
Abstract
In the last decade, Child and Adolescent Mental Health Services (CAMHS) have observed an unprecedented rise in young children presenting with suicidal ideation, needing urgent assessment and treatment. Once stabilised, CAMHS professionals often refer these children to speech and language therapists (SLTs) for assessment of and support for their social-emotional skills. The Secret Agent Society (SAS) is an evidence-based intervention for children with significant emotional regulation and social communication challenges. No published peer-reviewed evidence exists for the use of SAS for children with moderate-severe mental health disorders. This study aimed to evaluate the efficacy of SAS in an Irish outpatient CAMHS. Fifty-one children (30 boys, 21 girls) aged 8–12 years (mean age 10:11) with diagnoses of attention deficit hyperactivity disorder, anxiety disorder and/or autism attended the 14-week programme. Questionnaires were completed by children, their parents (51 mothers, 45 fathers) and teachers pre-intervention, post-intervention and at 3- and 6-month follow-up. Statistically significant improvements were made in children's social communication (F (1.985, 99.273) = 24.900, p < 0.001) and emotional regulation (F (1.787, 89.358) = 27.302, p < 0.001) across home and school settings. Children's knowledge of emotional regulation strategies also significantly improved. Treatment gains were maintained up to 6-months post-intervention. Results provide preliminary evidence for the efficacy of SAS in an Irish outpatient CAMHS. A cost–benefit analysis would determine the feasibility of offering SAS in other outpatient community services. SLTs have a vital role to play in delivering intensive social-emotional skills support for children with complex diagnostic profiles within CAMHS and other specialised multi-disciplinary teams.
Introduction
Located in the community and staffed by multidisciplinary teams, Irish Child and Adolescent Mental Health Services (CAMHS) offer assessment and treatment to young people with moderate-severe and enduring mental health disorders up to the age of 18 years (McNicholas, 2018). In the last decade, there has been a significant increase in the number of children referred to CAMHS in the Republic of Ireland and in the UK. Between 2012 and 2018, there was a 24% increase in the number of referrals accepted by Irish mental health services (Ryan, 2019). Escalating numbers of children presenting with mental health disorders have led to a substantial rise in demand for psychiatric care, with many mental health services experiencing an additional increase in the complexity of presenting disorders (RCSLT, 2022). The Covid-19 pandemic has also had an adverse impact. Referrals to UK CAMHS in September 2020 were reportedly 72% higher than in September 2019 (Longfield, 2021). Furthermore, Irish CAMHS teams have observed a rise in children under 12 years presenting with suicidal thoughts and behaviours, needing urgent assessment and treatment (Maguire et al., 2020).
The prevalence and nature of speech, language and communication difficulties among children with mental health disorders is well established (Botting et al., 2016; Cohen et al., 2013). Children with language or communication impairments are at greater risk of developing a mental health disorder, most commonly anxiety or depression (Botting et al., 2016). Up to 80% of children with mental health concerns experience language or communication difficulties, many of which are left unrecognised and untreated (Hollo et al., 2014). Even when recognised, the interaction between communication difficulties and mental health problems is highly complex and young people can present in very different ways (Conti-Ramsden et al., 2018).
In Ireland, speech and language therapists (SLTs) are core members of most community CAMHS teams. One aspect of the SLT's role in CAMHS is the provision of specialised input for children and young people with communication difficulties, such as those associated with attention deficit hyperactivity disorder (ADHD), anxiety disorder (AD) and autism. Children with these diagnoses may experience problems with social communication (Laugeson, 2022). Social communication difficulties can exacerbate mental health difficulties, as positive social relationships generally act as a buffer against mental health disorders (Perry and Szalavitz, 2017). Additionally, social communication impairments can result in children being rejected or victimised by their peers (Moore et al., 2017), with peer rejection being one of the strongest indicators of mental health problems (Laugeson, 2022).
Many children with communication and mental health disorders also experience difficulty with emotional literacy and social problem-solving skills (Rieffe and Wiefferink, 2017; Van Den Bedem et al., 2018a), leading to difficulties with emotional regulation. Maguire et al. (2020) examined case notes of 318 children referred to CAMHS Liaison Services in a Dublin hospital over a 10-year period (2009–2018). Analysis showed that the primary reason for referral was emotional dysregulation. Suicidal thoughts were reported in over half of the children's presentations, whereas suicidal behaviours occurred in almost one-quarter. All of these children were aged 12 years and under.
Heightened levels of emotional dysregulation may influence social functioning, particularly in those with neurodivergence (Mazefsky, 2015). Children who can identify their own emotions and the emotions of others tend to find it easier to interact socially and experience less anxiety (Denham et al., 2012). Indeed, social communication and emotional regulation are inextricably linked and may be considered ‘bidirectional’ (White et al., 2013). For example, anxiety disorders in children can result in clinically significant social impairments which interfere with social functioning (APA, 2013). Similarly, social communication difficulties can contribute to heightened anxiety (Kleinhans et al., 2010). This complex interplay complicates clinical service provision for SLTs, as emotional regulation difficulties can directly undermine the potential benefits of communication intervention, particularly in therapies with a social focus (White et al., 2013). Unfortunately, without effective intervention, social and emotional challenges may worsen as children grow older (Rubin et al., 2009). Yet evidence-based intervention programmes with a dual focus on both emotional regulation and social communication are limited, particularly at primary school level (White et al., 2013). Existing therapies tend to focus solely on emotional regulation (e.g. ‘zones of regulation’ Kuypers, 2011) or social communication (e.g. ‘social thinking’ Garcia Winner, 2014) but rarely both (Beaumont et al., 2019).
The Secret Agent Society (SAS) is an evidence-based, multimedia therapy programme for primary school children that targets social communication as well as emotional regulation (Beaumont and Sofronoff, 2008). Based on the principles of cognitive behaviour therapy (CBT), SAS teaches children how to identify and cope with their emotions and how to understand and manage social interaction. It combines various therapeutic modalities including weekly clinic sessions for children, parent and teacher training, computer game access and home/school activities. SAS was originally developed for children with autism and has a robust published evidence base for this client group. Effectiveness has been investigated in mainstream schools (Beaumont et al., 2015), on an individual basis (Tan et al., 2015; Thomson et al., 2015), remotely via Skype/phone (Beaumont et al., 2021; Sofronoff et al., 2015), in specialist autism classes (Enfield et al., 2017) and in hospital and university clinics (Beaumont et al., 2019) in Australia, America and Canada. Sauvé et al. (2018) adapted the SAS programme for 24 children (aged 8–13) attending a ‘specialty mental health clinic’ in California. The cohort of children all had a primary diagnosis of autism. In fact, most SAS research has focused on children with this condition (e.g. Beaumont et al., 2021; Weiss et al., 2018). No published peer-reviewed evidence currently exists for the use of SAS for children with complex mental health diagnoses attending community CAMHS.
SAS was developed by a clinical psychologist and most prior research describes the programme's implementation by clinical psychologists (e.g. Beaumont et al., 2019; Sofronoff et al., 2015). Teachers and occupational therapists have also been involved in published SAS research (Enfield et al., 2017; Sauve et al., 2018). No published SAS studies cite facilitation by SLTs. In the past, CBT interventions were typically offered by professionals trained in psychiatry and/or clinical psychology. However, in recent times there has been a move to training allied health professionals to deliver CBT, including SLTs (Deary et al., 2018). Research shows that SLTs have used CBT-informed interventions successfully to support those with functional dysphonia (Deary et al., 2018), dysphagia (Patterson et al., 2018) and stammering (Ansari et al., 2013). In fact, Deary et al. (2018: 11) stated it is ‘a necessity’ to train SLTs to use CBT when working with emotional disorders.
Following training in the SAS programme, authors piloted the intervention with 21 children to evaluate its suitability within two CAMHS clinics. Encouraging outcomes were achieved in relation to children's social communication and emotional regulation and prompted a more in-depth exploration. The authors sought to extend previous SAS research by exploring its effectiveness for primary school children with moderate-severe mental health disorders, using senior SLTs as facilitators.
Aims
To determine if the SAS programme led to improvements up to 6-months post-intervention in children's (a) social communication skills at home and at school; (b) emotional regulation skills at home and at school and (c) theoretical knowledge of anxiety and anger management strategies.
Method
Ethical permissions
Saint John of God Research Ethics Committee granted ethical approval for the study.
Study design
This was an exploratory intervention study. Data was collected between August 2017 and December 2018.
Study setting and participant recruitment
Three separate SAS programmes were delivered concurrently across three CAMHS clinics. Clinics were located in geographically distinct regions in the East of Ireland, encompassing both urban and rural areas. Each clinic was comprised of a multi-disciplinary team led by a Consultant Child and Adolescent Psychiatrist.
Purposive sampling was used to obtain participants. Three Consultant Child and Adolescent Psychiatrists working in each of the CAMHS clinics acted as gatekeepers in the recruitment process. They provided families who met inclusion/exclusion criteria with a participant information leaflet.
Inclusion criteria
Children with a moderate-severe mental health disorder (that which significantly impacts daily functioning across a number of settings) as confirmed by their Consultant Child and Adolescent Psychiatrist. Children were also required to have clinically significant social communication and emotional regulation difficulties.
Children aged between 8 and 12 years.
Children attending mainstream school, with average or above average intellectual ability, as measured by school reports or cognitive assessments.
Exclusion criteria
Children whose language skills fell significantly below the average range, to ensure they could fully understand programme content. This is in line with the programme developer's recommendation that children's language skills should be at least equivalent to that of an 8-year-old (Beaumont et al., 2019).
Children with oppositional behavioural disorders who may not have been amenable to group participation.
Children unable to communicate fluently through English.
Families who wished to partake in the study contacted their Consultant Psychiatrist. Following this, further information was given to each family and an interval of 7 days was provided prior to seeking consent. Gatekeepers then sent consent and assent forms along with a stamped addressed envelope to participants. When forms were returned, researchers contacted parents directly.
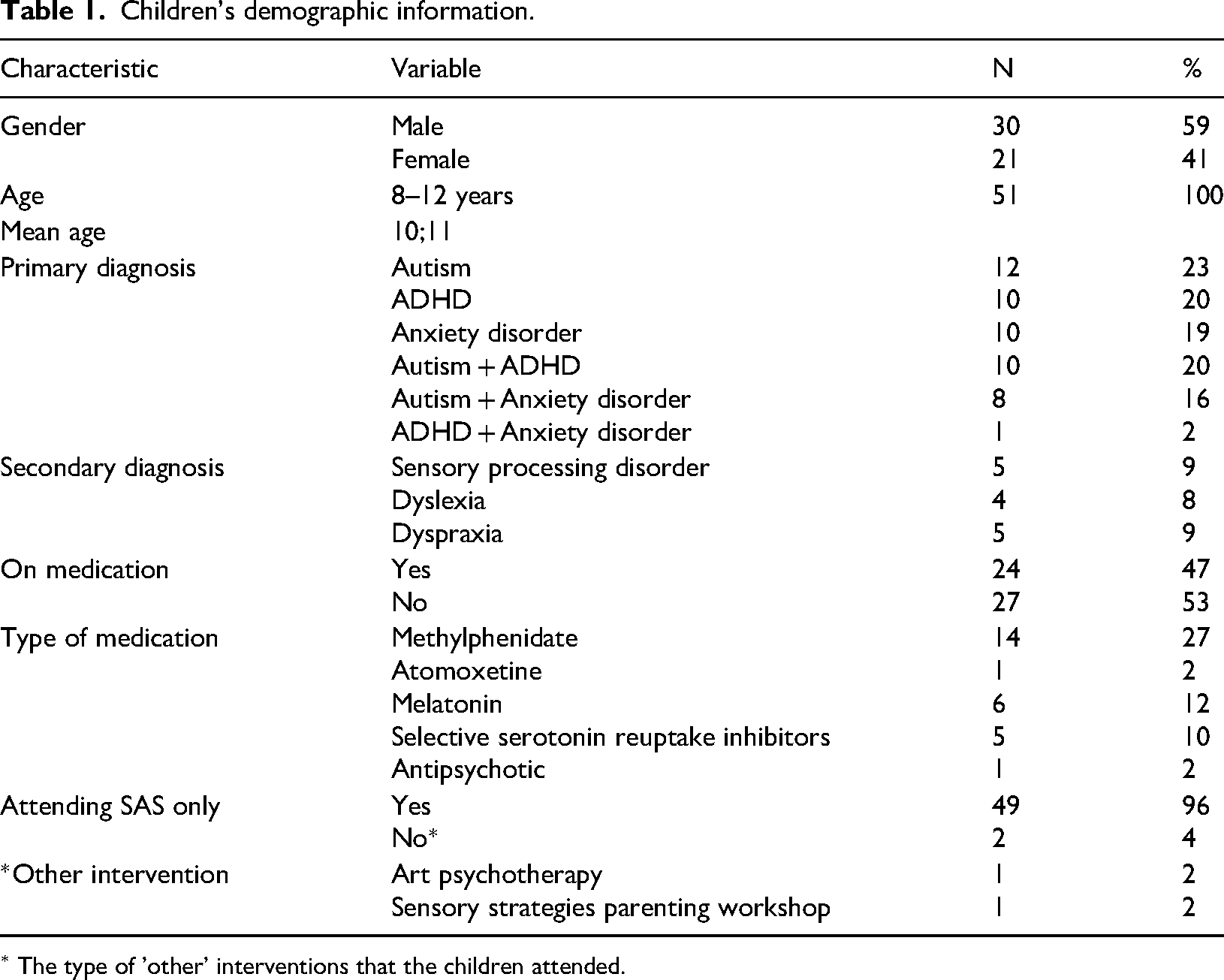
The study comprised 198 participants; 51 children (males n = 30, females n = 21), their parents (mothers n = 51, fathers n = 45) and teachers (n = 51). Children's mean age was 10 years and 11 months. Their demographic information is outlined in Table 1. Children's primary diagnoses comprised ADHD, AD, autism or a combination. Secondary diagnoses included sensory processing disorder, dyslexia and dyspraxia. Children were all Caucasian, born in Ireland and spoke English as their primary language. One child was bilingual
Children's demographic information.
Children's demographic information.
∗ The type of 'other' interventions that the children attended.
At the time of recruitment, 24 of the children (47%) were in receipt of medication relating to their mental health disorder. Five children were in receipt of more than one prescribed medication. One child commenced medication (methylphenidate) following the seventh session. Two participants received additional therapeutic support over the intervention period (art psychotherapy and a sensory strategies parent workshop). All 51 children completed the programme.
Outcome measures were completed by parents, teachers and children at four discrete timepoints; 2 weeks pre-intervention (during the parent and child interview), post-intervention (during or directly following Child Session 9), 3 months later and 6 months later (Figure 1).
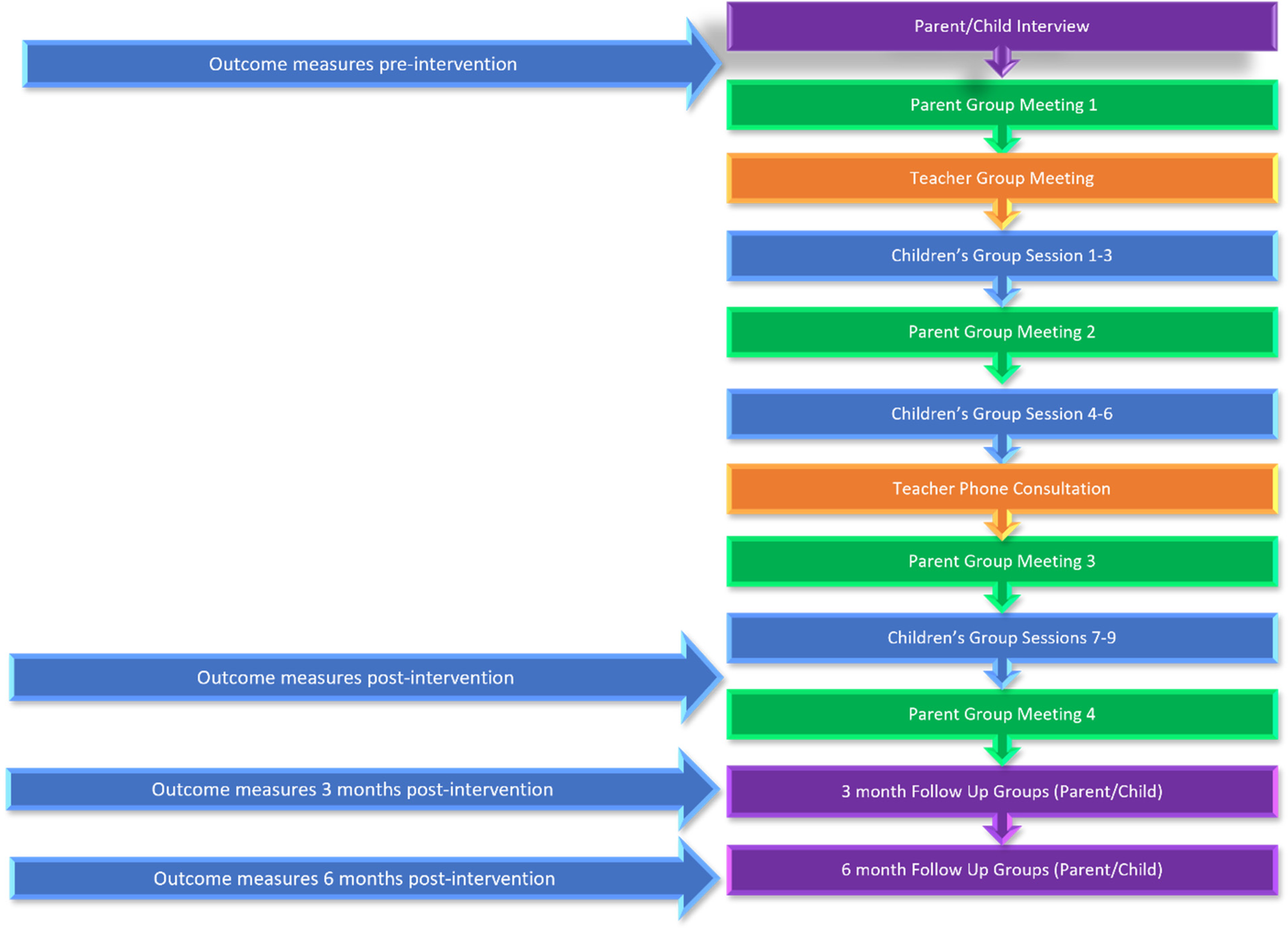
Outcome measure timepoints.
(i) Social Skills Questionnaire (SSQ: Spence, 1995)
The SSQ is a broad measure of children's social communication skills that has parent (SSQ-P) and teacher versions (SSQ-T). It has been used with multiple client groups, including those with depression (Spence et al., 2016), social anxiety (Spence et al., 2017) and autism (Beaumont et al., 2021). The SSQ has good internal consistency and has been shown to be reliable and valid (Spence, 1995). Respondents are asked to indicate how accurately each of 30 statements describes the child's social behaviour over the past 4 weeks (e.g. ‘stands up for him/herself appropriately’, ‘shares things with other kids’) using a 3-point scale. Response options are 0 (‘not true’), 1 (‘sometimes true’) or 2 (‘mostly true’). Total scores range from 0 to 60. A higher score indicates greater social communication competence.
(ii) Emotion Regulation and Social Skills Questionnaire (ERSSQ: Beaumont and Sofronoff, 2008) (iii) Programme Satisfaction Questionnaire (PSQ)
The ERSSQ parent version (ERSSQ-P) and teacher version (ERSSQ-T) were designed to evaluate children's competency in the specific emotion recognition, emotional regulation and social communication skills targeted by the SAS programme. Respondents are asked to rate how often the child engages in 27 behaviours on a 5-point scale (e.g. ‘controls his/her anger effectively’, ‘copes effectively when he/she makes a mistake’). Responses range from 0 to 4, using the options ‘never’ (0), ‘rarely’ (1), ‘sometimes’ (2), ‘often’ (3) and ‘always’ (4). Scores range from 0 to 100, with higher scores reflecting greater levels of ability. Both ERSSQ measures have been shown to have good psychometric properties and concurrent validity (r = .86) with the SSQ (Butterworth et al., 2013).
The PSQ was developed by Beaumont and Sofronoff (2008) to gather quantitative and qualitative data about the programme. It was administered to parents and teachers at the 6-month timepoint. Quantitative findings from the PSQ are reported on in the results section. Qualitative data gathered will be reported on in future publications.
Child outcome measures
These were completed individually with each child 2 weeks pre-intervention (during the parent and child interview), post-intervention (Child Session 9), 3 months later and 6 months later, using the same assessment process at each timepoint. Two stories were read aloud to each child and responses transcribed verbatim. Higher scores reflect greater knowledge of strategies for coping with anxiety and anger. Both child measures have been used in previous CBT-informed research (e.g. Beaumont and Sofronoff, 2008; Sofronoff et al., 2005).
(i) James and the Maths Test (Attwood, 2004a) (ii) Dylan is being Teased (Attwood, 2004b)
This measure assesses children's knowledge of anxiety management strategies. It involves a story about a boy, James, who feels anxious about a maths test. After the story, the child is asked ‘what could James do and think to feel less anxious?’ One point is awarded for each strategy suggested. For a strategy to receive 1 point, it must be appropriate in both content and context. For example, the response ‘study for the test’ would be appropriate, but ‘cheat on the test’ would not. Strategies must be specific (e.g. ‘take deep breaths’, ‘play with a fidget toy’), rather than vague (e.g. ‘just do the work’, ‘don’t worry’).
This measure assesses children's knowledge of anger management strategies. The child is asked to generate ideas for how a boy, Dylan, can effectively cope with anger and bullying, using the question ‘what could you do and say to help Dylan stay calm and not get mad with them?’ One point is awarded for each strategy suggested. Strategies must be specific and acceptable means of coping with anger and bullying. For example, responses such as ‘get them expelled’ or ‘bribe them’ would score 0, whereas ‘talk in a firm voice’ or ‘tell the teacher’, would score 1.
Programme content
The intervention consisted of the following core components:
Parent interview: This was completed with a researcher to gather information on the nature and duration of the child's social-emotional difficulties, as well as the child's strengths and areas of interest. Consent was obtained to send an information leaflet and consent form to the child's teacher. Pre-intervention outcome measures were also completed.
Child interview: This was completed after the parent interview with the child's parent present. The purpose was to inform the child of the SAS group, meet one researcher and ask questions. Pre-intervention outcomes measures were also administered.
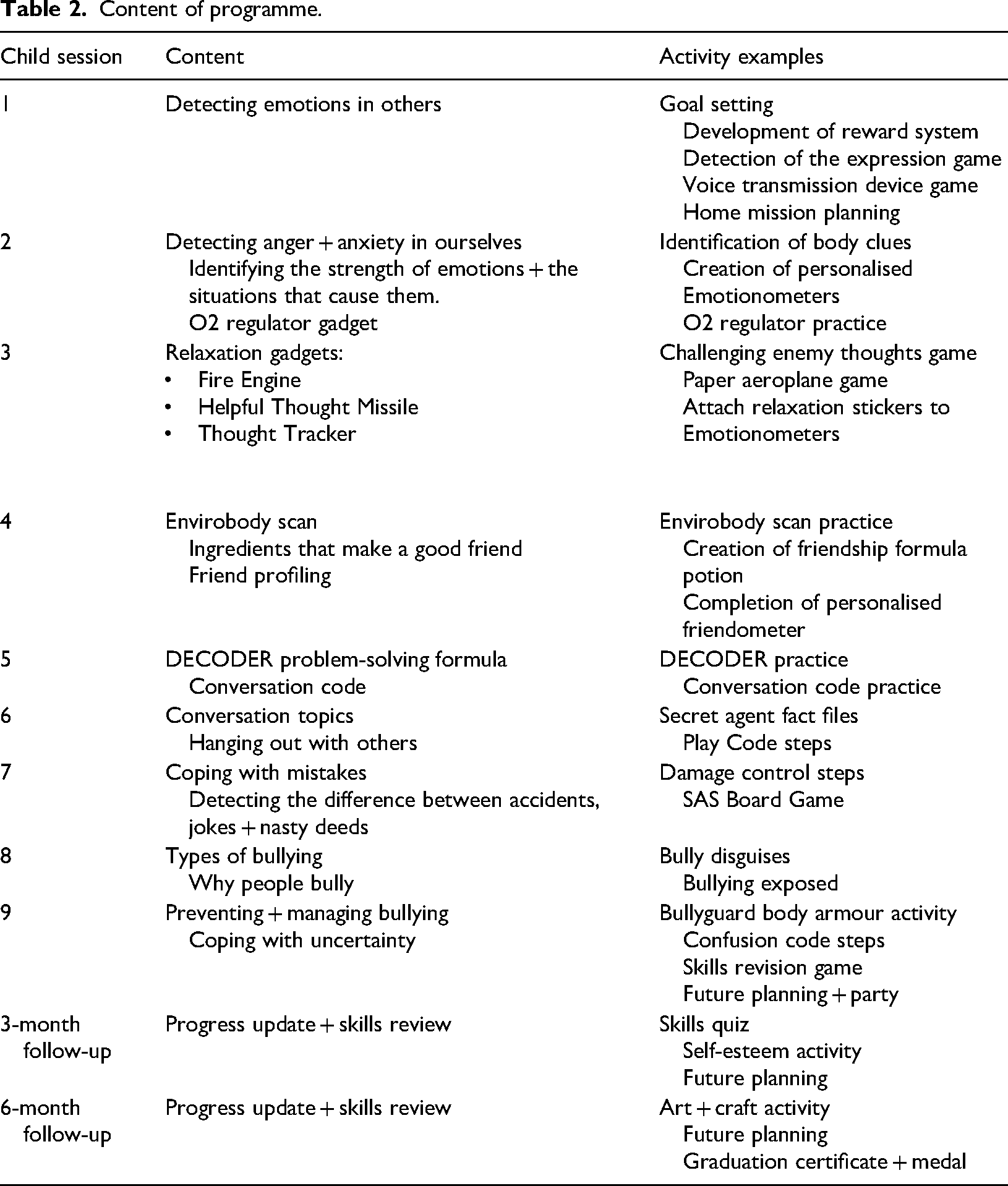
Parent meetings: Parents attended 1 × 2 h introductory meeting. Its purpose was to outline the content and structure of SAS, allow parents to meet each other and discuss essential aspects of the programme. A further 3 × 2 h parent group meetings subsequently took place, after every third children's group session. Sessions reflected the content covered in the children's sessions (outlined in Table 2 and described below), with the aim of enabling parents to support their child's SAS skills at home.
Content of programme.
Content of programme.
Teacher meeting: The class teacher of each child was invited to attend 1 × 2 h information meeting. The aims of the meeting were to introduce teachers to SAS, outline their role in the intervention and promote joint working between CAMHS and education. Teachers were given a Teacher Tip Sheet pack, which contained an overview of SAS skills and outlined how they could support the children to use their skills in school. Pre-intervention outcome measures were also completed.
Children's group sessions: 9 × 90 min weekly sessions were delivered to groups of 5–6 children by two researchers. Sessions progressed from teaching skills such as recognising and labelling emotions in oneself and others, to more complex skills such as using relaxation strategies to regulate emotions. Behavioural components included positive reinforcement, role play and the use of brightly coloured, visual material. A token reinforcement system was used to reward children for being kind to each other and trying their best. Between sessions, children completed ‘home missions’ to promote generalisation of social communication and emotion regulation skills. Skill tracker cards allowed monitoring of and subsequent rewarding for children's use of these skills at home and at school.
SAS computer game: Children also played the SAS computer game at home with a parent, to further reinforce skills taught. They were encouraged to do this for 5–10 min up to 3 times a week. Played over four levels, the game includes virtual reality missions whereby the child assumes the role of an avatar and applies SAS skills in simulated social situations. It is accessed online via a unique activation code given to each parent, using a device the family already has access to (e.g. their own PC/laptop/tablet).
Follow-up: Parents and children were invited to attend one 90-min group session 3 and 6 months post-intervention. The purpose was to review how the children were progressing with their SAS skills and to discuss ways to promote further social-emotional skills development. Outcome measures were completed again by parents and children and posted to teachers.
Quantitative data was collated by the researchers and inputted using IBM SPSS Statistics (Version 25) software (IBM, 2017). To ensure data entry accuracy on parent and teacher questionnaire data, all data was initially scored manually and then electronically by the principal investigator and one associate researcher. Where discrepancies were noted, the raw data was consulted and a consensus was reached between researchers as to the final score to be entered.
Mothers’ and fathers’ data were analysed separately as recommended by Phares et al. (2005).
For parent and teacher outcome measures, a repeated measures analyses of variance (ANOVA) with a Greenhouse–Geisser correction were used to compare data from both the SSQ and ERSSQ at the four timepoints. Due to the large number of primary statistical analyses performed, a Bonferroni adjusted alpha of (0.050) was applied. Post hoc analysis was conducted using a series of paired t-tests to explore the comparison of pre- to post-intervention scores and at 3- and 6-month follow-up.
It was sometimes difficult to ensure questionnaire return by parents and teachers. This may have been influenced by the system of receipt and return (i.e. reliance on parents/teachers to return questionnaires by post) and by the timing of questionnaire posting (some timepoints were around school holidays). A Little's Missing Completely at Random test indicated the missing values were random (χ2 = 485.00 (477), p = 0.387) indicating no clear systematic explanation for missing data. Therefore, additional analysis was conducted using the intention-to-treat principle via the ‘last observation carried forward’ (LOCF) method.
Children's responses on the JATMT and DIBT measures were scored by both the principal investigator and one associate researcher. Ambiguities were discussed with a third researcher who was blind to time of assessment, until 100% inter-rater agreement was reached. Children's data was also analysed using a repeated measures ANOVA with time of assessment as the within-subjects factor.
Programme fidelity
The study was conducted by the first three researchers, who were all practicing Senior SLTs in CAMHS and trained SAS facilitators. The study adhered to recommendations set out by the developer as outlined in the SAS treatment manual. Session checklists provided in the manual were completed prior to each session and used as a treatment protocol.
Results
Parent and teacher outcome measures
(i) Social Skills Questionnaire (SSQ)
It was determined, using repeated measures ANOVA with a Greenhouse–Geisser correction, that mean SSQ scores for mothers, fathers and teachers improved significantly between timepoints of pre-intervention, post-intervention and 3- and 6-month follow-up (F (1.985, 99.273) = 24.900, p < 0.001). Post hoc analysis with a Bonferroni adjustment (0.050) revealed that SSQ scores statistically significantly increased from pre-intervention to post-intervention (5.03 (95% CI, 2.79 to 7.26), p < 0.001), from pre-intervention to 3-month follow-up (5.18 (95% CI, 2.82 to 7.55), p < 0.001) and from pre-intervention to 6-month follow-up (5.39 (95% CI, 2.72 to 8.07), p < 0.001).
A series of paired t-tests (with 0.050 Bonferroni correction applied) were conducted to explore the comparison of pre-intervention SSQ scores (Pre) to scores post-intervention (Post), at 3-month (3 m) and at 6-month follow-up (6 m) for each participant group (Figure 2).
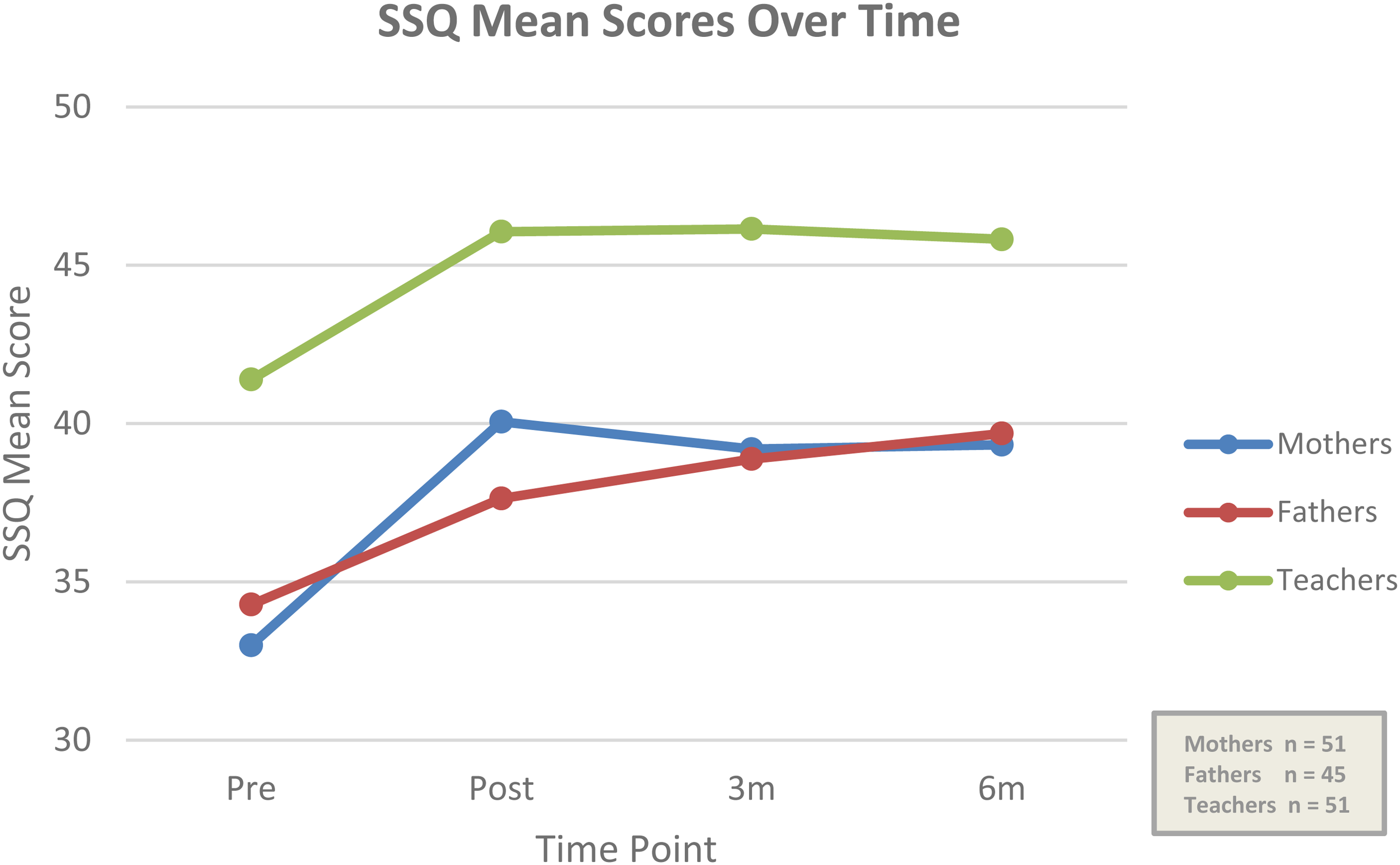
Mean SSQ scores for each participant group over four timepoints.
Statistical significance was maintained for mothers and fathers up to 6-month follow-up and for teachers up to 3-month follow-up (Table 3).
(ii) ERSSQ
SSQ results from paired t-tests.
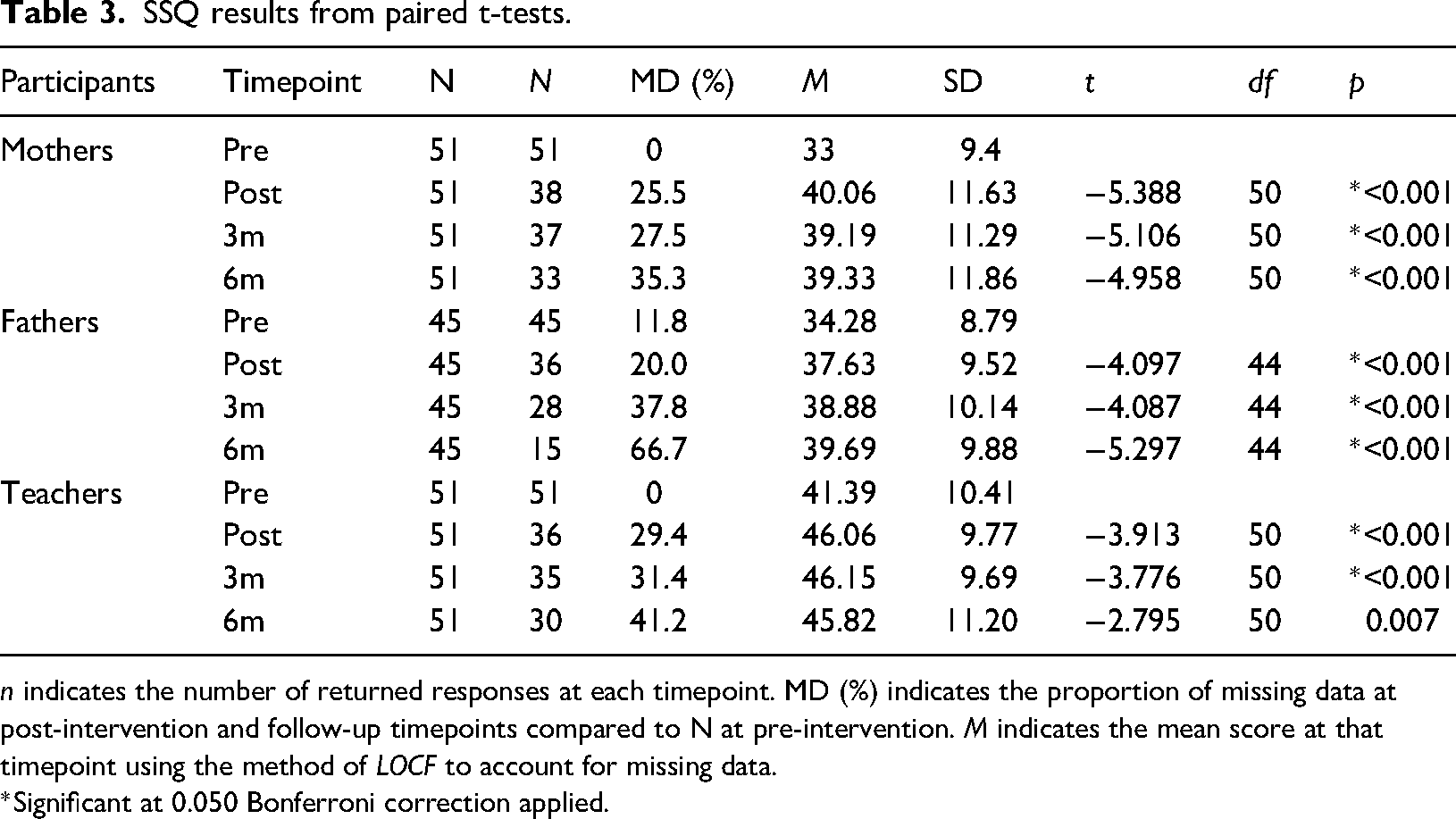
n indicates the number of returned responses at each timepoint. MD (%) indicates the proportion of missing data at post-intervention and follow-up timepoints compared to N at pre-intervention. M indicates the mean score at that timepoint using the method of LOCF to account for missing data.
*Significant at 0.050 Bonferroni correction applied.
It was determined, using repeated measures ANOVA with Greenhouse–Geisser correction, that mean ERSSQ scores for mothers, fathers and teachers improved significantly between timepoints of pre-intervention, post-intervention, 3 and 6-month follow-up (F(1.787, 89.358) = 27.302, p < 0.001). Post hoc analysis with a Bonferroni adjustment (0.050) revealed that ERSSQ scores statistically significantly increased from pre-intervention to post-intervention (8.36 (95% CI, 5.03 to 11.68), p < 0.001), from pre-intervention to 3-month follow-up (7.39 (95% CI, 3.86 to 10.92), p < 0.001) and from pre-intervention to 6-month follow-up (7.46 (95% CI, 3.54 to 11.37), p < 0.001).
A series of paired t-tests (with 0.050 Bonferroni correction applied) were conducted to explore the comparison of pre-intervention ERSSQ scores to scores post-intervention, at 3- and 6-month follow-up for each participant group (Figure 3).
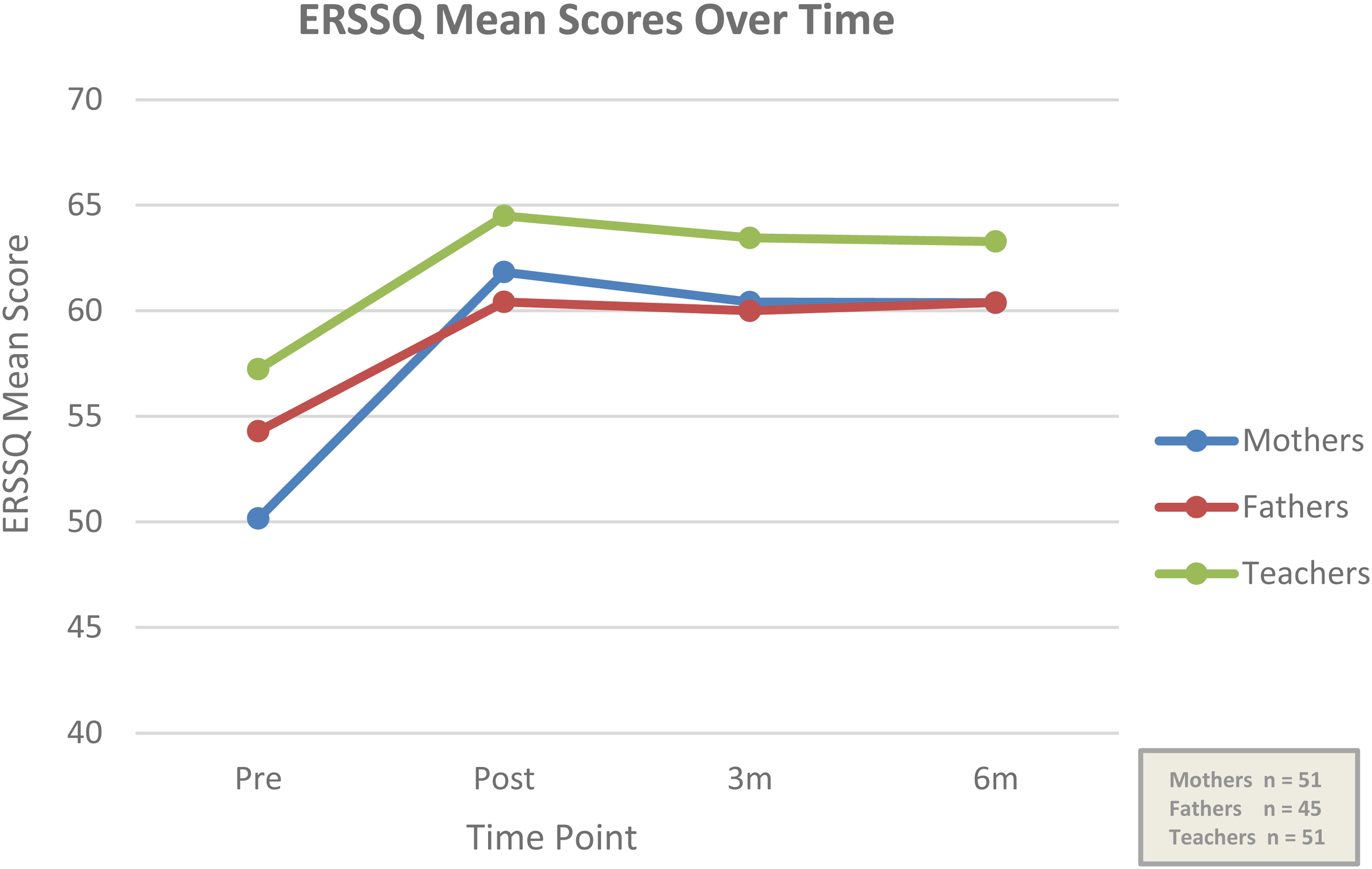
Mean ERSSQ scores for each participant group over four timepoints.
Statistical significance was maintained for mothers and fathers up to 6-month follow-up and for teachers up to 3-month follow-up (Table 4).
(iii) Programme Satisfaction Questionnaire (PSQ)
ERSSQ results from paired t-tests.
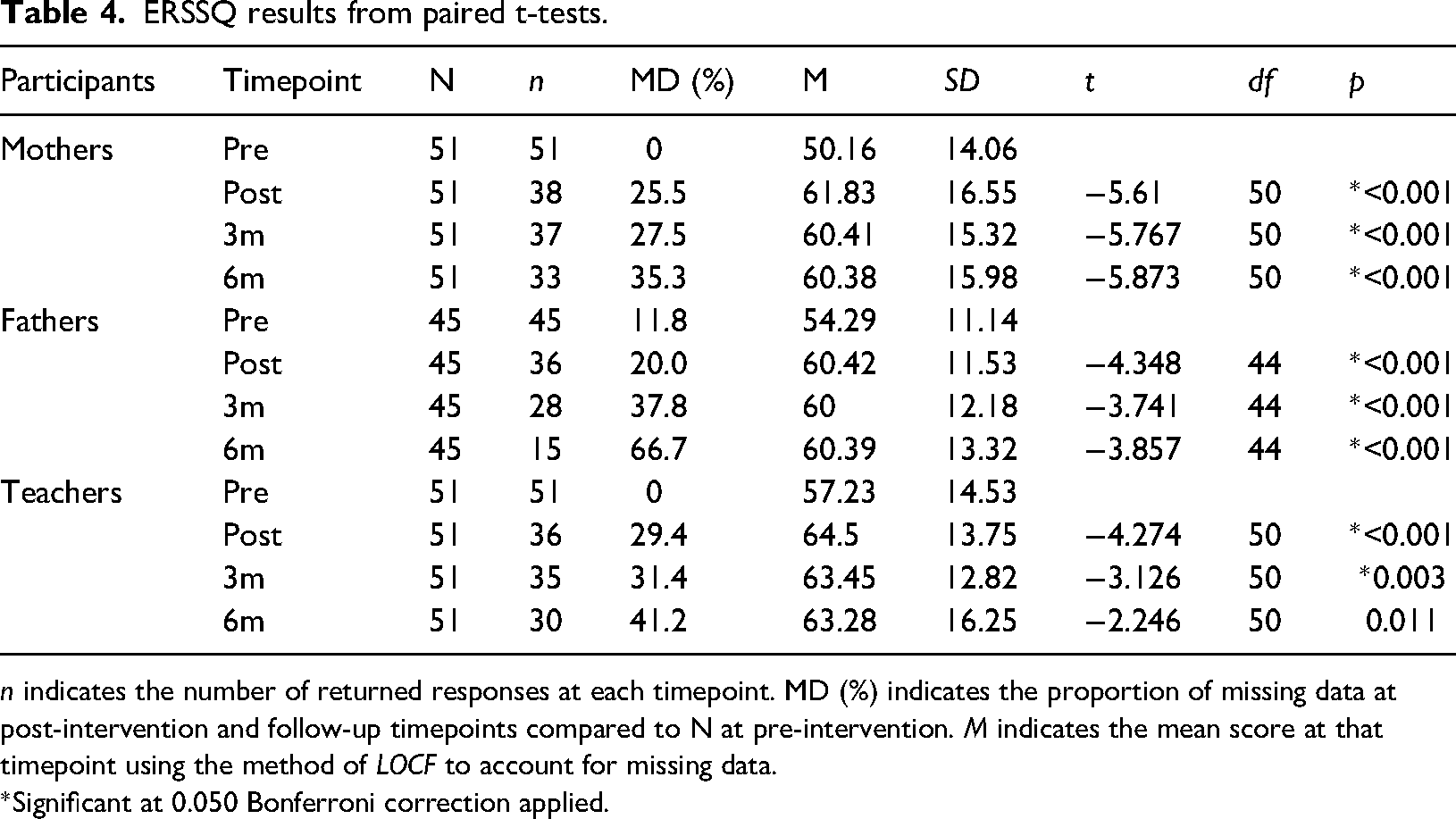
n indicates the number of returned responses at each timepoint. MD (%) indicates the proportion of missing data at post-intervention and follow-up timepoints compared to N at pre-intervention. M indicates the mean score at that timepoint using the method of LOCF to account for missing data.
*Significant at 0.050 Bonferroni correction applied.
Forty-nine out of 96 parents (34 mothers and 15 fathers) returned the PSQ at 6-month follow-up. Parents were asked two dichotomous categorical questions with either a ‘Yes’ or ‘No’ answer. The first question was ‘do you believe the SAS programme contributed to lasting changes in your child's skills and/or behaviour?’ 67% of parents (n = 33) answered ‘Yes’. 33% answered ‘No’ (n = 16). The second question was ‘do you believe that the programme contributed to lasting changes in how you support your child?’ 84% (n = 41) of parents answered ‘Yes’. 16% (n = 8) answered ‘No’ (Figures 4 and 5).
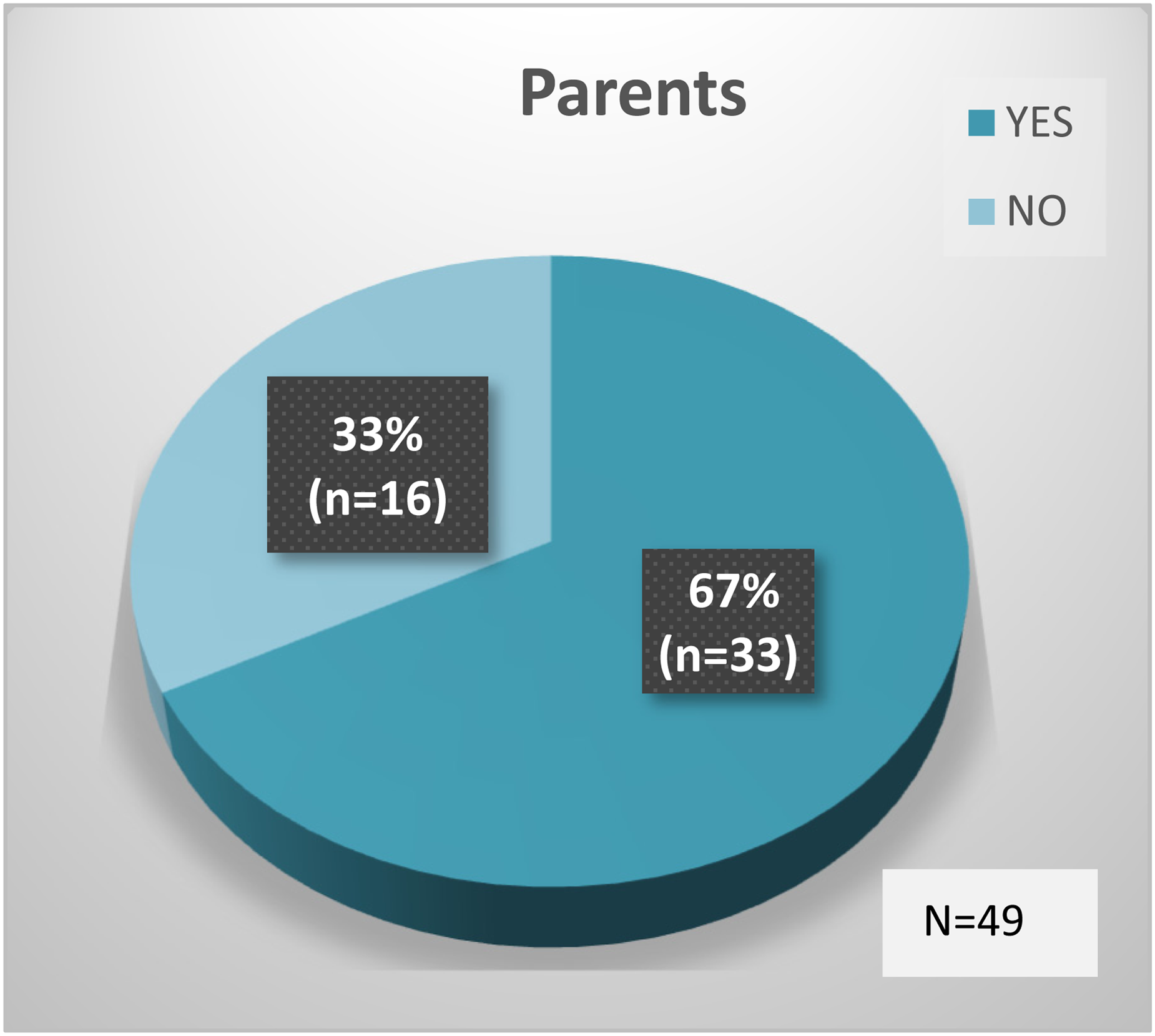
SAS contributed to lasting changes in child's skills and/or behaviour.
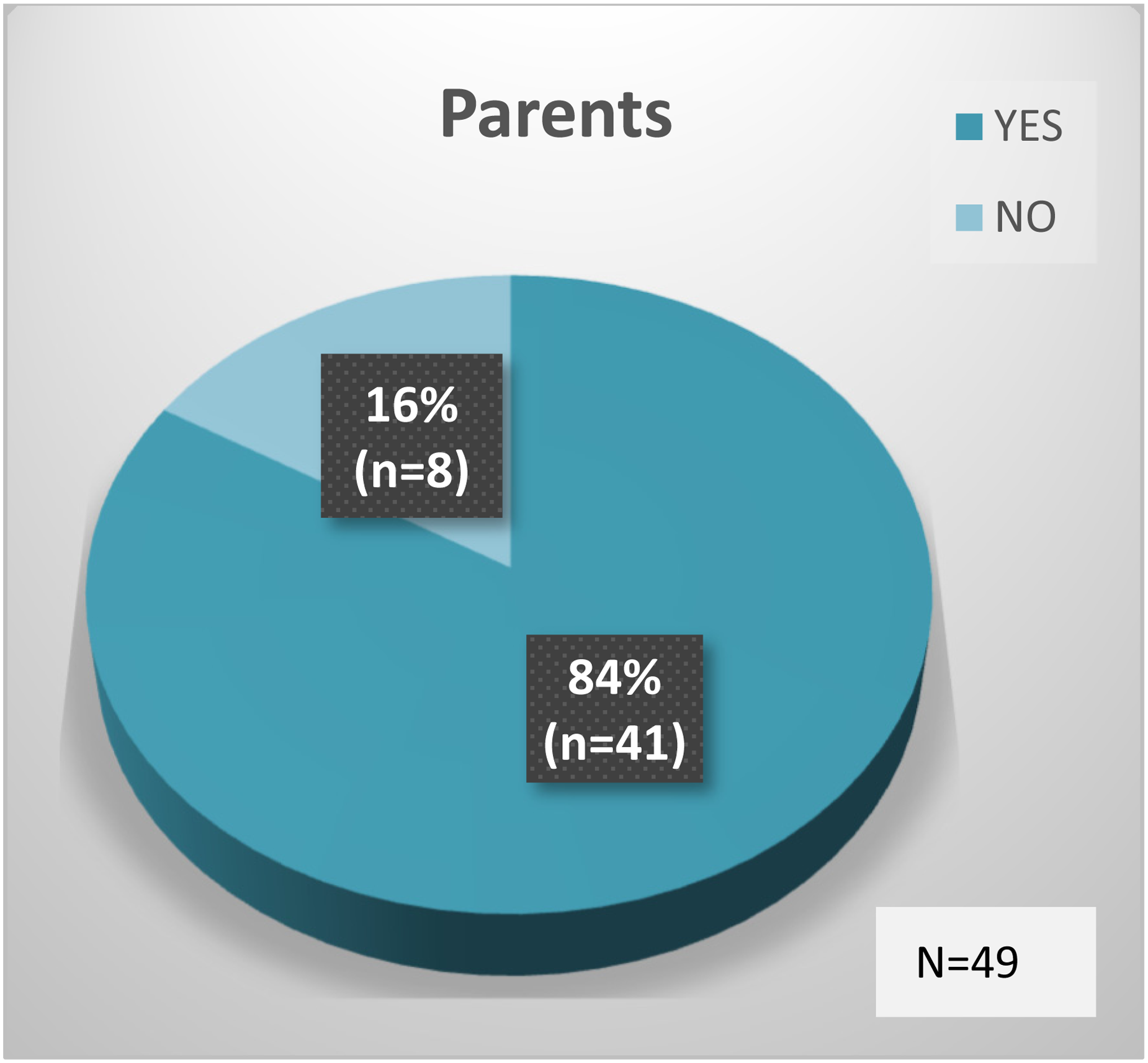
SAS contributed to lasting changes in how parents support their child.
Twenty-eight out of 51 teachers returned the PSQ at 6-month follow-up. Teachers were asked one dichotomous categorical question with either a ‘Yes’ or ‘No’ answer: ‘do you believe the SAS programme contributed to lasting changes in your student's classroom/playground behaviour?’ 75% (n = 21) of teachers answered ‘Yes’. 25% (n = 7) answered ‘No’ (Figure 6).
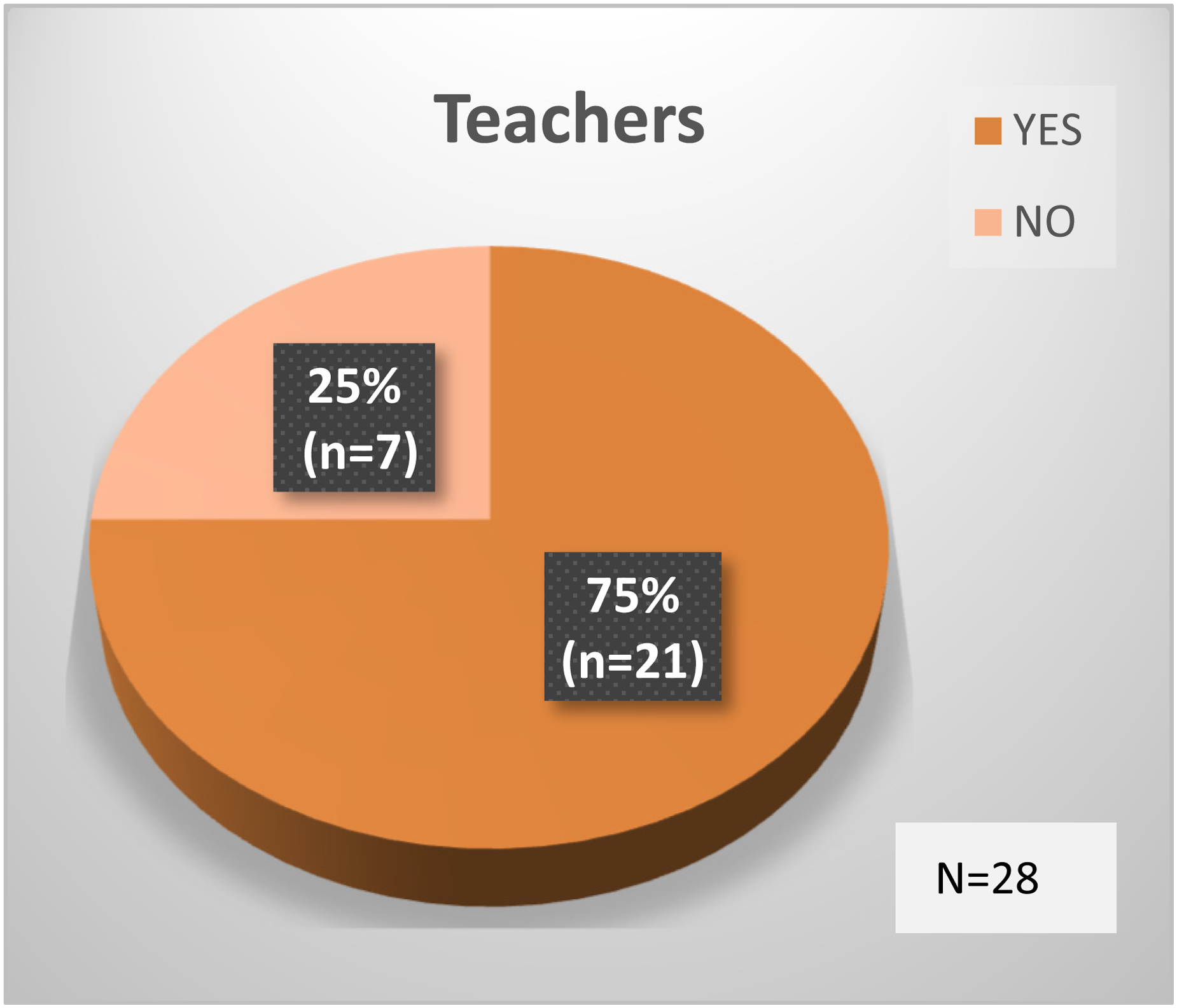
SAS contributed to lasting changes in student's classroom/playground behaviour.
(i) James And The Maths Test (JATMT)
A repeated measures ANOVA of the mean JATMT scores showed statistically significant improvement from pre-intervention to 6-month follow-up (F(3, 75) = 22.754, p = 0.001) (Figure 7).
(ii) Dylan Is Being Teased (DIBT)
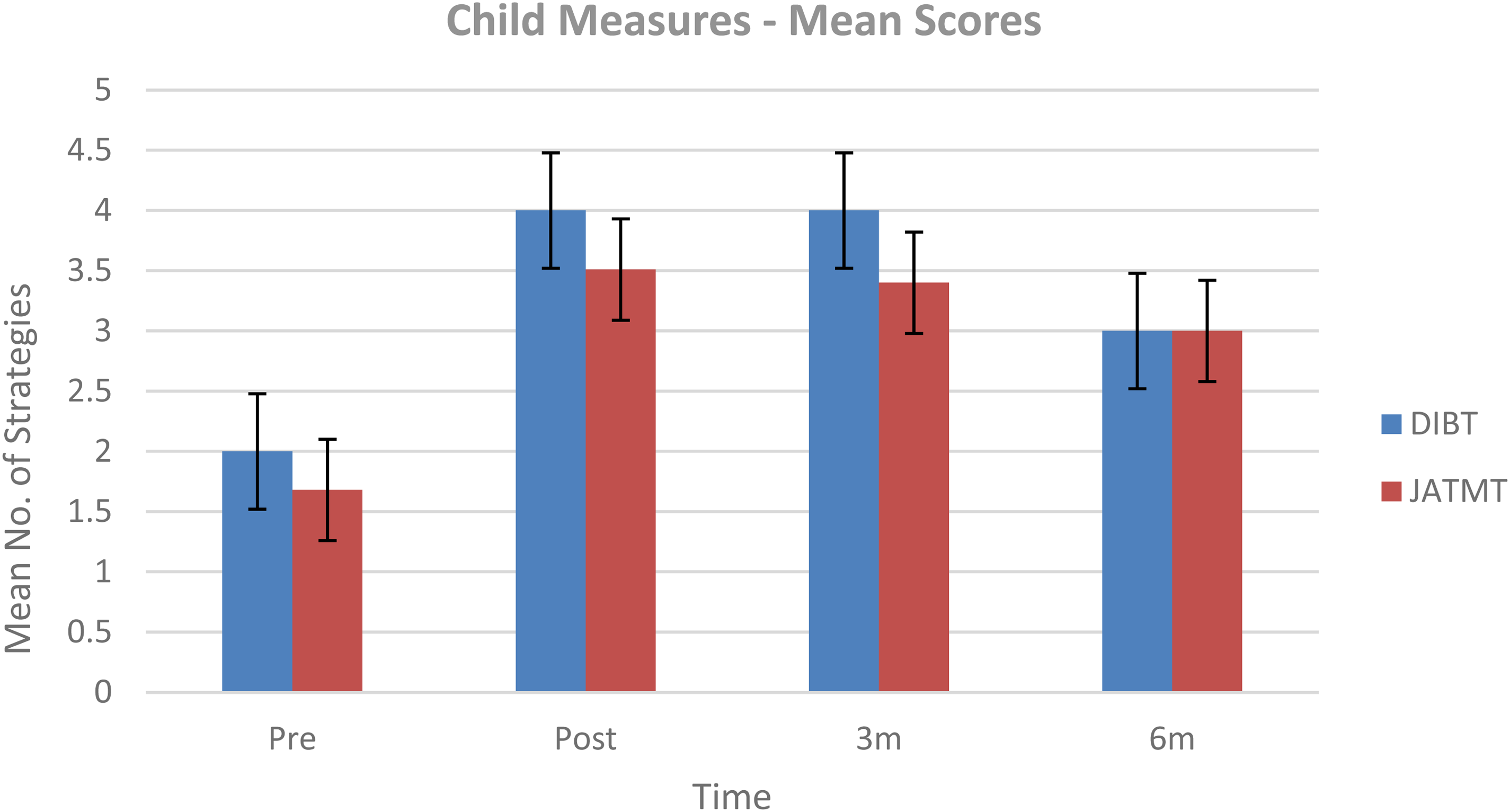
Mean scores of JATMT and DIBT over four timepoints.
A repeated measures ANOVA of the mean DIBT scores also showed statistically significant improvement from pre-intervention to 6-month follow-up (F(3, 75) = 9.144, p = 0.001) (Figure 7).
92.2% of children (47/51) completed both JATMT and DIBT measures post-intervention (7.8% missing data (MD)).72.5% (37/51) completed the measures at 3-month follow-up (27.5% MD) and 54.9% (28/51) at 6-month follow-up (45.1% MD).
This study sought to extend the existing international evidence based for SAS by examining its effectiveness in three community CAMHS clinics in Ireland, with Senior SLTs as facilitators. Aims were to determine if the SAS programme led to improvements in children's (a) social communication, (b) emotional regulation and (c) knowledge of strategies. Overall, results demonstrated positive outcomes for children, their parents and teachers, with most intervention gains maintained at 6-month follow-up.
Aim 1: improvement in social communication
Both mothers and fathers reported statistically significant improvements in children's social communication from pre- to post-treatment on the SSQ-P. Prior SAS research documented treatment gains on the SSQ-P that were maintained at 6-week follow-up (Beaumont et al., 2019; Sofronoff et al., 2015) and at 5-month follow-up (Beaumont and Sofronoff, 2008). However, the current study investigated one of the longest post-intervention periods and demonstrated gains in social communication that were maintained up to 6-months post-treatment.
Teachers in the current study also reported improvements for children on the SSQ-T with maintenance at 3-month follow-up. 35% of children (n = 18) had experienced a change of teacher by the 6-month follow-up timepoint. These teachers had known the child for just 1 month at the time of questionnaire completion, which may have impacted their responses.
Nineteen of the 51 children (37%) had dual diagnoses (autism and ADHD, autism and AD, ADHD and AD). Children with ADHD and autism in particular can present a unique challenge in terms of treatment response (Elwin et al., 2020; Ghriwati et al., 2017). This is due to a variety of factors, including greater impairments in daily functioning and increased risk of developing additional psychological disorders, compared to children with either disorder in isolation (Thomas et al., 2018). 20% of children in the study presented with both ADHD and autism. Of note, recent research supports a transdiagnostic approach to clinical practice, whereby children's strengths and vulnerabilities common to multiple diagnoses are treated simultaneously, rather than focusing on one specific diagnostic condition at a time (Hobson, 2022). Indeed, therapy that supports underlying factors rather than individual disorders could have positive effects on all the disorders the factors are related to (Mansell et al., 2009). Findings support the feasibility of offering transdiagnostic treatment programmes such as SAS to children with dual diagnoses. However, further analysis of, and comparison between, the separate diagnostic groups is warranted.
This was the first SAS study to investigate parent and teacher responses on the Programme Satisfaction Questionnaire (PSQ). Six months after the programme ended, 67% of parents and 75% of teachers reported the presence of ‘lasting changes’ in children's skills and behaviour. This is especially pertinent given the complexity of the children's presentations and the fact that the nature of childhood mental health disorders means that difficulties are often persistent (Reid et al., 2015). It is hypothesised that the ‘lasting changes’ achieved may be associated with parental participation, a vital component of the SAS programme (Beaumont and Sofronoff, 2008). There is a growing body of research demonstrating the effectiveness of parental involvement in social communication group interventions (Hock et al., 2015; Laugeson et al., 2012). Costley et al. (2020) concluded that when parents are committed to participating in their child's intervention, this has a positive impact on the child's competence. Moreover, by including parents in the intervention, treatment has the potential to continue indefinitely, even in the context of time-limited therapy (Laugeson et al., 2012).
Teacher involvement in SAS could also have contributed to the ‘lasting changes’ reported. This may be due in part, to the teacher information sessions attended by all 51 teachers. All teachers were contacted by phone following the fourth children's session, to discuss their experience of SAS and to identify solutions to possible implementation barriers. Weekly tip sheets updated teachers on what the children were learning and how to support generalisation of skills. These factors may have led to increased collaboration between CAMHS and education and enhanced compliance with supporting children's use of SAS skills in the classroom.
Aim 2: Improvement in emotional regulation
Statistically significant improvements were also reported by both mothers and fathers regarding their children's emotional regulation on the ERSSQ-P, with significance maintained up to 6-month follow-up. This is important given that difficulty with emotional regulation has been implicated in the development and maintenance of most psychiatric disorders (Berking and Wupperman, 2012) and that teaching children to manage their emotions has been described as one of the greatest challenges for clinicians (Ayres and Vivyan, 2019). Consistent with the findings of this research, previous SAS studies also showed improvements in the area of emotional regulation (e.g. Beaumont et al., 2021; Weiss et al., 2018). However, as previously mentioned, most published SAS research investigated shorter post-intervention periods and focused on children with autism, rather than those with autism (and/or other neurodevelopmental disorders) and moderate-severe mental health disorders.
Teachers also reported improvements for children's emotional regulation on the ERSSQ-T, with maintenance up to 3 months. Again, a change of teacher at the 6-month follow-up timepoint may have influenced responses.
Another noteworthy difference between the current study and prior research is the gender of child participants. Previous SAS research has a strong bias towards male participants, with a stark under-representation of females. For instance, in the original randomised control trial of SAS (Beaumont and Sofronoff, 2008), only 10.2% of the children were female. Subsequent research included female cohorts from 7.8% (Beaumont et al., 2015) to 26% (Beaumont et al., 2019). In contrast, 41% of children in the current study were girls. This mirrors clinical practice in community CAMHS, where increasing numbers of young females are being referred. 45% of the 318 children referred for emergency mental health assessment in the aforementioned hospital study were female (Maguire et al., 2020). Teenage girls in Ireland are more likely to report being unhappy or having poor life satisfaction than their male counterparts (Kolto et al., 2020), while the negative impact of the Covid-19 pandemic on adolescent mental health has been found to be more pronounced in girls (Halldorsdottir et al., 2021). Interventions that promote gender inclusivity are therefore essential for children attending CAMHS. Findings suggest that SAS is an equally effective treatment programme for both genders, but further research is merited.
84% of parents reported experiencing ‘lasting changes’ in terms of how they support their child at the 6 month timepoint on the PSQ. Indeed, parents themselves have been shown to benefit from involvement in other social skills interventions (Costley et al., 2020). Although research in this area is limited, it has been suggested that parents who play an active role in child-directed social skills programmes experience gains in their own self-efficacy (Karst et al., 2015) and emotional well-being (Radley et al., 2014).
Aim 3: Improvement in children's knowledge of strategies
There was a statistically significant difference in the number of anxiety and anger management strategies generated by the children on both measures (James and the Maths Test and Dylan is Being Teased) following completion of the SAS programme. Children's knowledge of strategies was maintained up to 6-months post-intervention. No specific child measure in the study examined whether children's knowledge of strategies resulted in actual behavioural change. Instead, information regarding real-life behavioural change for the children was sought from parent and teacher point of view through completion of the SSQ-P/T and the ERSSQ-P/T. However, children's knowledge of strategies is an important prerequisite for their ability to put skills into practice in everyday life (Beaumont and Sofronoff, 2008). Indeed, Moody and Laugeson (2020: 361) noted that changes in knowledge following intervention can generate ‘downstream effects’ in children's social behaviour, as the skills are used and subsequently reinforced over time and across contexts.
Clinical implications
Primary school children can be underserved in CAMHS where the focus is often placed on crisis management for adolescents, despite increasing numbers of children under 12 years being referred (Maguire et al., 2020). SAS allows young children with mental health difficulties access to an evidence-based treatment that develops social-emotional resilience. Increasing children's social competence may result in a positive feedback loop, where positive reinforcement is received through successful social situations, thus reducing future social anxiety and emotional regulation difficulties (Factor et al., 2022). This is critically important in light of high recurrence rates for childhood anxiety disorders, the increasing prevalence of children's mental health disorders and the long-term consequences of these disorders being left untreated (McNicholas, 2018; Schraeder and Reid, 2017).
SAS involves significant financial costs, both in terms of facilitator training and purchasing of resources for children, parents and teachers, which may impact the feasibility of service delivery for some clinics (authors obtained grant funding for the purchasing of SAS resources). Most outpatient CAMHS teams in Ireland are under-resourced (McNicholas, 2018) and clinicians regularly face the challenge of balancing increasing therapeutic demands with limited resources (Hansen et al., 2021). However, the relatively short duration and group format of SAS suggest that it has the potential to be a cost-effective option for children attending CAMHS, particularly given the magnitude and longevity of treatment effects shown. The transdiagnostic aspect of SAS, combined with the dual benefit of improving both social communication and emotional regulation may further maximise cost-effectiveness.
Limitations
Study findings are an exploratory account of the impact of SAS in a community CAMHS setting and so are tentative in nature. Generalisability of the findings is limited by the demographics of the sample (all Caucasian, born in Ireland, most monolingual) and should be determined by the reader.
Several limitations should be acknowledged when interpreting the findings, including the absence of a control group and a relatively small sample size. Parents and teachers were both the intervention-delivery agents and the evaluators, making them more susceptible to responder bias. Researchers were also the programme delivery facilitators. The participant group was highly motivated as evident in the high attendance rate, which may have contributed to the treatment effects demonstrated.
Future research using a randomised design with a larger sample size and a longer follow-up timeframe would be valuable. Analysis of how children with specific diagnoses responded to treatment (especially those without autism) was outside the scope of this article but will be examined in future publications. In-depth exploration of a potential relationship between gender difference and intervention efficacy would also be of interest. Future research could employ a multiple baseline design to strengthen the findings.
In recent times there has been a growing awareness of the importance of fathers’ roles in clinical child research, reflecting increased paternal involvement in caregiving (Davison et al., 2017). However, as noted by Panter-Brick et al. (2014) the science of paediatric practice is impeded by lack of information from fathers. To the authors’ knowledge, this is the only SAS study that investigated treatment effectiveness from mothers’ and fathers’ viewpoints separately. Time and resource constraints precluded more in-depth analysis. Future exploration of the data will investigate the specific variables that may impact effectiveness from fathers’ experiences.
Conclusions
This research extends the existing evidence base for SAS by demonstrating significant treatment effects for 51 children with moderate-severe mental health disorders attending community CAMHS in Ireland. Findings highlight preliminary evidence of social-emotional skill generalisation to the home and school environment up to 6-months post-intervention. A cost–benefit analysis is recommended to investigate the feasibility of offering SAS in other outpatient community services. SLTs have a vital role in delivering intensive, CBT-informed support for children with complex diagnostic profiles within CAMHS and other specialised multi-disciplinary teams.
Footnotes
Acknowledgements
Researchers would like to thank the children, parents and teachers who participated in the study and Mr Peter Gallagher (Research Support Service, Saint John of God Research Foundation) for his assistance with statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant funding was obtained through the Saint John of God Development Company to purchase SAS resources for participants.