eligible candidates for the study. For the people who participated it was given again at the start, at the end of treatment and at follow up.
Steen Happiness Index (SHI)
The SHI is comprised of 20 items that require the participant to choose from one of five statements that most closely reflects how they have felt over the past week. Response choices range from a negative (1) to an extreme positive (5), as in the following example: Most of the time I am bored (a); Most of the time I am neither bored nor interested in what I am doing (b); Most of the time I am interested in what I am doing (c); Most of the time I am quite interested in what I am doing (d); and Most of the time I am fascinated by what I am doing (e). This measure was created by Seligman et al. (2005) to serve as a measure of happiness that might be particularly sensitive to upward changes in happiness. The items on this scale reflect three kinds of happy lives (the pleasant life, the engaged life and the meaningful life). Scores on this scale were found to be highly correlated with other measures of happiness and to have an internal consistency of α = .95 and a test-retest reliability of .97 over 1 week (Seligman et al., 2005). The measurements of satisfaction with life with the SHI are found to be reliable and can be broken down into two theoretically justified components (Kaczmarek et al., 2014). One component is attributable to the stable trait of satisfaction. The second component represents occasion-specific influences; the SHI provides the opportunity to measure unique aspect of situational well-being (Kaczmarek et al., 2014). In this study we have translated the measure by translating it into Swedish and then back into English to ensure that the measure would not change in any fundamental way. Future research will need to be undertaken to validate this measure on a Swedish sample.
Beck Depression Index-II (BDI-II)
The BDI-II is a widely used 21-item self-report inventory measuring the severity of depression in adolescents and adults. It was revised in 1996 to be more consistent with DSM-IV criteria for depression (Beck et al., 1996). It can be used to monitor therapeutic progress in both inpatient and outpatient settings. Each item includes a list of four statements arranged in increasing severity about a particular symptom of depression. For example, Item 1: Sadness, (0) I do not feel sad. (1) I feel sad (2) I am sad all the time and I can’t snap out of it. (3) I am so sad and unhappy that I can’t stand it. Psychometric properties of the Beck Depression Inventory-II as a self-report measure of depression in a variety of settings and populations has shown the internal consistency α = .92 for the clinical group and at α = .93 for the non-clinical group (Beck et al., 1996) and the retest reliability ranged from .73 to .96 (Wang & Gorenstein, 2013). Wang et al., concluded in their review that the BDI-II is a relevant psychometric instrument, showing high reliability, capacity to discriminate between depressed and non-depressed subjects, and can be viewed as a cost effective questionnaire for measuring the severity of depression, with broad applicability for research and clinical practice worldwide.
Beck Anxiety Index (BAI)
This 21-item inventory is designed to measure of anxiety. Psychometric properties of the Beck Anxiety Inventory, a self-report measure of anxiety, have shown the internal consistency around .92 and the retest reliability .75 (Beck et al., 1988).
The Behavioral Activation Scales (BAS)
The BAS is a 13-item measure of sensitivity to reward, assessing behavioral activation across three domains: drive, responsiveness, and fun seeking. This scale has demonstrated excellent reliability and convergent/discriminant validity (Carver & White, 1994).
Satisfaction With Life Scale (SWLS)
Five statements measuring global cognitive judgments of one’s life are given on which the person may agree or disagree using a 1 to 7 scale, with 1 = strongly disagree and 7 = strongly agree (Diener et al., 1985). For the purpose of trait measurement, the SWLS might be preferred to the SHI (Kaczmarek et al., 2014). Life satisfaction as assessed by the SWLS shows a degree of temporal stability (0.54 for 4 years), yet the SWLS has shown sufficient sensitivity to be potentially valuable to detect change in life satisfaction during the course of clinical intervention (Pavot & Diener, 2009). Further, the scale shows discriminant validity from emotional well-being measures. The SWLS is recommended as a complement to scales that focus on psychopathology or emotional well-being because in making a life satisfaction judgment, it emphasizes the person’s own standards of evaluation. The SWLS provides an adjunct to measures oriented toward the assessment of negative states. It assesses the positive side of the individual’s experience rather than focusing on unpleasant emotions or specific areas of life. The items appear to hold together in a unified factor (Pavot & Diener, 2009). The SWLS has shown strong internal reliability (.87, Diener et al., 1985). A Swedish translation of this measure was used (Linngård & Lorsell, 2012).
Brunnsviken Brief Quality of life scale (BBQ)
This inventory is developed as a measurement of subjective quality of life which is an important complement to symptom ratings in clinical research and practice. Six life areas (Leisure time, View on life, Creativity, Learning, Friends and Friendship, and View of self) were identified as important for overall quality of life and were included in the BBQ (Lindner et al., 2016). Results from a psychometric evaluation suggested a unifactorial structure, with good concurrent and convergent validity, high internal and test-retest reliability, and accurate classification ability. Psychometric properties in a Swedish sample show a test-retest reliability of .89. It has good just as good reliability and validity as the Quality of Life Inventory (QOLI), and good capacity to discriminate between a clinical and non-clinical subject (Frykheden, 2014).
Feedback Form
This form was created for this study to collect feedback from the patient on their experiences with the intervention. At the end of the treatment they were asked to rate satisfaction and acceptability with the intervention, and provide qualitative feedback regarding what they found most and least helpful, and any particular modifications they would recommend.
Statistical Analysis
Data were analyzed using visual inspection techniques (Barker et al., 2015). Data from the outcome measures were plotted graphically and assessed for level and change in slope across the study phases. Data were analyzed using bar chart presentations. Differences were computed/calculated for each participant for changes in each measures over time, and assessing cumulative percentage of change. A qualitative assessment was completed for each participant.
Further descriptive statistical analysis to assess changes in pre-, after, and follow up measures was conducted using a box plot method for graphically depicting groups of numerical data through their quartiles. This enabled an analysis of variability occurring outside the upper and lower quartiles.
To assess for magnitude in change further use of statistical measures was used. At group level Friedman’s Two-way Analysis of Variance was computed for each measure assessing the significance level (p < .05) of change, which is the appropriate test for within subject designs (Clark-Carter, 1997). Significance values were adjusted by the Bonferroni correction for multiple tests. Non parametric correlations were calculated using the Spearman rank-order correlation to assess the strength and direction of association between different measures (Clark-Carter, 1997). All statistical analyses were completed with IBM SPSS Statistics for Windows, Version 24.0.
Acceptability and feasibility of the intervention were examined using the participants’ ratings in a questionnaire where they provided qualitative feedback, and on recruitment and retention rates. The feedback was examined case by case.
Ethical Considerations
Informed consent was obtained and the study has been granted ethical approval. Risks for participating were considered being vulnerable in a group setting, putting time and effort in a treatment which is not evidence based, and becoming aware of deficits in positive emotion regulation skills as this is normally not assessed. Safety measures to try to diminish risks were put in place such as using a strict group protocol and discussion of rules to make the group setting as safe as possible, using only interventions that have some empirical support already, and letting participants volunteer to the study hence then assuming they are aware of the deficits studied. To eliminate acute risk factors patients with suicidal or homicidal ideations or a clinical condition requiring immediate treatment were excluded from the study. Should a participant deteriorate in mood during the treatment the standard protocol for the clinic is utilized, such as checking in with the person after the group session and putting in place safety measures such as scheduling a follow up appointment in the clinic or arranging a check-up with mobile health care team. Benefits of participating in the study are considered to be feeling affinity with other group members, participating in a treatment which increases awareness of mental health and personal strengths, can increase subjective wellbeing, being part of a development project in mental health might increase feelings that one’s own opinion matters. The benefits outweigh the risks. The ethics application (2019-06065) was approved. Declarations of interest: none.
Results
The final sample comprised of 10 participants. Participant ages ranged from 25 to 62 years (Mean = 41, 60, SD = 12,545). 100% were female, 90% Swedish and 10% other European descent. Participant characteristics are presented in Table 1.
Characteristics of Participants.
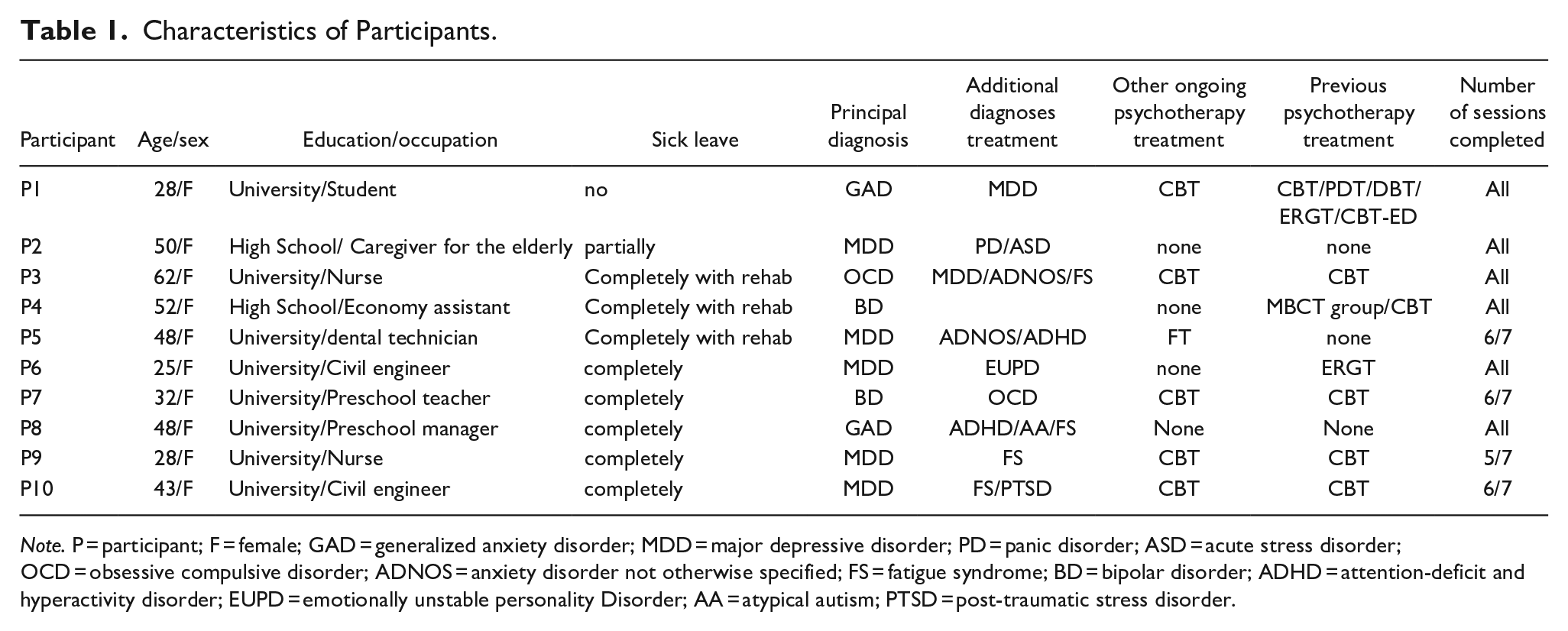
Note. P = participant; F = female; GAD = generalized anxiety disorder; MDD = major depressive disorder; PD = panic disorder; ASD = acute stress disorder; OCD = obsessive compulsive disorder; ADNOS = anxiety disorder not otherwise specified; FS = fatigue syndrome; BD = bipolar disorder; ADHD = attention-deficit and hyperactivity disorder; EUPD = emotionally unstable personality Disorder; AA = atypical autism; PTSD = post-traumatic stress disorder.
In terms of demographics, 80% had some college or university education, 90% were employed (although at the time of study 80% were on complete sick leave and 10% were partially on sick leave) and 10% were studying at university level (studying full time). Eighty percent were married or living with a partner, 70% had children.
Of the participants included in the study 40% had a principal diagnosis of major depressive disorder and an anxiety disorder (including, general anxiety disorder, panic syndrome, anxiety unspecified), 30% depression, 20% bipolar disorder, and 10% anxiety. All participants had a clinically significant level of depressive symptomatology (BDI-II; mean for sample = 33, 40; range 19–43). Eighty percent of the sample had levels of depression which fell in the severe range, scoring above 29 (Beck et al., 1996). Clinically significant levels of anxiety symptomatology (BAI; mean for sample = 27, 44; range 13–48; Beck et al., 1988) were present in all participants at the start of the treatment.
Their additional diagnoses showed some diversity, and included acute stress disorder (=1), obsessive compulsive disorder (=2), fatigue syndrome (=4), ADHD (=2), atypical autism (=1), emotional instability personality disorder (=1), post-traumatic stress disorder (=1) and a history of self-destructive behavior and suicidal ideation (=4).
Summary of Analyses of Individual Data
Six of the ten participants (P1, P2, P3, P7, P8, P10) showed changes in level and slope of their SBI scores from baseline to after the intervention consistent with a positive effect of the intervention on their positive emotion regulation skills (Figure 1). Three of the participants (P2, P3, P7) made additional gains after the intervention to follow up, and the remaining three maintained a substantial proportion of their gains at follow up. One participant (P6) showed a slight decrease in scores for SBI after the intervention. This appears as an adverse effect of the intervention on P6’s positive emotion regulation skills. Two participants (P5, P9) exhibited substantial changes after the intervention to follow up. P4 showed relative stability, slight increase in slope, but no clear change in slope. At follow up 80% had made positive gains on the SBI measure.
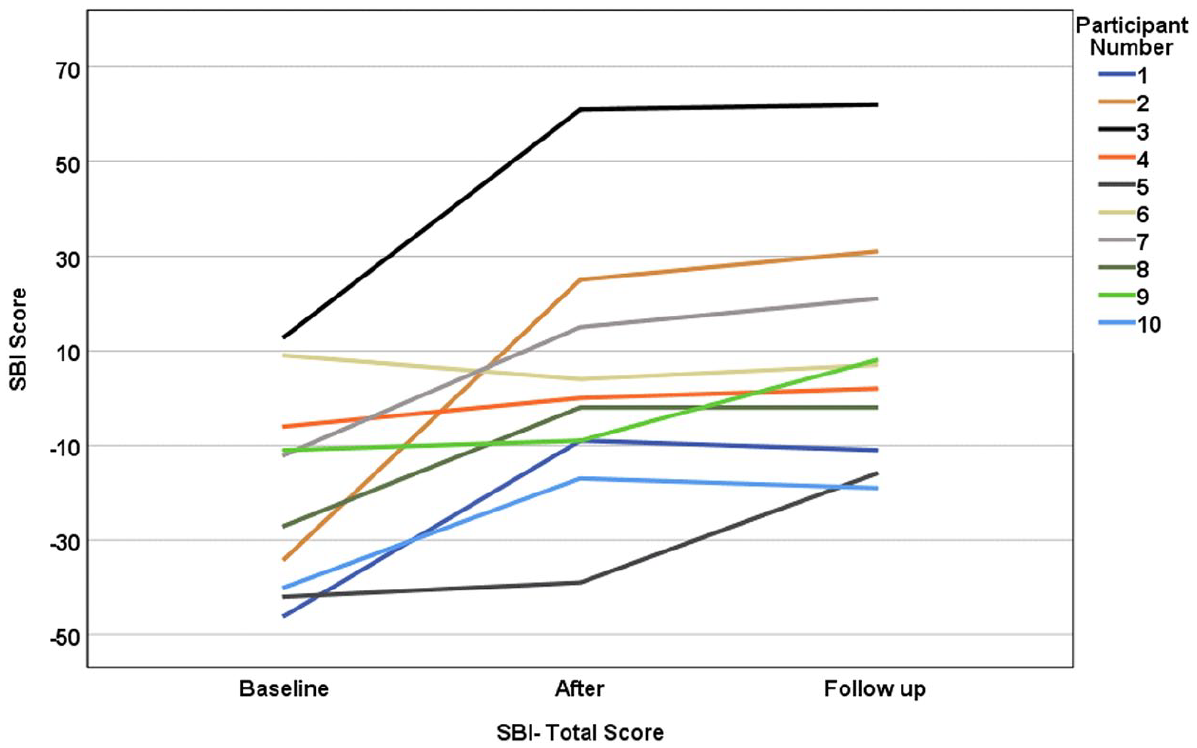
Savoring Beliefs Inventory (SBI) scores at baseline (week 1), after the intervention (week 6) and at follow up (week 14) for each participant.
Overall, participants’ anxiety (BAI) and depressive (BDI-II) symptoms decreased (Figures 2 and 3). At baseline eight participants (P1, P2, P3, P4, P5, P7, P8, P10) had severe levels of depressive symptoms (BDI-II > 29) which improved at follow up, then only one participant continued to be in this range (P7). At follow up five participants (P2, P3, P4, P8, P9) had depressive symptoms in the minimal to mild range (BDI-II < 20). For a visual representation of overall change please refer to Figure 3.
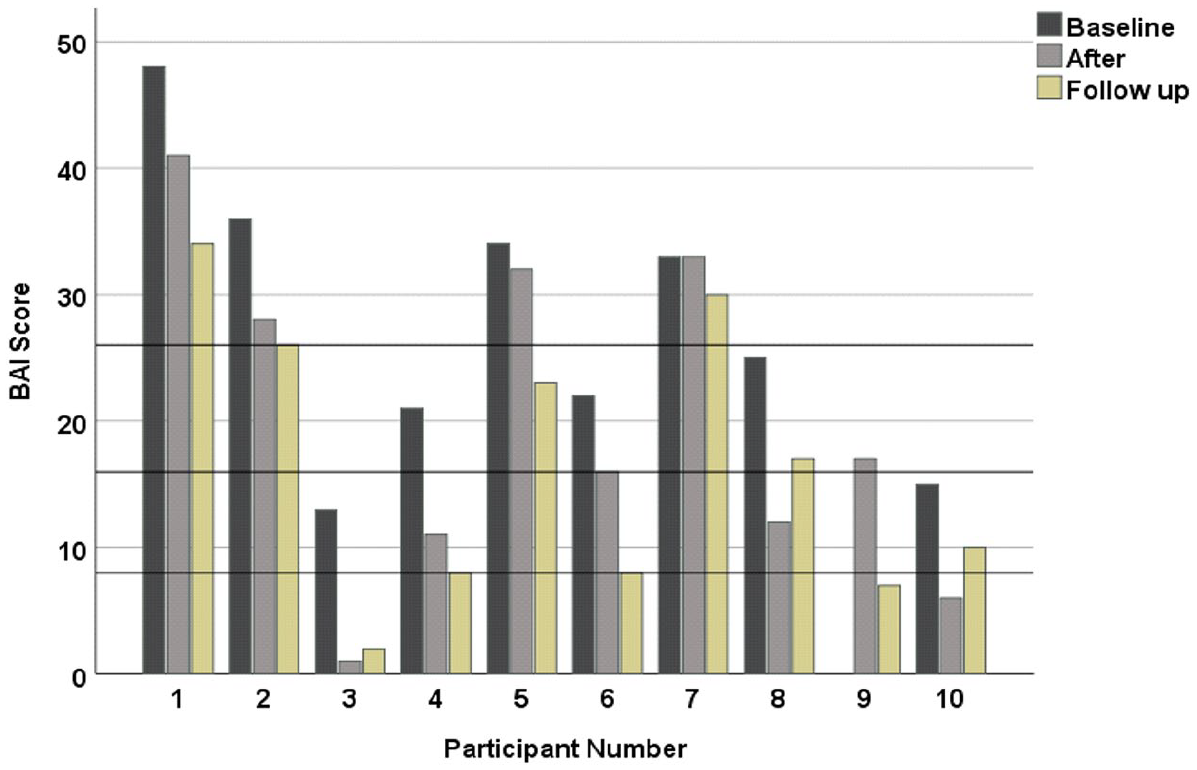
Beck Anxiety Index (BAI) scores at baseline (week 1), after the intervention (week 6) and at follow up (week 14) for each participant. BAI standardized cut off scores are outlined at 0–7 minimal; 8–15 mild; 16–26 modest; 26–63 severe.
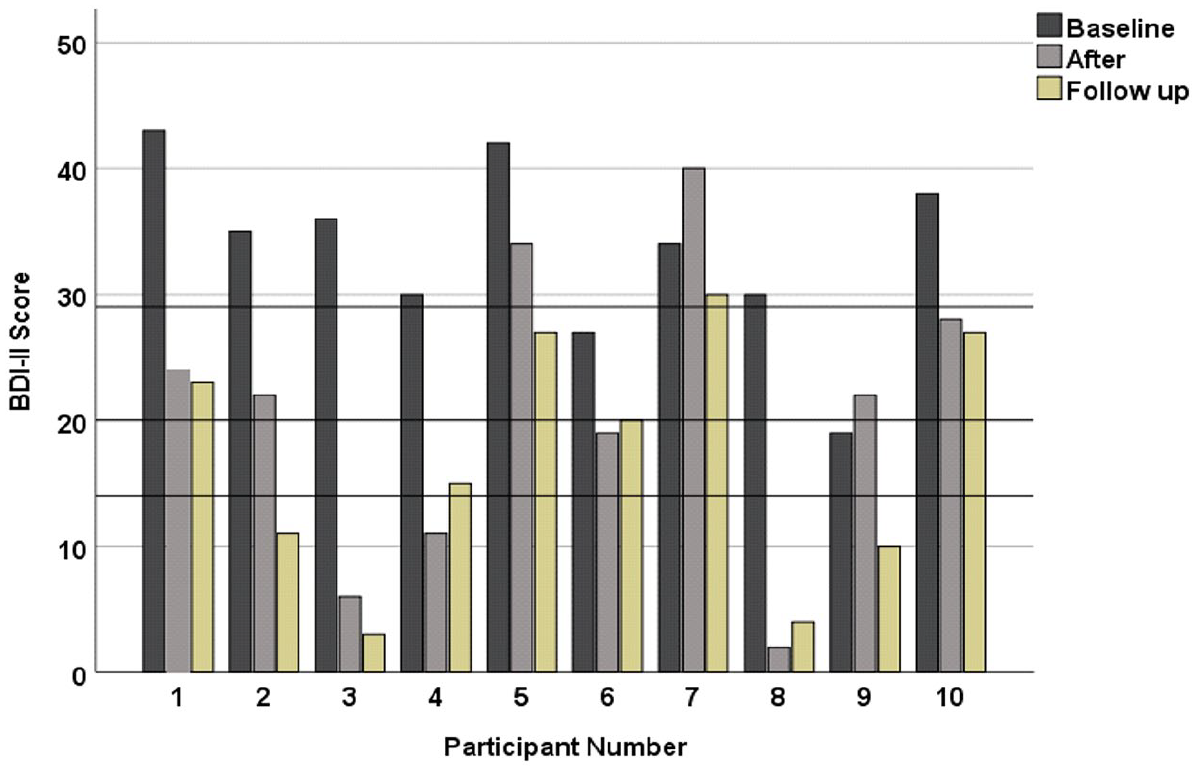
Beck Depression Index-II (BDI-II) scores at baseline (week 1), after the intervention (week 6) and at follow up (week 14) for each participant. BDI-II standardized cut off scores are outlined at 0–13 minimal; 14–19 mild; 20–28 modest; 29–63 severe.
On the questionnaire assessing qualitative feedback 8/10 participants found the intervention to be helpful and were satisfied, the remaining two reported finding some exercises difficult to grasp. Overall in the evaluation participants reported that most of the interventions were found to be helpful, in particular flow, scheduling positive activities, three good things, and setting emotional goals. Most participants found an area in their lives to continue working on to build and strengthen the positive emotion in that setting. Taken together these data suggest the intervention to have the potential to produce desired change in positive emotion regulation, and at the same time may not be effective for everyone.
Effects on Positive Emotion Regulation Skills (SBI)
SBI (total) scores improved from the baseline to after measure and continued to improve at the follow up measure. The difference from baseline to follow up was significant (.004). Analysis of the subscales show that anticipatory emotional regulation skills improved significant after the intervention (.022) and continued to improve at the follow up (.001). Savoring improved significantly (0.022) from baseline to follow up. No significant changes were found for reminiscing skills.
Happiness Ratings (SHI)
Happiness ratings improved over time. Results show a significant change from baseline to follow up (.016).
Effects on Drive, Responsiveness, and Fun Seeking (BAS)
Drive and responsiveness ratings improved. Significant change was observed from baseline to follow up for drive (.018) and responsiveness (.042). No statistically significant change was observed on the fun seeking measurement.
Effects on Quality of Life and Well-being
Ratings on BBQ and SWLS increase over time. Results show a significant increase in BBQ scores (.005) after the intervention which was maintained at follow up (baseline to follow up .011). Subjective well-being ratings (SWLS) improved significantly from baseline to follow up (.030).
Effects of Anxiety (BAI) and Depressive (BDI-II) Symptoms
Descriptive data for changes in symptoms of anxiety and depression are presented in Figures 4 and 5. Depressive symptoms (BDI-II) improved after the intervention and the change from baseline to follow up was significant (.002) Anxiety symptoms (BAI) significantly improved (.029) after the intervention and the results were maintained at follow up.
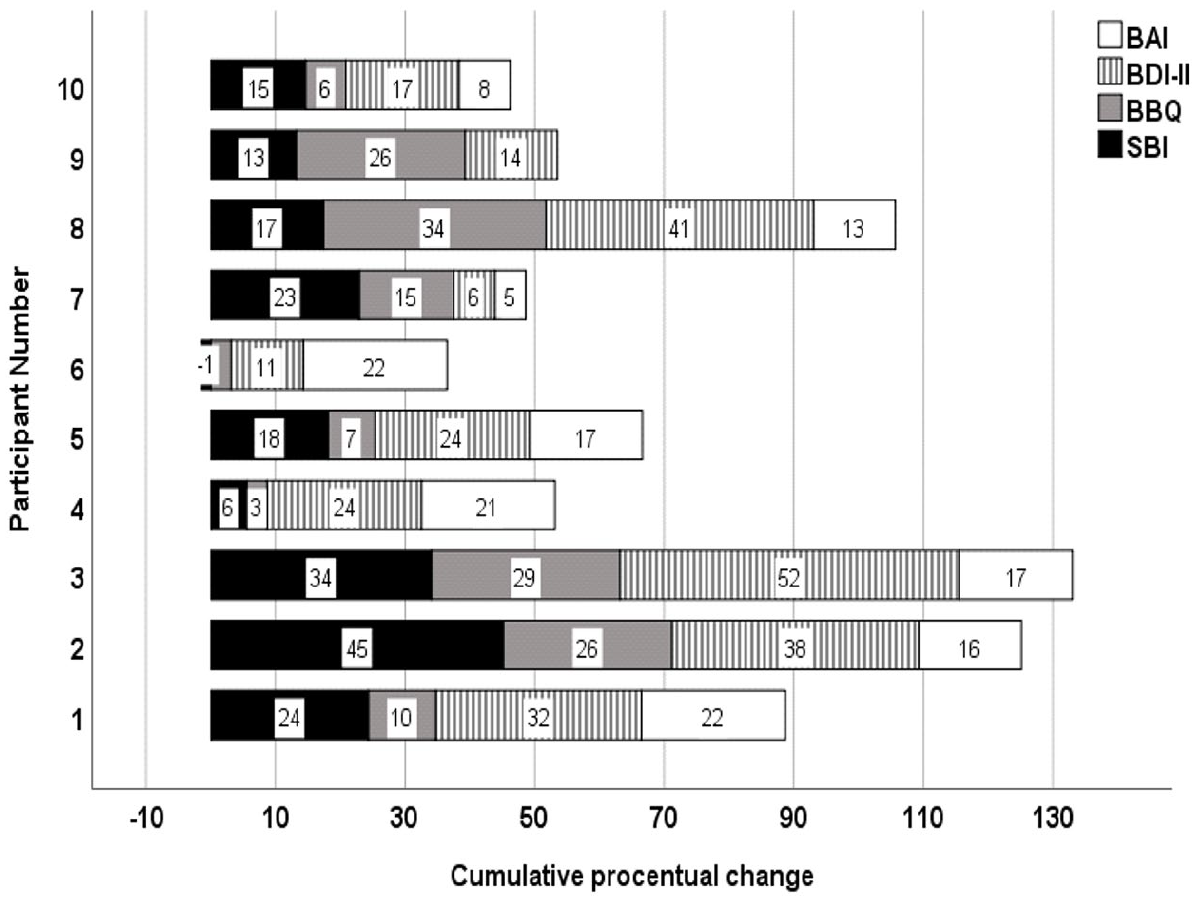
The cumulative percentage change is depicted for each participant adding the percentage changes of the following measures; Beck Anxiety Index (BAI), Beck Depression Index-II (BDI-II), Brunnsviken Brief Quality of life scale (BBQ), Savoring Beliefs Inventory (SBI).
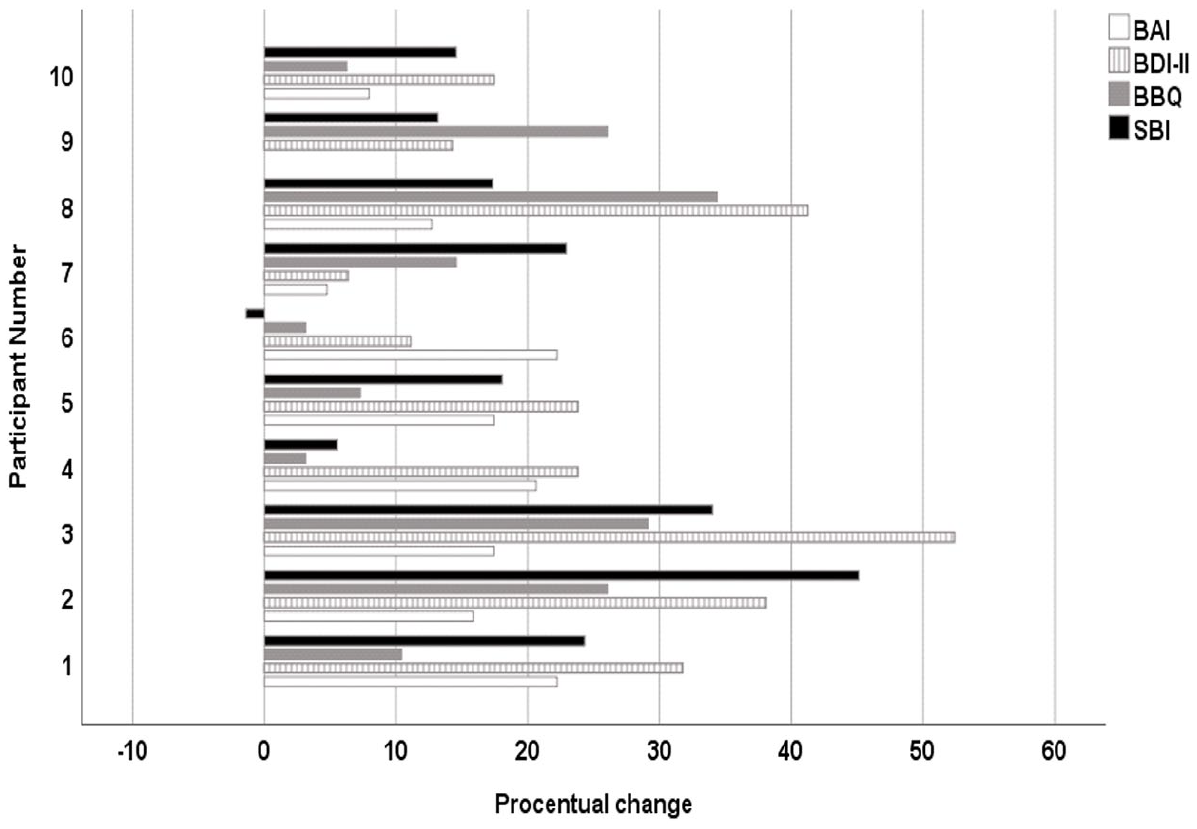
For a percentage comparison for change on the different scales Beck Anxiety Index (BAI), Beck Depression Index-II (BDI-II), Brunnsviken Brief Quality of life scale (BBQ), Savoring Beliefs Inventory (SBI), the increase in percent on each measure was computed for each participant.
Are Improvements in Positive Emotion Regulation Skills (SBI) Associated With Beneficial Changes in Other Measures?
Spearman’s rho correlation coefficient was used to assess the relationship between positive emotion regulation skills (SBI) and other measures. The following correlations were found between SBI and BDI-II (p = .565), SBI and BBQ (p = .591), and SBI and SWLS (p = .482). Please refer to Figure 5 for a visual presentation to display percentage change in measures to facilitate some form of comparison.
External Events Influencing Outcome
The feedback from participants in this study on their thoughts about the Covid-19 pandemic was in general that they found the intervention helpful in providing a specific focus on building personal strengths in this time of world crisis.
Discussion
Preliminary results across participants show significant improvements from baseline to follow-up in positive emotion regulating skills, in particular savoring and anticipation, happiness, drive and reward responsiveness, anxiety and depressive symptoms, and quality of life. Anticipatory skills and quality of life showed improvement from baseline to after the treatment intervention and this continued to improve at follow up. The changes in positive emotion regulation skills correlated with decreased depressive symptoms and increased life quality ratings.
The drop in symptoms of depression (BDI-II) and anxiety (BAI) were significant. In the behavioral activation treatment for depression (BA) pleasant activities scheduling is presumed to have beneficial gains. BA continues to be an effective treatment for depression (Ekers et al., 2014). This is in some ways similar to this treatment in that participants are actively taught to seek out situations and activities that enable and stimulate positive emotion with the difference in approach being that the focus in this intervention is on trying to enhance the positive emotion by thinking in a different way or changing something in the situation to make it more pleasant instead of scheduling and increasing the frequency of pleasant activities per se. CBT is by far the most consistently empirically supported psychotherapeutic option in the treatment of anxiety disorders (Otte, 2011).
The building resilience treatment program differs from standard CBT in that no direct focus on anxiety symptoms is undertaken and it does not work on confronting situations where anxiety is felt. Participants are encouraged to widen their experience, to go out and meet people and do things but in the context of seeking out the possibility to feel positive emotion contrary to learning how to challenge and combat anxiety. Possibly, it may be that the focus on regulating positive emotion and increasing it and seeking it out can have the same effect on decreasing anxiety and depressive symptoms as the traditional therapy approach. 6 participants (P1, P3, P4, P7, P9, P10) had previously received treatment with CBT. The clinical psychologist giving the treatment has many years of clinical experience of working with CBT. Hence some pre-understanding on treating anxiety and depression is present both with participants and clinician. In the study by Carl (2015) the participants made gains after having received a full course of CBT. The findings could be taken that this intervention provides support for the additional value of the intervention.
The feasibility and acceptability of the intervention were supported by the high rate of recruitment (88 %) and positive qualitative feedback on the helpfulness and utility for the intervention. The retention rate (67%) was not as high as hoped for. The emergence of the world pandemic Covid-19 occurred at the start of the research project. The reason for leaving the study was in three cases directly linked to the Covid-19 pandemic, two having flu like symptoms early on and one participant electing not to participate in a group treatment setting during a pandemic. The other two participants dropped out due to personal issues. The retention rate but also the attendance rate for this study will have been adversely affected by the Covid-19 world pandemic. The pandemic resulted in very strict rules about not being permitted to attend the clinic if any symptom of un-wellness were felt, thus resulting in a higher than normal clinic wide rate of appointments being cancelled.
Although the world pandemic crisis had adverse effects on the ability for participants to attend some sessions, and for some to complete the project, it could possibly have had a positive effect on the participants’ attention to homework tasks and desire to focus on the skills being trained, providing them with a focus during an ongoing world crisis. Focus on building skills and personal strengths can possibly be useful in which this provides a person with a sense of direction and control during ongoing disconcerting world events.
Other research performed concurrently as this study have found similar support for the effect of positive psychology interventions (PPIs). A meta-analysis (Geerling et al., 2020) on the effects of PPIs on well-being and psychopathology in patients’ with severe mental illness did not find PPIs more effective in comparison with other active interventions, although they did find that people benefited from PPIs in terms of well-being and mental health, and had good impact on Major Depressive Disorder. The control groups in the studies were CBT, cognitive therapy, and mindfulness. These findings support the pleas for a more balanced approach in clinical psychology and are in line with the findings in this study. A network analysis (Blanco et al., 2020) exploring topography of changes in psychological elements after a 10 week group treatment of either PPI or CBT, showed a significant change in the reorganization of psychological variables after therapy for the patients who received PPI. Both treatments were effective although the effect size was greater for those receiving PPI. Depression symptoms were positively associated with difficulties in emotion regulation prior to the intervention but this changed after the intervention. Positive affect (hedonic components) and well-being (eudemonic components) emerged as the bridge nodes suggesting an interesting change in the structure connecting both the negative and positive communities after the intervention indicating a more balanced recovery, not only less symptoms but also more wellbeing. Integrative Positive Psychological Intervention for Depression (IPPI-D) compared to CBT might be the optimal treatment for depressed patients with high levels of negative automatic thoughts (Lopez-Gomez et al., 2019). Clinician led positive psychology interventions seem to be effective at reducing medical patient anxiety (Brown et al., 2019).
To engage with challenge and discomfort has great potential for growth, healing, and insight (e.g., Ivitzan et al., 2016; Masten, 2014; Seligman, 2011; Vaillant, 2000). The importance of the dialectics of emotion, in order to grow and develop, is reported in several studies and theories (e.g., Ivitzan et al., 2016; Vaillant, 2000). Depression needs to be characterized not only by the presence of negative emotions and cognitions but also by difficulties in experiencing or maintaining positive emotional states (Watson & Nargaon-Gainey, 2010). Mental health services need to offer the same dialects in its approach to treating mental illness by also having focus on functional recovery and building wellness and strengths systematically. There is growing evidence that including PPIs have the potential to increase the effects on mental health (e.g., Geerling et al., 2020; Seligman et al., 2005).
Study Limitations and Directions for Future Research
This study was an open clinical trial with only one treatment. An open clinical exploratory trial was made as a first step to demonstrate if a gross effect exists at all. A strength with this design is to be able to look in depth at the individual studied and each participant serves as its own control. The weakness with this design is not being able to establish typicality’s or general laws (Barker et al., 2015). A clinical replication study with a more sophisticated design will be needed for subsequent studies with control of comparison groups to estimate net effects of possible confounding variables. Threats to internal validity of the current design include changes within the individual and spontaneous recovery, remission, interfering events, and significant events (e.g., Covid-19 pandemic). The participants volunteered to participate and were very interested in the intervention as such, expectancy effect could be a cause for improvement. Another limitation to the generalisability of the results is that 100% participants were female.
A further study using a single case experimental design with a multiple baseline could determine the initial stable expression (i.e., baseline) and then the participants are randomized to the period to when the manipulation (i.e., treatment intervention) is applied. In successively administering a manipulation to different behaviors after initial behaviors have been recorded, a multiple baseline design allows for inferences about the effect of the intervention. This design would be easy to implement in a clinical setting.
In the future a control group, and increasing randomization to the study such as asking staff to assist with finding participants and recommend potential participation in the study to a greater extent could rule out some of the design flaws in the present study. To be able to generalize beyond the individual studied a clinical replications study will need to be undertaken with a larger sample and a control group.
Many of the primary studies on the effectiveness of PPIs have used a small sample size (White et al., 2019). Taken this into account small but significant effects have been found but future research needs to increase sample size, also research needs to employ strategies to increase effectiveness of the PPIs.
Future research will be needed to confirm the validity of these findings and research into who benefits from which treatment the best to help tailor treatment to fit the individual’s needs.
Conclusions
The outcome data from this study suggest that this intervention can have beneficial effects across individuals wanting to participate in the group with a principal diagnosis of an anxiety disorder and/or unipolar depression as well as having comorbid emotional disorders. The present results support the notion that focusing on positive emotion processes may have the potential to have beneficial changes to quality of life, well-being and reduce clinical symptoms of anxiety and depression. It further supports the potential utility of incorporating this intervention into the treatment of emotional disorders to help reduce symptoms of anxiety and depression but also to increase overall mental health.
Individual differences in response to the intervention did not appear to be due to age, principal or comorbid diagnostic status. The sample is quite small to draw firm conclusions. It is notable that there was a variation in diagnoses in the participants responding to the treatment and this suggests the intervention can have beneficial effect for individuals with a number of different principal and comorbid emotional disorders, similar findings are reported elsewhere (e.g., Carl, 2015).
Footnotes
Acknowledgements
Thank you to the participants in the study and also to all the staff at the adult mental health outpatient unit Department of Psychiatry and Rehabilitation, Region Jönköping, Sweden.
Author’s Note
The authors are solely responsible for the content and writing of this paper.
Data Availability Statement
All data generated or analysed during this study are included in this published article. Additional data are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided for the ethical application FUTURUM-932830 and for research time FUTURUM-937250, Region Jönköping County, Sweden.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.