
Abstract
Research on digitalisation in the public sector has largely overlooked trade unions or found mainly top-down change and limited involvement. This article focuses on unions representing admin workers in hospitals in Norway and the devolved nations of the UK. Drawing upon interviews in two unions, it offers a novel analysis of their involvement and influence in digitalisation, emphasising the interrelationships between union power and forms of political governance at multiple levels. The findings underline the enduring role of national systems, but with regions and devolved nations offering distinct patterns of union influence, and reveal some promising cases in Norway and Scotland.
Introduction
Digitalisation is said to be having a substantial impact on the public sector, including how employees work and citizens access services (Andersson et al., 2022). The promise of improved outcomes, along with the automation of bureaucratic and routine tasks, has obvious appeal to cost-conscious governments and managers (Kirov, 2017). A central focus has been the digitalisation of administrative and clerical work (hereafter: ‘admin work/workers’). This is particularly prominent within healthcare where ‘Big Tech’ has been offering ‘solutions’ around digitalised medical records and patient management systems (Voss and Rego, 2019) which, it is claimed, will free up resources for clinical services (NHS England, 2023). In public hospitals, admin workers may, therefore, be faced with job loss or new working practices.
This article explores whether unions in public hospitals can shape digitalisation affecting admin workers – a diverse group of predominantly female workers, including medical secretaries, ward clerks, medical records staff, audio typists and receptionists. Several studies have highlighted the difficulties of implementing digitalised patient records and management systems, including technical failures and additional work burdens for clinical staff (Håland, 2012; Knudsen and Bertelsen, 2022). However, admin workers and the ability of unions representing them to influence decisions and outcomes are largely overlooked.
We take as our starting point that whether and how digital technologies are introduced, along with their impact on workers, are ‘socially shaped’ by key actors, including government, employers and unions (Howcroft and Taylor, 2023). Within particular national, sector and workplace contexts, these actors have varied interests and different levels of power to influence technology decisions (Doellgast and Wagner, 2022; Lloyd and Payne, 2021a). Exploring the public sector entails an additional level of analytical specificity compared with manufacturing or private-sector services. Governance and politics play a key role in technology decisions and implementation that may take place at multiple levels (Collington, 2022; Kuhlmann and Bogumil, 2021), potentially offering additional opportunities for union influence. In most Western European countries, hospitals have high rates of unionisation and institutionalised social dialogue (Bechter et al., 2012: 195), which would seem to bode well for union involvement in digital change. Yet, the few studies that have examined unions’ role, either in hospitals or in the public sector more broadly, suggest a mixed picture (Leonardi, 2023; Voss and Rego, 2019: 56).
A multi-level analysis of unions’ role in digitalisation is adopted in this article through a comparison of Norway and the UK, two countries with starkly contrasting models of capitalism. Norway is noted for its social dialogue and tripartism, multi-level collective bargaining and relatively strong unions (Alsos and Trygstad, 2018), the UK for its lightly regulated labour market, low bargaining coverage and weakened and marginalised unions (Martínez Lucio and MacKenzie, 2024). In Norway, Basic Agreements between the ‘peak-level’ union and employer confederations, alongside the Working Environment Act, require unions to be consulted and involved in technological change (Alsos and Trygstad, 2018). In the UK, consultation rights only apply where potential redundancies arise.
These differences in national industrial relations systems narrow in the case of public hospitals where both countries have high union density, sector-wide collective bargaining and institutionalised forms of consultation at various levels. Governments have also pursued forms of New Public Management (NPM), albeit less so in Norway, and have restricted hospital budgets with ensuing problems of waiting lists, staff shortages and concerns over care quality (Aas et al., 2021). In the UK, four different hospital governance arrangements exist following devolution, affording a further opportunity to probe the influence of national political and institutional specificity.
This article focuses on two research questions. First, to what extent are unions able to influence initial decisions over the introduction of digital technologies affecting admin work? Second, are unions representing these workers involved in the implementation process? In addressing these questions, we explore country differences in union involvement in digitalisation in respect of this sector and group of workers. The research draws on interviews with union officers and lay representatives from the two largest public sector unions in Norway and the UK, Fagforbundet and UNISON. These offer critical insights from perspectives that are often overlooked in studies of digital change in the public sector. The research also makes a significant contribution by incorporating governance and political processes into the comparative analysis of unions’ ability to shape digitalisation.
The article opens with a discussion of the literature on union involvement in digitalisation, outlining our multi-level analytical approach and incorporating the role of public governance. Next, the digital technologies affecting admin workers in hospitals are discussed, followed by an outline of key features of the sector in Norway and across three systems (England, Wales and Scotland) in the UK. The research methods are then presented. The findings are structured around the two research questions: unions’ role in initial digitalisation investment decisions and their involvement in implementation at hospital level. The ensuing discussion draws out the influence of country effect vis-a-vis sector specificity, before concluding with the study’s contribution to analysing unions’ role in public-sector digitalisation.
Unions and digitalisation in the public sector
In many advanced economies trade unions have traditionally found it difficult to influence technology decisions, especially in the UK and other neoliberal countries (Beirne and Ramsay, 1992; Deery, 1989). By contrast, Germany and the Nordic countries have, historically, afforded more supportive institutional environments and forms of social dialogue that opened up greater opportunities for union involvement (Deutsch, 1986). There is some evidence that these differences persist, with examples of country variation in unions’ abilities to shape digitalisation at the workplace (Doellgast and Wagner, 2022; Lloyd and Payne 2023, 2025). However, the public sector remains marginal in these studies.
In this article, we adopt a multi-level analytical approach to understanding unions’ role in digital change, as expounded elsewhere (Lloyd and Payne, 2021a). This approach emphasises the critical role of union power at the level of the workplace and the sector, alongside the wider trade union movement’s ability to shape the national regulatory context within which unions act in relation to digitalisation. As such, it shares certain affinities with other frameworks (Gasparri and Tassanari, 2020; Lévesque and Murray, 2010). There is agreement that while national institutions matter, the relative power and ability of unions to organise and mobilise workers will vary across sectors within a country (Bechter et al., 2012). This creates an uneven terrain of boundary conditions within which unions can act to shape digitalisation. Sectoral factors, for example, may narrow differences between countries with contrasting national institutional environments. Unions, regardless of country, might be expected to have more limited involvement in digitalisation in typically difficult-to-organise sectors like retail (Payne et al., 2023), and greater influence in the public sector where unions are often well organised and have established mechanisms of social dialogue (Voss and Rego, 2019). We may, therefore, find fewer differences in these sectors when comparing neoliberal countries with those having more supportive institutional regimes.
This analytical approach requires further adaptation when applied to the public sector to account for the role of political decision-making. Studies of digitalisation in the public sector often draw on a governance and service delivery perspective, focusing on modernisation and reform agendas, but have little to say about the impact on work and largely ignore unions (Lips, 2019). The literature, nevertheless, offers insights into the dominant role played by the political sphere, including ‘governmental ideas and ideals’ (Plesner et al., 2018: 1177), as well as policy drives and directives. It is important to consider how unions might apply political pressure to elected national and local government representatives (and their political parties) running public services. This opens up possibilities for union influence in digitalisation projects outside of formal managerial structures, opportunities that are typically unavailable in the private sector. It is, therefore, critical to extend analyses of union power (Arnholtz and Refslund, 2024) to include the political nature of the government as ‘employer’.
Studies of technological change have long emphasised the importance of unions being involved in decisions at an early stage (Beirne and Ramsay, 1992). Ideally, this would encompass technology design, an area where unions have only rarely gained admittance (see Ehn, 2017). Digital change in the public sector is more likely to be initiated from decision-making structures above the workplace, and is often large in scale. This may offer certain advantages to unions accustomed to working at sector and national level, given that public sector collective bargaining is typically centralised. Yet, recent evidence suggests that digitalisation in the public sector is often being pushed by large private tech companies regardless of established negotiation or consultation arrangements (Collington, 2022; Voss and Rego, 2019).
By the time technologies (digital or otherwise) arrive in the workplace, they already reflect the influence of distinct ‘forms of power and authority’ (Howcroft and Taylor, 2023: 354), which impose restrictions on their purpose and use (Wajcman, 2006). These forms of power and authority encompass a range of interests that includes technology companies, lead employers and governments. Technology design is also influenced by existing divisions of labour which in the public sector incorporates power differentials between professional and non-professional groups, and reflects ‘the reproduction and maintenance of gender expectations’ (Frennert, 2021: 4). These ‘immanence’ effects may, therefore, limit unions’ ability to shape technology at the workplace (Beirne and Ramsay, 1992; Edwards and Ramirez, 2016: 105).
National policy decisions and bureaucratic state structures can also reinforce top-down decision-making, squeezing local managers’ room for manoeuvre and further limiting the scope for union influence in the workplace (Ernst, 2022; Lebesby et al., 2023). Admin work is highly feminised and often low status (Truss et al., 2013), adding to the risk that these workers will be marginalised when changes occur. Senior managers and tech providers may have limited understanding of what their jobs involve or how these workers and their representatives may be able to contribute to the implementation of technology.
There are a few studies which have begun to examine the impact of digitalisation in the public sector that include union perspectives (Lloyd and Payne, 2021b). Voss and Rego (2019: 10) note that digitalisation is a ‘polarising issue’ for unions, given the ambivalent potential of these technologies to have positive and negative impacts on workers and public services. They identify international examples where unions are actively seeking to shape ‘a just digital transition’, along with surveys conducted by unions in countries, such as Germany and Norway, which show limited involvement (Voss and Rego, 2019: 56). A recent study of three areas of the public sector in eight European countries finds that digital change is often absent from collective agreements, notwithstanding evidence of informal cooperation in the Nordic countries at workplace level (Leonardi, 2023).
It is important to avoid generalisations about the public sector, given that there are substantive differences in the public profile of services and the way that unions are organised. Healthcare has one of the highest political profiles; for example, in the UK it is frequently cited 1 as the top concern of the electorate. Numerous patient-advocacy groups, campaigns and charities attempt to influence health policy, funding and treatment (Opedal et al., 2012), although there is a lack of research on their potential to shape digital change.
Union organisation is also distinct compared to other areas of the public sector, with a multitude of often competing unions and professional associations. In Norway and the UK, the largest are the two general unions, Fagforbundet and UNISON, along with ‘professional’ unions for nurses and doctors. In addition, there are many smaller occupationally specific unions, covering for example pharmacists or radiographers, which may also seek to influence public policy (Guillaume and Kirton, 2023; SoR, 2025). This multifaceted pattern of health sector governance points to a range of union actors and advocacy groups with the potential to influence digitalisation. Power is not equally distributed across these groups and may also vary by hospital and country, so we should expect a complex and variegated pattern of influence and outcomes.
Digitalisation and administrative work in hospitals
The primary digitalisation process affecting admin workers in hospitals is the transition to electronic medical records (EMRs) systems. 2 This involves various stages from scanning paper records and creating new ones in digital format to the development of wider digital health platforms that aim to integrate records, appointment systems and patient flows across hospital and community care. A substantial evidence base is emerging on these more extensive systems, with reports of widespread technical difficulties, a lack of flexibility for different uses, spiralling costs and lengthy delays (Hertzum and Ellingsen, 2019; Kirchoff et al., 2021; Petrakaki and Kornelakis, 2016).
Speech recognition software that can be integrated into EMRs has often added to these problems. The automatic conversion of clinicians’ voiced notes into text creates transcription errors which require ongoing checking for accuracy, with some high-profile cases of patient harm, for example where incorrect drug doses have been recorded (Barbour and Wright, 2024; Bossen et al., 2014). Evidence suggests that rather than freeing up time for patient care, there has been a redistribution of admin tasks to clinical staff, particularly medics, alongside processes of standardisation and increased control (Bergey et al., 2019; Håland, 2012; Hansen and Baroody, 2023; Petrakaki and Kornelakis, 2016). These safety and workload issues have led to some doctors being reluctant to use the technologies or refusing altogether, with common problems reported across different institutional contexts and hospital systems. (Ernst, 2022; Håland, 2012). Smaller-scale technologies are also being implemented, such as self-service reception and booking systems, where problems have been highlighted but nothing in comparison with EMRs (Bossen et al., 2014).
The experience of admin workers is mostly marginal in these studies which may reflect the view that their work is invisible, misunderstood and undervalued, linked to the gendered nature of these jobs (Bergey et al., 2019). Although nursing is also predominantly a female occupation, and doctors are increasingly gender-balanced, admin work is often seen as comprising ‘routine’ tasks that are ripe for automation and efficiency savings and as marginal to delivering care. Some research, however, has charted the complex range of tasks undertaken by certain groups, such as medical secretaries (Bossen et al., 2014; Knudsen and Bertelsen, 2022). Positioned at the interface of patient administration and clinical care, their role involves liaising between clinicians and nurses as well as carrying out ‘data work’ (such as completing and updating records), which calls for contextual knowledge, accuracy and sensitivity (Knudsen and Bertelsen, 2022).
The relegation of these roles to ‘the background’ (Bossen et al., 2014: 102) may also encourage managers and tech designers to overestimate the routine nature of the job and the ease with which workers can be replaced by technology (Bergey et al., 2019). Perceptions and status may also serve to limit admin workers’ role in digital change processes. Qvarfordt et al.’s (2024: 182) study of medical secretaries suggests that workplace hierarchies and lack of status can act as ‘possible barriers’ to involvement. However, research has largely neglected admin workers or their unions’ participation in digitalisation. Before examining more closely unions’ role in this area, the next section outlines the key features of public hospitals in the UK and Norway, including governance structures and the industrial relations context.
Public hospitals in the UK and Norway
In the UK, health has been a devolved issue since 1999, with England, Scotland, Wales and Northern Ireland operating their own National Health Services (NHS). Following devolution, NPM reforms that were first introduced across the UK, such as internal markets, performance management systems, self-governing hospital trusts and the contracting-out of support services (Simonet, 2015), were partly disbanded in Scotland and Wales. Both countries removed the internal market and reintroduced Regional Health Boards (RHBs) to oversee healthcare (Bacon and Samuel, 2017), as NHS England moved further towards marketisation. Union membership in hospitals is high and likely to exceed the public-sector average of 48.6% (DBEIS, 2023). Although there remains UK-level collective bargaining over terms and conditions (including grading structures), pay rates associated with grades are decided by the devolved governments. 3 All nations also have their own national-level consultative body, entitled ‘partnership forum’.
In England, staff are employed by over 200 NHS trusts. 4 In Scotland and Wales, the employer is the Regional Health Board, of which there are 14 in Scotland and seven in Wales. RHBs have an elected employee representative on their management board, but there is no such requirement for trusts in England. Formal structures of multi-union negotiation and/or consultation operate at regional level in Scotland and Wales, and at hospital/trust level in all nations. Scotland has gone further in terms of engagement with unions through ‘social partnership’ mechanisms from national policy level through to local hospitals (Bacon and Samuel, 2017). A recent review found that partnership in NHS Scotland ‘works extremely well’, with positive examples outnumbering ‘dysfunctional cases’ (Findlay et al., 2019: 3, 9). In England, partnership was never very widespread (Bacon and Samuel, 2017) and often lacked commitment from senior management (Bach, 2004).
In Norway, a major health reform in 2002, inspired by NPM principles, transferred ownership of hospitals from the counties to central government through a decentralised enterprise structure, subject to financial accounting principles similar to those in private companies (Neby, 2015: 1003). Five Regional Health Authorities (RHAs) were established (subsequently reduced to four), each with their own board and director, to manage and allocate resources to hospital trusts 5 on behalf of government. RHA and trust boards include three elected employee representatives, holding a minority of seats.
Union density in the government sector (including hospitals) is around 85% (Nergaard, 2022). The main collective agreement is the Basic Agreement between the employers’ association, Spekter, and the union confederations, including Landsorganisasjonen i Norge (LO). It covers the main conditions of service across the public sector, with sub-agreements specifically for hospitals that primarily deal with pay and conditions. Social dialogue is required at central, regional and trust level on a multi-union basis. The Basic Agreement includes principles of codetermination over organisational change and working conditions (Hovedavtale, 2021: 15). It also states that ‘the introduction and use of new technology and digitalisation’ must be discussed with shop stewards and that employees should have ‘real influence’, including in project groups (Hovedavtale, 2021: 16). While mechanisms exist to deal with employers that fail to follow the Agreement, questions remain over how far these participation principles apply in practice (Bie-Drivdal, 2021). Apart from one study which found that most shop stewards thought involvement happened too little or too late (Trygstad and Anderson, 2015: 29), there is little research examining union influence at different levels and across regions.
Research methods
Research was undertaken with two unions – UNISON in the UK and Fagforbundet in Norway. Both were selected as they represent the largest numbers of admin workers in hospitals, although they also recruit other groups, including nurses, cleaners, porters and catering staff. The biggest unions in their respective countries, UNISON is affiliated to the Trades Union Congress (TUC), and Fagforbundet to the main peak-level union confederation, LO. As predominantly public sector unions, over 70% of their members are women. They are also the largest unions in the health sector, which means their representatives often have key positions on committees and boards for joint consultation, partnership or social dialogue from national to workplace level.
The research primarily involved semi-structured interviews with national officers and regional and workplace union representatives (Table 1). It was important to include individuals from different levels to capture where decisions are made and how influence and involvement operates within the political sphere, governance structures and at the workplace itself. National officers (three in UNISON and five in Fagforbundet) were included who had a key role in the union’s policy on digitalisation or had responsibility for admin workers within the hospital sector. The research was conducted between June 2022 and April 2023. UK Conservative governments had been in power since 2010 (until July 2024). In Scotland, the Scottish Nationalist Party (SNP), 6 and in Wales, Welsh Labour, held office and continue to do so. In Norway, a Labour-led (Arbeiderpartiet) government had been elected in 2021, following a period of Centre-Right government.
Research interviews.
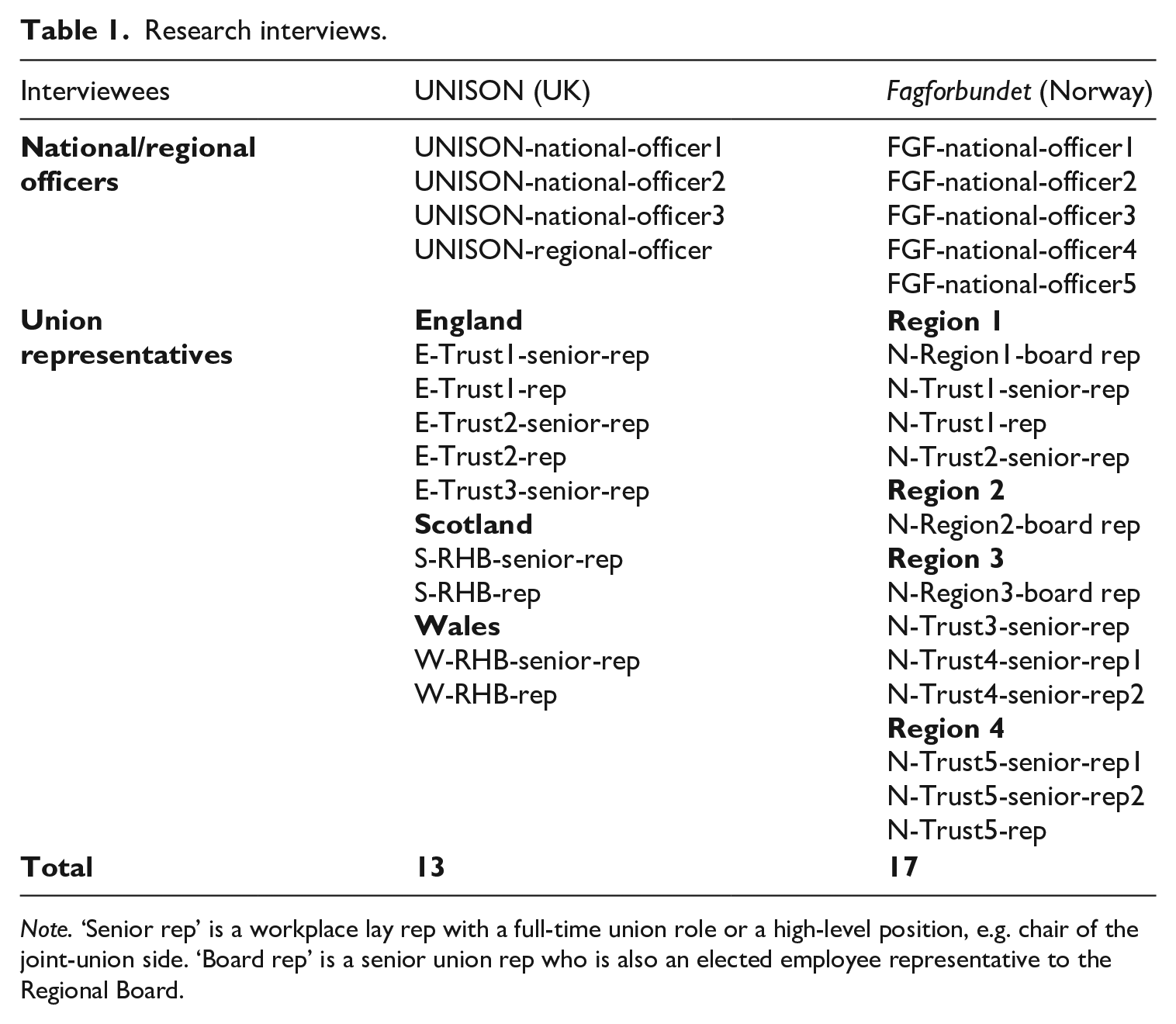
Note. ‘Senior rep’ is a workplace lay rep with a full-time union role or a high-level position, e.g. chair of the joint-union side. ‘Board rep’ is a senior union rep who is also an elected employee representative to the Regional Board.
The selection of the workplace cases sought to include at least one hospital in the UK and in Norway that might afford positive examples of union involvement and influence as part of a small sample of cases that could help to identify enabling and constraining factors. A key officer in each union helped to facilitate contacts with union reps at regional or workplace level. Due to the importance of the regional level in Norway, interviews were undertaken with Fagforbundet reps who were also employee representatives on three RHA boards. Workplace reps from five hospital trusts were included, which provided examples of ‘good’ and ‘challenging’ environments for union involvement.
In the UK, it proved more difficult for our key contact to identify positive examples in England. An RHB from Scotland was included, having been identified as an exemplar case. The senior rep interviewed had also held positions in the union at the Scottish level, allowing a comparison with governance arrangements in England. Unfortunately, we were unable to obtain interviews with reps at Welsh level, which limits the subsequent analysis. Along with the Scottish RHB, interviews were also conducted with workplace representatives in three trusts in England, and one RHB in Wales. Adapted discussion guides were used for interviewees with different positions in the union, covering their role in relation to the union’s influence and involvement in digital change. In total, 25 interviews were conducted online in English, involving 30 participants, 22 of whom were women and 13 were, or had been, hospital admin workers. All interviews were audio recorded, transcribed and anonymised.
The data analysis was undertaken primarily through a deductive approach, with codes developed from the research questions, theoretical framing and existing literature. These included items such as ‘formal structures of union involvement’, ‘use of legal rights’, ‘examples of involvement’ and ‘digital technology introduced’. Certain codes were only relevant for particular interviewees, for example national officers’ interviews included ‘influencing government’ and ‘union strategy towards digitalisation’. Some additional codes were created iteratively during the coding of the transcripts, such as ‘redeployment’ and ‘board level influence’.
Following the data coding, themes were identified that linked into the research questions. In relation to the first question on influence over initial decisions, themes included location of decision-making, the role of management attitudes at different levels, and examples of where involvement was considered successful or not. Across these themes, the analysis focused on exploring variation by country and workplace, along with whether differences in unions’ role could be linked to union power and institutional supports. It is important to recognise that the research is based upon union perspectives which are often overlooked in studies of digitalisation. However, we have to be measured in how we interpret these accounts when applied to the role of managers and policy makers.
Findings
The findings are structured around the two core research questions. The first section concentrates on interviewees’ perspectives concerning their role in initial decision-making around digital technology. The second section examines involvement and influence in the implementation process, drawing primarily on the interviews with union reps at the regional and workplace level.
Union involvement in initial investment decisions
Decisions on investing in digital technology occur at multiple levels, depending on the scale of the investment. Differences across Norway and the devolved nations of the UK in decisions over large-scale investments are presented in Table 2. In analysing the findings, we take each country in turn, focusing on the most important levels where decisions are taken, the extent of union involvement and examples of influence.
Locus of decision-making over large digitalisation investments.
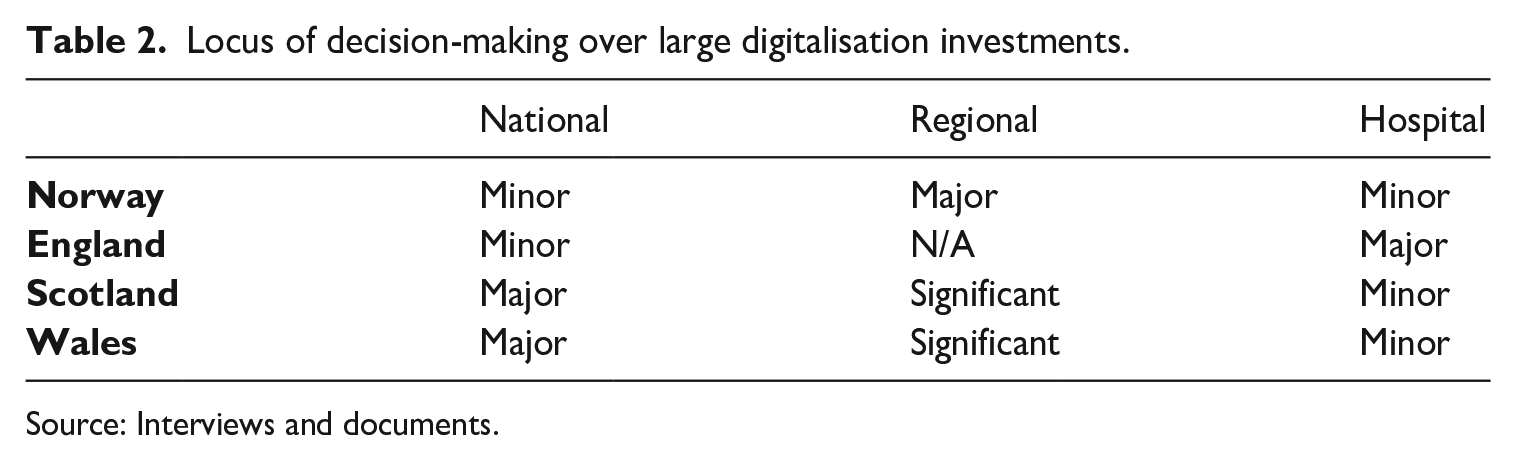
Source: Interviews and documents.
In Norway, the national government sets digitalisation policy in the hospital sector and the overall budget but does not make decisions over specific investments. National-level tripartism includes union membership of many advisory bodies and working groups on digitalisation (N-Region3-board rep). The political party in power was considered by union officials to be an important factor in their ability to influence national policy, while also setting expectations in relation to union involvement within the regions. The shift from a Centre-Right to a Labour-led government in 2021 had provided more opportunities for engagement and influence, reflecting the strong ties between LO and the Labour Party. Fagforbundet officers also emphasised their own influence through weekly meetings with the Ministry of Health where the union could exert ‘a lot of pressure’ (FGF-national-officer4). The Ministry was also said to be more willing to intervene with regional or hospital management if they were not following collective agreements (FGF-national-officer3). Importantly, the union could still exert some influence even without a Labour-led government. Under a previous Centre-Right government, Fagforbundet, in collaboration with other unions and interest groups, had successfully pressurised the Ministry to halt a national programme on digitalising patient records which was widely considered unworkable and expensive.
The Regional Health Authorities (RHAs) make the major decisions over investments in digital technologies and are, therefore, key targets for union influence. Norway was an earlier adopter of EMRs. Each RHA decides on the system for its hospitals, with the Norwegian company, DIPS, supplying three of the four regions (Green, 2018). The fourth region (Region4) was in the process of implementing a new digital health platform – ‘Epic’ – developed by a major US technology supplier. Each RHA is overseen by a board with members appointed by the Ministry, apart from the three elected employee reps which are typically from the doctors’ union, the nurses’ union and Fagforbundet. In addition, there are formal monthly meetings between unions and regional management as part of the collective agreement. As discussed below, these meetings outside the RHA board play a critical role.
The research revealed considerable variation across the regions in union influence over decisions to introduce new digital technologies. In Region3, relationships with management were described as very good, with a tradition of union involvement at multiple levels. Union reps insisted that they were involved in decisions over technology and placed particular emphasis on the regular meetings held with regional managers. Typically, management would suggest looking at digitalising an area of work and, together with union reps, would start a project group to develop proposals. Decisions over which technology to buy was, according to the Regional Board rep, made jointly with regional management. A union rep (N-Trust4-senior-rep2) explained that the RHA board authorises the final decision, where there is a ‘last chance’ for employee representatives to object if prior agreement has not been reached with regional management.
In the other regions, union reps appeared to have substantially less ability to influence decisions at the RHA level. In Region1, decisions were said to be ‘adjusted sometimes’, although there was ‘not very much dialogue in the board meeting’ (N-Region1-board rep). While projects could not be stopped, an example was provided of one that had been postponed. In Region2, the rep commented that the Board ‘listen to what we say, that doesn’t mean we win all the time’ (N-Region2-board rep).
In Region4, the planned implementation of the Epic EMR system across hospital and community services has been particularly fraught. The local workplace reps insisted unions had tried to warn regional management, citing known problems with Epic in Denmark, but the region ‘chose this system anyway’ (N-Trust5-senior-rep2). Technical problems following implementation have since seen general practitioners opting out and hospital doctors going on strike related to fears over patient safety. Mounting costs have plunged the main hospital in the region into financial crisis (Kommunal Rapport, 2023). Fagforbundet officers were extremely concerned about ‘Big Tech’ suppliers pushing through rapid digitalisation projects that left little time for effective consultation and local adaptation.
This consultant-driven process and also the involvement of the IT industry is very detrimental . . . the consultants are not really familiar with collective bargaining . . . [they want] centralised, standardised solutions which do not really fit our health sector. (FGF-national-officer5)
Unions lacked the power to prevent its introduction, while reluctant hospital trust boards were forced by the region to implement the digital platform, despite major concerns.
In England, government attempts to introduce a national patient record system between 2002 and 2011 were abandoned and subsequently assessed as being ‘expensive and largely unsuccessful’ (NAO, 2020: 6). Investment decisions now reside with individual trusts. While the Department for Health still produces targets to progress take-up of EMRs and offers some financial incentives, progress has remained slow. Around three-quarters of acute hospitals have adopted various systems but many lack the ‘interoperability’ needed to share digital records across health organisations (House of Commons, 2023: 7, 17). There is an English-level ‘social partnership’ forum which brings together unions, employers and government ‘to work collectively to tackle healthcare system priorities and challenges’. 7 However, UNISON officers reported no engagement over technology through this mechanism. This is perhaps not surprising as governments have ceded responsibility for digitalisation to trusts, while successive Conservative governments have been reluctant to engage with unions.
All three English trusts in the study had introduced some form of EMR system. Only one of the reps interviewed (E-Trust2-senior-rep) reported any involvement in decisions on investment, however, that was very limited. The rep referred to a ‘very forceful’, top-down approach that had become ‘dominant’ following a merger, where the CEO ‘saw it [the Epic system], wanted it, went out and got it’. Notwithstanding some initial engagement with unions and staff looking at alternative systems, as the process proceeded all but very senior managers were excluded, with only the doctors’ union involved ‘at the last minute’.
At the other two English trusts, there was no involvement beyond informing unions of forthcoming investments. At E-Trust1, union–management relationships had deteriorated under a new senior management team that was said to have little understanding of ‘the need for unions or what it is unions actually do’ (E-Trust1-rep). Major reorganisations and digital changes were rushed through without ‘meaningful consultation’ and ‘we keep being told when it’s happening rather than what do you think?’ (E-Trust1-senior-rep).
In Scotland and Wales, the national level is the most significant locus for investment decisions, although the region also plays an important role. Union involvement across the sector was viewed as better under a Labour government in Wales and SNP government in Scotland, with the latter seen as ‘very pro-dialogue’ (UNISON-national-officer2). In Scotland, larger-scale technology projects are decided at national level, with the government moving towards implementing standard digital record systems across the country. Smaller-scale changes could be decided within a particular region. A senior rep explained that national proposals are first discussed at the Scotland-wide partnership forum, a tripartite group comprising Scottish government, NHS managers and unions whose remit is to ‘work together to improve health services’.
8
Purchasing decisions are made by working groups with union involvement. Any digitalisation projects then go through the regional forum before filtering down to partnership forums at hospital level. A senior rep explained how they brought in local reps and involved them at an early stage through working groups:
If the [national] forum sets up a working group to deliver something, or introduce something, our health committee would look for local reps . . . who work in that area, who [have] a knowledge and an understanding of that. (S-RHB-senior-rep)
If management attempted to unilaterally introduce technology, the union would stop the process. Typically, as one rep stated: ‘a paper should be presented and then we would agree it; [otherwise] you start again’ (S-RHB-rep). Failure to follow partnership agreements could be taken up at the Scottish level and directly with government ministers.
The data suggest that Fagforbundet and UNISON have achieved meaningful involvement and influence in initial digitalisation decisions in the Scottish RHB and Region3 in Norway; however, this was not the case in the three trusts in England (see Table 3). The next two sections address the second research question concerning unions’ role in the implementation of digital technology at hospital level.
Union rep perspectives on their role in digitalisation.
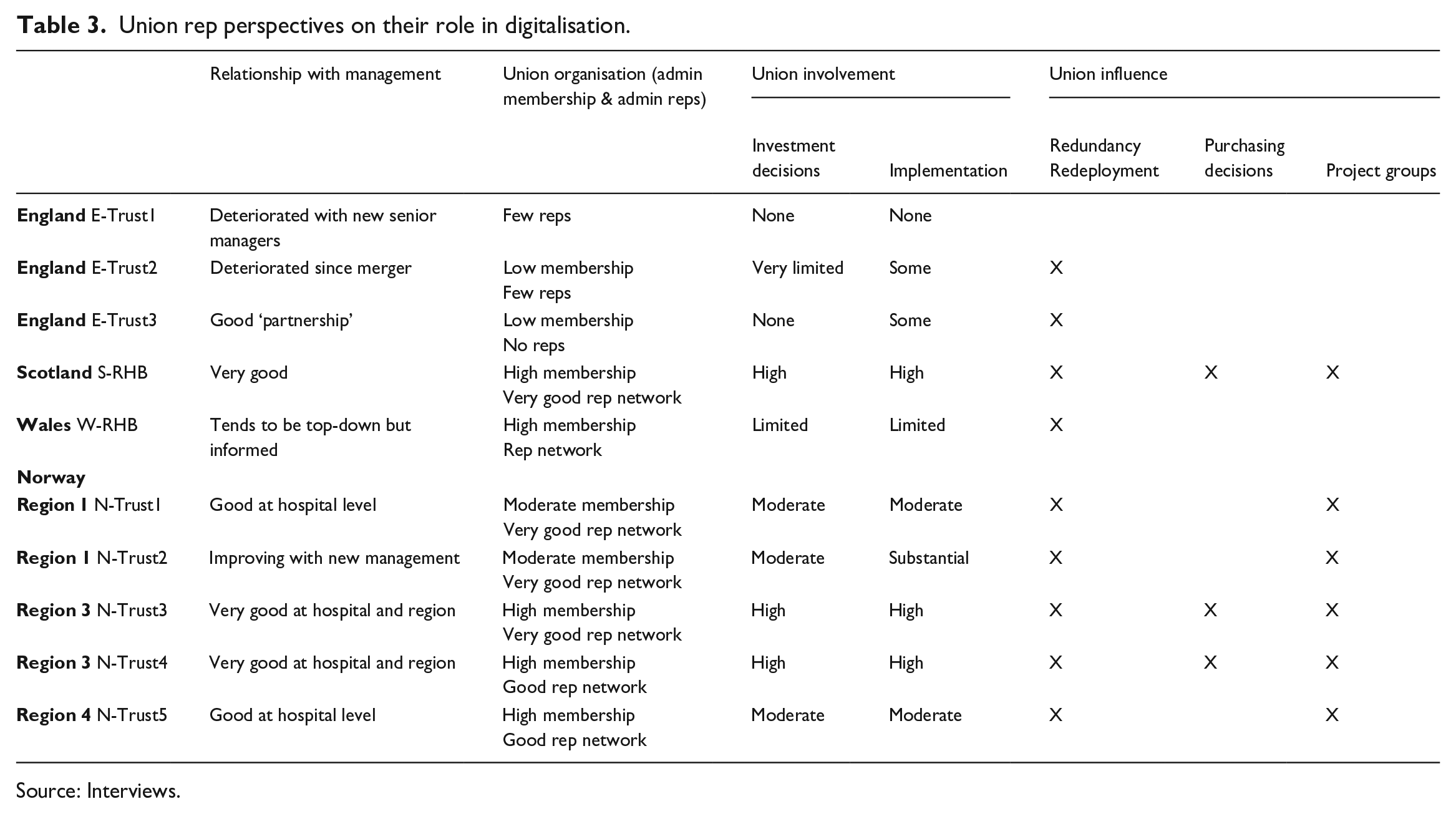
Source: Interviews.
Union involvement in implementation at hospital level in Norway
In Norway, union involvement in implementing digital technology at hospital level was variable. National officers stated that much depended on the attitude of the trust’s senior management towards unions, along with the approach of local union representatives.
We have some management, they really understood that this social dialogue is very important to get things done. But I also think that some leaders [managers] may see that . . . this really slows down the work. (FGF-national-officer3)
However, the same officer also noted that some union reps were ‘scared’ of dealing with digital change as ‘they don’t know enough about what is going on and may not be demanding to be involved’. An RHA board rep admitted a reluctance to engage in technical aspects, commenting ‘we don’t want to choose between companies [suppliers]’ due to it being ‘quite complicated’.
Some regional and hospital reps reported that greater involvement in the implementation process was underpinned by good relationships with management, reflecting long established practices of joint working that endured even with changes in senior management and union leaders. In Region3, where substantial involvement was reported at N-Trust3 and N-Trust4, reps also emphasised the continued importance of union strength to ensure the law and collective agreements were followed. One rep remarked:
They cannot do anything without the principal shop steward here in the hospital, they have the law . . . I told [the hospital director] once ‘if you’re having a dream, you have to have me in it’. (N-Trust3-senior-rep)
At N-Trust4, the senior rep had fortnightly meetings with the hospital director, who they could contact at any time, with the union ‘always invited . . . into projects’. The recent transition to a new EMR system had been overseen by a working group which met monthly:
We have a meeting about the system and how far we’ve come and what went wrong, do we have to stop a little bit and think, are we going to do this now or wait? . . . [Management] listen quite a lot actually, because they need the employees and the secretaries . . . to be really, really good at the job. (N-Trust4-senior-rep2)
The system had been piloted in one clinic over six months, allowing problems to be resolved before further testing in two other clinics.
In the other hospital trusts (N-Trust1, N-Trust2, N-Trust5), although there was some engagement with unions, reps referred to various problems that limited their involvement and influence in the implementation process. A principal concern was that the main decisions were taken at regional level where the unions had less influence, which could lead to standardised technologies being cascaded down. In Region4, the rep explained that with the impending adoption of Epic: ‘we’re not getting any information . . . it’s going to drop on our heads’ (N-Trust5-rep). Local reps were then left with limited ability to input their own and members’ views into how the systems might be used or what problems might arise. A workplace rep at N-Trust2 in Region1 spoke of ‘top down’ decisions with a ‘generic product’ being imposed that was ‘made for a different industry because it’s cheaper’.
At N-Trust1 in Region1, the senior rep reported ‘more influence and control’ over small changes within the hospital, such as automating patient reception. Union reps participated in project groups and management ‘listen to us a lot’. Another rep at N-Trust1, who worked as a secretary, was less positive, noting that admin staff were frequently ‘the last ones’ to be asked and were ‘overlooked most of the time’ (N-Trust1-rep). The rep linked this to their position in the status hierarchy compared with clinicians and nurses rather than to the feminised nature of admin work.
At N-Trust2, also in Region1, recent plans to move to a new hospital, including a vision of becoming ‘paperless’, had seen the union involved ‘every step of the way’. This included participation in project groups, such as one on handling patient data and another on the future of clerical work. However, given previous experience, there was scepticism as to whether this would amount to substantive influence.
Historically . . . I got the impression that it was already decided and you were just there to waste your time . . . you can talk and you can pray they will listen and take note the next time. (N-Trust2-senior-rep)
The rep reported that admin staff were anxious concerning potential job losses as, unusually for the public sector in Norway, 70 secretaries had been made redundant when digitalising medical records in 2009. However, within three months, those who wanted to return had ‘got their jobs back’ because the patient management system could not operate without them (N-Trust2-senior-rep). Although this experience cast a long shadow for workers, the rep considered redundancies were unlikely this time round. The new management showed a greater willingness to work with unions, while a more ‘hard hitting’ local union leadership would not ‘tolerate’ redundancies again. The result was that ‘we are being taken more seriously than we were for years’ (N-Trust2-senior-rep).
Union influence over job losses and task changes was reported in all of the Norwegian cases. Redundancies stemming from future digitalisation were considered unlikely by reps, with the strong expectation that workers would continue to be redeployed to other roles or acquire new tasks. Union reps spoke of assisting workers in this process and, in some trusts (N-Trust4 and N-Trust5), successfully pushing management to utilise the clinical skills of ‘health secretaries’, 9 particularly when other tasks were being replaced. Nationally, Fagforbundet is campaigning for their skills to be better utilised and is also part of a national commission on changing job roles in the healthcare sector.
Union involvement in implementation at hospital level in the UK
In the UK, union involvement in implementing digital technology was reported as being far greater in the Scottish Regional Health Board (S-RHB) than in the English and Welsh cases, reflecting the Scottish NHS’s model of institutionalised multi-level partnership working. S-RHB is strongly unionised and senior managers were said to have a positive view of unions. Referring to a recent decision to introduce a new patient ‘tracking system’, a senior rep explained that a working group had been established where union reps and relevant admin staff would ‘be involved in rolling the programme out’ (S-RHB-senior-rep). A local hospital rep also referred to a forthcoming pilot on voice recognition technology which would involve shop stewards and admin workers. Both reps reported that digitalisation was being used to reduce admin staffing levels, either through retirement or not replacing those who left. It was said, however, that management could overestimate the potential savings and the union had to keep ‘an eye on the management team’ to ensure staff numbers were not ‘below minimum level required to run the service’ (S-RHB-senior-rep).
In England, reps in two trusts (E-Trust3 and E-Trust2) noted that their involvement was restricted to dealing with redundancy, redeployment and regrading. At E-Trust3, the senior rep referred to a ‘positive culture’ of union and staff engagement, with unions briefed on plans to introduce EMRs at the Joint Consultative Committee. To avoid redundancies, the unions agreed to freezing vacant posts and only offering temporary contracts for jobs that could not be left unfilled. Over time these contracts had mostly become permanent, while the project had gradually ‘fizzled out’. In the senior rep’s view, this was because management realised ‘it was a much more complex and harder change process than they’d originally envisaged’.
At E-Trust2, the rep reported that although they had been consulted over the introduction of an Epic EMR system, they could only achieve small changes to new role descriptions and were excluded from the redeployment process. The senior rep explained that management ‘didn’t listen to us . . . some people were offered jobs that they probably would not be able to do and so therefore have left’. The result was ‘extra work’ for those who remained, leading to cases of stress and long-term absence.
At E-Trust1, where there was a general lack of consultation over digitalisation, the senior rep noted that the union just ‘had to deal with the fall-out’.
I’m noticing more and more . . . that they don’t actually involve the people that will be using it on the ground. (E-Trust1-rep)
Following the digitalisation of paper records, the senior rep outlined how the union had resorted to escalating certain issues, for example through grievances where management had failed to provide adequate training.
There was no evidence in England and Wales of union participation in working groups or pilots. Technologies were said to have been introduced too quickly without any adaptation to the local work environment and involvement of the staff affected. This invariably created problems. At E-Trust2, the rep reported that the grafting on of new systems to existing IT infrastructure had led to ‘chopping and changing between different software’ that did not link together, dictation errors with voice recognition technology, and patient letters repeatedly being sent out with incorrect addresses and phone numbers. Training at some workplaces (E-Trust1, E-Trust2 and W-RHB) was described as either non-existent or very limited, with workers having to learn by themselves or through supporting each other. In one instance, this was said to be ‘a six-minute YouTube video’ (W-RHB-rep). Reps referred to the impact on admin workers in terms of frustration, stress and enhanced workloads:
Staff obviously aren’t happy . . . especially because . . . it’s being thrust upon them, and they haven’t had any input. They’ve had no training, they don’t know what it’s going to look like . . . how they’re going to make it work? (E-Trust1-rep) People have been kicking up a fuss . . . ‘you didn’t factor this in’ . . . you needed someone who would be doing it day-to-day to work out any problems. (W-RHB-rep)
To summarise, the research identified patchy union involvement in the implementation process across the three trusts in England, mainly limited to the provision of information and consultation around redundancy and redeployment, with similar findings in the Welsh case. By far the best example was the Scottish RHB where union reps reported being involved in digitalisation projects from the outset.
Discussion
Both UNISON and Fagforbundet were actively seeking to participate in digital change and advance worker involvement. There are, however, discernible differences across workplaces in the levels of union participation and influence which belie a neat contrast between the UK and Norway. In the ‘best cases’, which were only found in Norway and Scotland, unions reported influence from initial decisions through to the implementation process, including involvement in project groups alongside admin workers. In the cases in Wales and England, unions were marginalised and had little role or influence. There were also other cases in Norway where the union was often actively involved but reps expressed limited ability to influence decisions and implementation. A few positive examples of union involvement in digitalisation in the public sector have also been identified in the literature but these studies remain quite broad brush (Leonardi, 2023; Voss and Rego, 2019). Responding to calls for ‘a more in-depth sectoral approach’ (Voss and Rego, 2019: 89), our study provides detailed insights into unions’ role from decision-making through to implementation.
What might explain the positive cases of union involvement in Norway and Scotland? In Norway, the national model of tripartite social dialogue frames an expectation that unions will be consulted over healthcare policy, allied to an institutional architecture within the hospital sector for union involvement. Fagforbundet is an influential actor in health policy, particularly when the Labour Party holds office. Similarly, Scottish governments have been committed to partnership working with unions since devolution (Bacon and Samuel, 2017; Findlay et al., 2019). The health unions are well organised and powerful actors with agreements in place that require unions to be consulted and involved in digital change. Fagforbundet reps appeared to have sufficient power to halt some projects at regional level as well as influence the implementation of digital technology within a number of hospitals. The one RHB examined in Scotland also provided positive examples of union influence that ranged from initial decision-making to implementation.
By contrast, the picture that emerges from the English and Welsh cases is one of the union having little role in technological change, despite specific negotiation and consultative arrangements being in place within the hospital sector. Notwithstanding some weak consultation exercises, union reps seemed to lack the power to secure involvement or influence and had no mechanisms through which to insist on union participation. Arguably, the then UK Conservative government’s anti-union stance encouraged hospital management in England to pursue a unilateral approach. The position in Wales is less clear. The Welsh Labour government has adopted a policy, and more recently legislation, related to ‘social partnership’ 10 that includes NHS Wales. There was no evidence that this approach supported union involvement in digitalisation at W-RHB, but further research is required to draw definitive conclusions. It is possible that other trusts in England and RHBs in Wales might provide examples of more effective union involvement. If so, UNISON officers were unaware of them, suggesting a wider problem may exist. In both the English and Welsh cases, notwithstanding a lack of involvement in digital change, some reps were still able to influence certain outcomes such as limiting redundancies, revising job descriptions and supporting workers in redeployment.
In Norway, there is considerable variation across the cases in union involvement and influence, despite strong collective and legal rights. These differences seem partly to reflect regional variations in management–union relations. In Region3, where positive cases were identified, interviewees referred to long-term constructive working relationships whereby involvement in change was seen as ‘normal’ and had simply been extended to digitalisation. How these relationships emerge is unclear but there are indications in the data that unions’ organisational strength is likely to be important. This is not just a matter of having high membership density and an active shop steward network but also requires an ability to enforce collective and legal rights, if necessary through worker mobilisation. As with the positive case in Scotland, there were examples where the unions had held up or reversed projects, which can act as a powerful incentive for management to involve them at an early stage. Securing similar union influence in other regions and hospitals in Norway appears challenging, despite sharing the same institutional-regulatory environment. Whether limited union influence in these cases can be attributed to lower levels of union power or less proactive reps is not possible to conclude from the data. However, there is evidence that embedded union–management relationships have been less conducive, and it is possible that political factors at regional or municipal level may have a bearing.
Consideration also needs to be given to the role of professional hierarchies and the difficulties this presents for lower-status admin workers to gain involvement in digital changes. While in some cases in Norway, admin reps commented that doctors and nurses were more likely to be involved, in England and Wales there was no evidence that other occupations or unions played a greater role. This is not to say, however, that the gendered nature of admin jobs and position in the hierarchy are not factors in management’s tendency to overlook the benefits of their input, given that these digital technologies are designed specifically to reshape their work. As noted earlier, this is despite female admin workers from UNISON and Fagforbundet often holding senior union representative positions, including on joint union bodies, within the hospital sector.
The findings also indicate that influencing digital change in hospitals is particularly challenging for unions due to the multiple levels at which decisions occur and the role of political and policy processes within the public sector more generally. Government approach remains critical, not only in terms of institutional structures and mechanisms for union involvement, but also for shaping the attitudes of hospital and regional management. The ability to appoint senior managers or trust boards is one mechanism a government can use to influence management and their approach to union involvement.
There are country differences in the role of central government and the power devolved to different levels within the health system which is likely to be echoed across a broader range of countries and in other areas of the public sector (De Vries, 2020; Simões et al., 2021). While hospital budgets, along with broad policy approaches to digitalisation, are decided centrally by governments in Norway and across the UK, the locus of decision-making with regard to major investments, such as introducing an EMR system, is varied. The level where decisions are made has important implications for where unions should focus their efforts and the extent to which strength and capacity at national level, as is more typical in the public sector (Schmidt et al., 2019), can effectively influence digital change at the workplace.
Conclusion
With little research addressing union participation in digital change in the public sector (Doellgast and Wagner, 2022; Lloyd and Payne, 2021b), the article has examined the role of two unions, Fagforbundet and UNISON, in public hospitals in Norway and the UK. Norway is generally seen to offer a more supportive industrial relations environment for union participation in digital change than the UK. This study, however, uncovers a complex picture regarding the role of these two unions in the digitalisation of hospital admin work, with the different hospital governance arrangements across the nations of the UK emerging as important factors.
The article makes three significant contributions to analysing the role of unions in digitalisation within the public sector. First, the variation in where decisions are made and the role played by politics adds a new dimension to existing studies of unions’ involvement in digital change which have largely focused on the private sector (Doellgast and Wagner, 2022). The findings suggest that the role of governance is of critical importance in terms of the level at which investment decisions are made and by whom, and how this can subsequently constrain or open up the options available to workplace actors. Decisions at national or regional level, while restricting the involvement of unions locally, are more likely to be subject to political influence (Johnson et al., 2021). This is potentially the case across the public sector (Schmidt et al., 2019) and affords alternative points of leverage that are limited in most areas of the private sector.
Second, the prospects for union involvement also need to be understood in relation to whether there are institutional supports and government backing for management to involve unions at these different levels. In part, this is about government policy and approach. Similarities between England and Scotland in terms of industrial relations institutions and union organisation in the sector suggest that changing the government’s approach to managing digital change is likely to be critical to enhancing union involvement in NHS England. It is also about the power wielded by unions – both past and present – to shape the institutional and policy environment (Jensen et al., 1995). While these supports are important for union involvement, the effects are uneven. Union activism and organisation in the workplace, and the relationships they are able to establish with management, are key to developing a more conducive context for influence. Lack of institutional and regulatory backing makes it difficult for even well-organised unions to obtain early involvement.
Third, the research suggests that in certain areas of the public sector there may be stronger linkages between digital systems working effectively and job quality. While there is evidence of large-scale digital technology failures in the private sector (Flinders, 2024), in the hospital context this can be a matter of life or death for patients (Barbour and Wright, 2024; Clark, 2024). More frequently, system failures compound already increasing workloads as workers battle against them to keep services functioning. These closer links between workers and ‘customers’ in the public sector may provide additional pressure from workers for unions to be involved in the process.
Notwithstanding high levels of unionisation and established mechanisms for collective bargaining and consultation, top-down digital change (Voss and Rego, 2019) is certainly alive and kicking for many working in public sector hospitals in the UK and Norway. Fuelled by ‘Big Tech’ companies intent on selling lucrative IT ‘solutions’, the ability of unions to counteract this narrative, or intervene at an early stage, remains challenging. How can unions respond? Unions can actively campaign to ensure that patient data are kept secure and not sold off to private companies. Fagforbundet and other Norwegian unions have been very vocal in highlighting mass data breaches caused by outsourcing to foreign multinationals (Geard, 2017). Union education and training programmes remain vital for expanding and sharing officers’ and reps’ knowledge of new digital technologies, including their potential benefits, pitfalls and alternatives. Strengthening unions’ ability to resist or shape their introduction and use will also require ordinary members to understand their implications if they are to be mobilised in support of union proposals. Again, the union can play a key educational role. Strategies for shaping digital change that focus exclusively on the workplace, however, are likely to be limited without voice and influence at higher levels of governance.
While this article offers important insights from a union perspective, it relies on union reps and officials reporting their experiences. Further research that includes managers, policy makers, tech developers, public pressure groups and other unions would offer a fuller account of unions’ role in digital change and why differences emerge. It would also be valuable to explore the relationships and tensions between different unions within the hospital governance context when technology is introduced. With digitalisation seen as central to modernising public services, unions have a critical role in contesting these developments and pushing for greater union and worker involvement. This article has uncovered some positive examples that unions can build upon, notwithstanding the challenges that continue to exist.
Footnotes
Acknowledgements
The authors would like to thank those in Fagforbundet and UNISON who generously gave up their time to contribute to the study, Dr Jose Secki for his support in undertaking the data collection, and the two anonymous reviewers for their helpful comments on earlier versions of this article.
Funding
The research was funded by the Leverhulme Trust (RPG-2019-275).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.