
Abstract
Managing sexual and reproductive health (SRH) needs remains a challenge for many women migrant workers in developing countries. Nonetheless, the extent to which they can be supported in meeting these needs remains underexplored, with implications for worker health and working life. Drawing on semi-structured interviews with 25 factory women migrant workers in Penang, Malaysia, this article applies a Foucauldian lens of governmentality to explore directly their agency in managing their SRH. The authors consider the self-surveillance practices the women adopt in response to a programme of SRH interventions. The findings reveal varied degrees of compliance with programme expectations. The article demonstrates empirically the importance of the perceived salience of SRH as a motivating force in self-surveillance practices, drawing out the disempowering effects of self-consciousness and shame in gendered subjectivity. The authors further consider the impact of universalist prescriptions for SRH within locales in the developing world, and the implications for SRH interventions with factory women migrant workers in such settings.
Introduction
Rapid changes in global social and economic conditions have encouraged increasing levels of migration as individuals seek better employment prospects outside their home countries. This is particularly evident within South East Asia. In 2019, it was estimated that intra-regional migrants made up over 92% of the migrant population in the region (Capaldi, 2023). Women’s migration has far-reaching implications for their health, including sexual and reproductive health (SRH). The extent to which women migrant workers in these countries are able to manage their SRH needs is important. We draw attention to the challenges that they face in managing their SRH below. An equally important question is the extent to which they and their advocates are able to influence workplace practice to support these needs. What would interventions or practices to support their SRH needs look like?
Development initiatives are an important vector for global reproductive health rights. Yet, the priorities embedded in them have long been determined within developed settings (Alfonso and Korten, 1981), reflecting universalist, global aspirations. Programmes informed by Sustainable Development Goals (SDGs) thus frame ‘appropriate’ and ‘modern’ SRH practices (Ginsburg and Rapp, 1995), promoting a standardised model. Abstracted from socioeconomic, political and cultural contexts and realities in the developing world, the unintended consequences of such programmes may reinforce existing inequalities (Chan, 2022). All programmes require local enactment, their effects being a function of the agency of those involved. Evidence of the unintended consequences of SRH programme implementation in fertility (Maternowska, 2006) and reproductive health (Smith-Oka, 2009) signals the importance of local contours in programme design and delivery (Chan, 2022). It is important that the sociocultural contexts which shape women’s SRH practices are considered, to ensure that services are designed to be both safe and accessible (Agu et al., 2016; Metusela et al., 2017). Smith-Oka (2009) provides valuable insights into instantiation processes in the context of SRH programmes, exploring ethnographically the inscription on indigenous women’s bodies of population-based SRH policies in Mexico. Tracing the interplay between population policies, development programmes and medical practitioners, her analysis reveals the choices and strategies adopted by women in the face of institutional constraint. Her sensitive ethnography draws attention to the dynamics between local religious and social identities which may preclude programme adoption (Manderson and Whiteford, 2000), or the creation of moral selves congruent with programme expectations (Laveaga, 2007).
In this article, we apply these concerns related to identity and creation of moral selves to the experience of factory women migrant workers in Malaysia in receipt of SRH interventions informed by international SHR standards.
Women migrant workers form a large social group within the Association of Southeast Asian Nations (ASEAN). Of the 10.1 million international migrants living in ASEAN’s net destination countries, 7.1 million are intra-ASEAN migrants. Women make up 48% of intra-ASEAN migrant workers, an increase of 2% from three decades ago (ASEAN, 2022). 1 The challenges facing women migrant workers in managing SRH within ASEAN are well documented. Within South East Asia, the evidence suggests that these needs remain unmet; women migrant workers contend with many barriers preventing access to SRH care and support in their host countries. In Thailand, migrant workers exhibit lower levels of knowledge of SRH than local workers, likely to cause reproductive health problems (Khamthanet and Suthutvoravut, 2020). Women migrant workers in Industrial Zones (IZs) in Vietnam experienced barriers when attempting to access SRH services, including inconvenient clinic opening times, the distance of clinics from their work location and prohibitive costs (Ha et al., 2023). Female migrant workers in Cambodia are reluctant to use modern contraception methods, incurring higher risks of unwanted pregnancies; resulting in a need for comprehensive abortion care and contraceptive counselling (Masuda et al., 2020). In Laos, young female migrant beer promoters seldom use contraception, deferring to their male partners’ preference for not using condoms. They are often also subject to sexual harassment within this sexualised environment. Poor contraceptive practices result in sexually transmitted infections (STIs) and unwanted pregnancies (Sychareun et al., 2022). Yet, little remains known about the long-term health needs of temporary migrant workers in East and South East Asia (Turnbull et al., 2023). Elsewhere, research is only beginning to uncover ways in which workplace hazards within the oil, gas and mining industry (Razafimahefa et al., 2022) and manufacturing sector (Patangia et al., 2023) affect women’s SRH.
Malaysia offers a unique site for our investigation for two reasons. First, it is one of the largest migrant-receiving countries in South East Asia, where they provide cheap labour in manufacturing, hospitality and construction (IoM, 2023). The significant proportion of its migrant workers are from Indonesia and Bangladesh, but also from the Philippines, Myanmar and Vietnam. The women in our study are from Indonesia and Vietnam. Second, the dominant religion in the country, shared by many migrant workers from Indonesia, creates a particular moral context that may militate against effective SRH initiatives. Indeed, within Malaysia disciplinary discourses of ethnicity and sexuality underpin national migration narratives – and migrants must negotiate these discourses in order to resist the bodily inscriptions to which they are subjected (Hilsdon and Giridharan, 2008). Women migrant workers’ SRH needs in Malaysia are severely neglected in policy and practice (Loganathan et al., 2020a; Miles et al., 2022). Their cultural diversity, and the institutional contexts within which they are embedded, require sensitivity in addressing their SRH needs (Devadason and Meng, 2014). Adoption of the analytic lens of governmentality (Foucault, 2007) enables us to consider the extent to which their agentic responses were informed by processes of regulation and the power–knowledge nexus in context. Such analysis draws attention to the extent to which women engaged with the interventions in the manner intended, and the motivating force behind their self-surveillance practices. Considerations of the degree of the women’s engagement in such initiatives are crucial for researchers interested in improving the women’s quality of working life. How advocates (e.g. NGOs, unions) can exercise influence to accommodate women migrant workers’ SRH needs is also of critical concern (Miles et al., 2022). We explore empirically the extent to which an intervention designed to extend influence over the workplace to enhance SRH care was able to do so, drawing attention to the choices exercised by programme recipients.
Governmentality: Regulatory power and surveillance
Foucault rejects the idea that power is wielded through domination, instead framing power as dispersed and pervasive within modern society. He observed that the surveillance systems of prisons, mental hospitals and schools were not rooted in force or violence – on the contrary, those subject to these institutions undertook it upon themselves to behave in expected ways (Foucault, 1980b). A central concern here is the notion of a subject constituted by exposure to surveillance, the normalising expectations of behaviour and disciplinary regimes (Foucault, 1979). Regulatory power provides an efficient means of control, extending pervasive influence through self-surveillance. It requires discipline (Foucault, 1980a), through which power relations are inscribed on the body.
Foucault introduces the neologism ‘governmentality’ to convey the processes by which self-surveillance operates within governance regimes. Governmentality is generative, to the extent that it creates subjects who freely choose to comply with requirements, removing the need for compulsion. Governmentality thus relies on self-surveillance by the subject (Fleming and Spicer, 2014), such that personal ambition is shaped to be consistent with external requirements. At its core, governmentality consists of three inter-related processes (Foucault, 2007). The first requires creation of a series of ‘taken-for-granted’ practices: an amalgam of existing procedures and expectations together with reflections on their value and use. Such practices are thus culturally situated and not simply ‘invented’ out of nothing (Foucault, 1997). The second process concerns the use of knowledge within a power–knowledge nexus comprised of actors within state and professional institutions. The third and final process concerns development of technologies of the self which constitute the personal identities of the governed (Foucault, 1982). This draws attention to the active construction of ‘selves’ by actors – an endeavour in which agents become ‘entrepreneurs of their selves’ (Cooper, 2015). Governmentality operates in the interplay between the three processes above, binding the ambitions, projects and creativity of agents to institutional requirements (Clegg, 2019).
Limitations of governmentality – the role of emotion/affect in self-surveillance
Foucault’s abstract formulation of the subject is curiously silent on the nature of disciplinary practices which produce gendered subjects (Bartky, 1988). It lacks consideration of what women feel about such norms; the extent to which self-surveillance and normalisation processes are experienced as differentiated rather than totalising; and the degree to which women are docile or active in relation to discipline (Deveaux, 1994).
Such abstraction of (de-gendered) agents in networks of power relations fails to adequately theorise women’s internal, subjective experience of power (Held, 1991). Such experiences may manifest in the disempowering effects of self-consciousness, shame and/or unreciprocated emotional care (Bartky, 1991) – the experience of which is gendered. Foucault’s failure to consider such internal obstacles to agency thus offers an inadequate model of female agency (Deveaux, 1994; McNay, 1991). Any adequate feminist analysis requires due consideration of women’s subjective experience of power, informed by dynamics of self-actualisation, to explore possibilities for resistance and change through individual and collective endeavour.
Below, we outline the three interrelated processes of governance in the context of SRH interventions with women migrant workers in Malaysia, i.e. the ‘taken-for-granted’ amalgam of existing procedures and expectations; the contested power–knowledge nexus of actors within state and professional institutions; and the technologies of the self which constitute the personal identities of the governed. We explore the first two processes by drawing on political economy, healthcare and feminist literatures, and policy documents. We explore the third process empirically, in an original qualitative analysis of narratives in interview data with women migrant workers in receipt of a suite of SRH interventions detailed below. We explore the subjectivities revealed in their narratives, in the context of the SRH governance systems within which they are embedded.
Existing procedures and expectations
Malaysia’s migration regime is intolerant of the SRH needs of women migrant workers (Loganathan et al., 2020a). These women are subject to two phases of health screening to certify that they are healthy and free from dangerous or contagious diseases prior to employment. Pregnancy is a breach of work permit conditions, rendering them liable to deportation (Immigration Department of Malaysia, 2021). Employers are legally required to report pregnancies to the government. In many cases, women migrant workers who become pregnant run away and become undocumented (Loganathan et al., 2020b). Others resort to dangerous means of terminating their pregnancies (Loganathan et al., 2020a).
Women migrant workers lack access to SRH care. The high cost of healthcare, the inconvenient location of health institutions and discrimination by healthcare providers against migrants all reduce the ability of women migrant workers to manage their health needs. Language barriers discouraged access to healthcare. Migrant populations are thus unreached by national SRH programmes (Lasimbang et al., 2016; Loganathan et al., 2020a). Tan (2020: 611) recently noted that in Malaysia, care was unambiguously delimited by nationality. Access to care by foreign workers and refugees was a risk, leading to arrest, either for being illegal or for being unable to pay medical bills.
Secondly, access to several SRH services remains a low priority in Malaysia’s universal health coverage plans. The level and extent of prioritisation are influenced by its sociocultural and religious norms (Lim et al., 2020). These values dictate that SRH is taboo and shameful, and set moral injunctions on behaviours considered acceptable. Sexual relations before marriage are considered unacceptable, and unmarried women and young women who fall pregnant face barriers in accessing pregnancy and safe delivery services (Huang and Lim, 2018). Social cultural norms which regard abortion as immoral affect the decision making of medical practitioners (Huang et al., 2013). It is argued that expanding SRH rights to women requires more than simply technically expanding access to these services: a move from a technical to an empowering approach that addresses patriarchy and heteronormativity is required (Sciortino, 2020).
These values and practices run counter to those encoded within international SRH standards, which place SRH rights at the heart of development. International SRH standards prescribe that, at a minimum, women will be able to access SRH information; access affordable and acceptable contraception methods of their choice; be empowered to protect themselves from STIs; and have the right to make informed choices about their SRH (Table 1).
Attributes of women required to obtain good SRH (idealised ‘selves’).
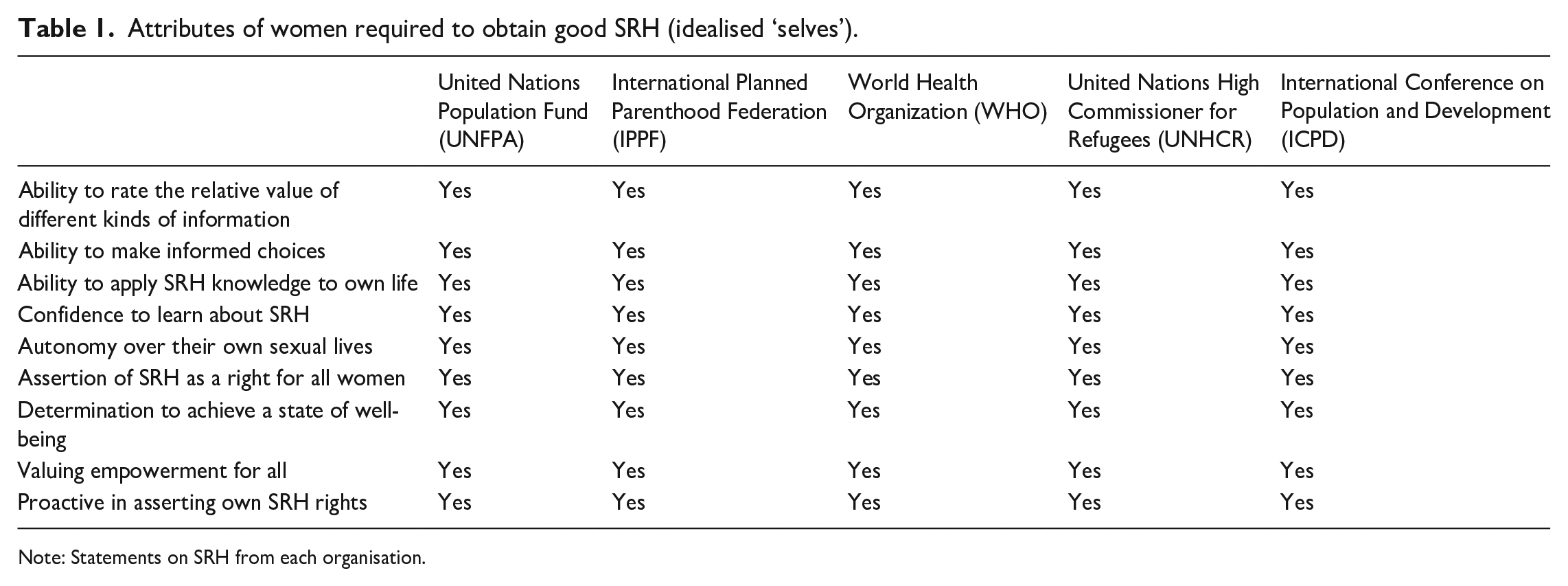
Note: Statements on SRH from each organisation.
Power–knowledge nexus of actors within state and professional institutions
The second process concerns the use of knowledge by actors within state and professional institutions within a power–knowledge nexus. This process mediates between regulatory requirements, and the self-regulation of individuals subject to such regulation.
Clinical knowledge is embedded in power relations. In Malaysia, one important group of actors are those clinicians who administer tests which verify the SRH status of women migrant workers on behalf of the government. The Foreign Workers’ Medical Examination Screening System (‘FOMEMA’), an organisation appointed on behalf of the Ministry of Health, screens women migrant workers for multiple conditions, including HIV, syphilis, breast abnormalities/swelling, malaria, tuberculosis and pregnancies (FOMEMA, 2023). Failure of screening tests results in deportation, and those who pass are re-screened each year for the first three years of their stay, then every alternate year up to a maximum of 10 years. Also, clinical services may be denied to women migrant workers who often cannot afford the full cost of healthcare. Although they may rely on the mandatory ‘SPIKPA’ Foreign Workers’ Health Insurance Protection Scheme which covers some medical costs, such cover is limited (Lim et al., 2020). Factory clinic staff, as well as off-site hospital staff, are required to report pregnancies and other SRH conditions which affect the ability of women migrant workers to work (Loganathan et al., 2020a). Unfitness to work renders women migrant workers liable to deportation. It is also well documented that hospital staff may discriminate against migrants by withholding services (Loganathan et al., 2019).
Conservative cultural and/or religious mores related to SRH and embedded within patriarchal values may be upheld – including by women migrant workers themselves. Women migrant workers subscribing to conservative values may report others who are pregnant, as extra-marital sex transgresses such mores. In this way, unmarried women may be ‘policed’ by their married counterparts, older women exerting moral authority over younger women. Shell-Duncan et al. (2018), for example, demonstrate how older women are steadfast guardians of tradition, using their power to perpetuate the tradition of female genital mutilation/cutting in Senegambia and resisting those who challenge the practice.
A final group of actors are the representatives of NGOs, who organise and deliver services congruent with international SRH standards. They do so in an environment inimical to women migrant workers’ SRH needs. Many have collaborated to lobby the government to change laws and protect the SRH needs of migrant workers in the country. Prominent NGOs include the Reproductive Rights Advocacy Alliance Malaysia (RRAAM), Asian-Pacific Resource and Research Centre for Women (ARROW) and Penang Family Health Development Association (FHDA). Collectively, these actors make a strong moral case for SRH self-actualisation, running counter to the moral agency implied in conservative sociocultural and religious norms.
Technologies of the self
The third and final process concerns active construction of selves by actors, in dynamic relation to both existing procedures and expectations, and the power–knowledge nexus of actors within state and professional institutions. This is a creative and generative process, in which actors are ‘entrepreneurs of their selves’ (Cooper, 2015). We explore these dynamic constructions through analysis of narratives within semi-structured interviews with women migrant workers in receipt of a suite of SRH interventions, presented below.
Methodology
The data here reported were collected as part of a research study funded under the British Council Newton Fund Impact Scheme (grant #536753284) in which we implemented three interventions in two factory sites to support the SRH needs of women migrant workers. Our interventions were informed by a prior literature review, identifying education, access to healthcare and counselling and support services as critical in supporting these needs. Our interventions comprised education on reproductive hygiene, anatomy, contraception, urinary tract infections and menstruation; a mobile clinic operating as a well-women clinic offering blood tests, pap smears and general information on SRH; and a counselling and referral service for more complex SRH conditions through the medium of ‘Facebook’ and a hotline number. Our analysis draws on 25 interviews with women migrant workers in the factories. They are documented workers, authorised to enter the country and engage in paid work. Data were collected between October 2021 and January 2022.
Women migrant workers were selected by collaborating factories to participate in the interventions, or else volunteered to do so. The two participating factories are from the electronics assembly sector within Penang, Malaysia, which is heavily reliant on migrant labour. In both factories, women migrant workers comprised at least 50% of the workforce. We secured full cooperation from the two factory sites by working closely with factory HR personnel.
Women migrant worker interviewees were of Vietnamese or Indonesian heritage, and received a small honorarium. Table 2 presents an overview of the participants’ characteristics. Due to the sensitive nature of the topic, interviews were conducted only by female members of the research team. All of the women interviewed had education up to secondary school level. Members of the research team spoke Bahasa Malaysia, a language familiar to the Indonesian women. Interviews with women from Vietnam were conducted in Bahasa Malaysia or English, depending on their preference. Women migrant workers were fully briefed on the purpose of the research and invited to ask questions to clarify their understanding. Interviews were all conducted online, due to Covid-19 restrictions in force at the time. Ethical approval was granted by the ethics committee of one of the authors’ university.
Demographic characteristics of women participants in the study.
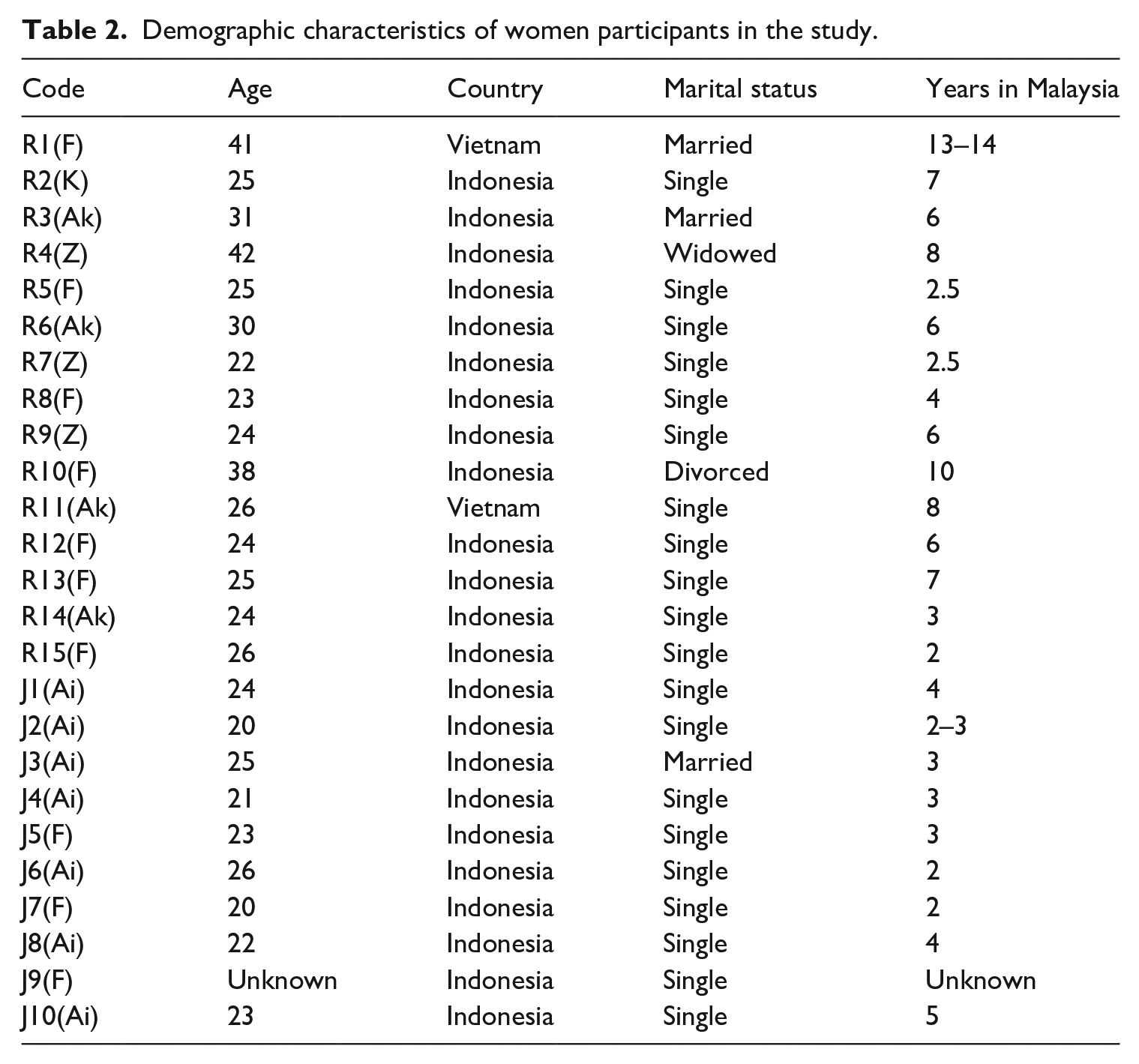
The interview schedule included questions on the benefits of each of the interventions; any improvements that women wished to make to them; and what (if any) impact the interventions had on their SRH knowledge, attitudes and/or practice. Interviews were recorded, transcribed and analysed thematically (Braun and Clarke, 2006) to surface narratives related to the ‘selves’ that they formed in response to the existing procedures and expectations regulating SRH and the power–knowledge nexus that they are embedded in. The data are available on reasonable request from the lead author.
Findings
Our findings reveal three narratives drawn on by interviewees in constituting their ‘selves’ in response to the complex governance environment in which they are embedded: Progressive; Conservative; and Passive. We elaborate each in turn below, reporting data segments typical within each narrative.
Progressive self
This narrative is consistent with the idealised moral self, envisaged within international SRH standards (Table 1). This includes feeling confident to engage with SRH needs; applying learning to practice; and valuing empowerment for all women.
Feeling confident to engage with SRH
Women informed by a progressive narrative developed a sense of safety, confidence and trust sufficient to allow them to engage with programme health providers and address their SRH needs. Women appreciated the respect shown to them by the doctors. These interactions led to ongoing contact with healthcare providers – an important factor in women’s ability to manage SRH over time: I did not visit any doctor in Malaysia, only in Indonesia [because] I am afraid of how to interact with doctors, are they going to serve me well? Because I am a foreigner. But now that I have visited [the clinic], the service is very good; the doctor listens to me and they will give advice . . . They explain, and treat me well. So, I think if I have any health issue, I will just refer back to [them]. [J3(Ai)]
Applying learning to practice
Women demonstrated a curiosity about SRH which enabled them to change their existing practice. The educational intervention improved knowledge of women’s anatomy, the relevance of contraception and the importance of breast self-examination/cervical smears: For the education programme, I benefitted a lot from this, especially ways to use condom, breast self-examination . . . for my own health. Previously, I had no idea about what was within my body, what was SRH. Now at least I know the shape of my vagina, and how to perform breast self-examination. [R2(K)] . . . you have to use a condom, then throw it away. You can’t have [unprotected sex]. Don’t get the HIV virus. [J5(F)] Before this, I thought the condom is like a dangerous thing . . . but after I listened to the lecture, now I know we need to wear it to prevent STIs. [J6(Ai)] I practise breast self-examination once a month, following what was taught by the service provider . . . [J5(F)] I also experienced the Pap Smear check for the first time, I have never done it before. In the beginning, I was very shy but later I thought I should just do it, so I can get early detection and get treatment. [R1(F)]
In addition to changes in practice related to their own bodies, women also indicated a new attitude towards their relationships with their partners, including deciding when to have a family, and the unacceptability of sexual coercion: Husband and wife are not obliged to have children. When you’re married, it’s okay if you are not planning to have a child, you are not forced to have a baby. [J5(F)] We must be mutually happy, no coercion. There must be communication with each other, so that the relationship is harmoniously maintained . . . There is one friend, she was always abused by her partner, so told her how to communicate; before sex, there should be communication, don’t let any violence happen . . . Afterwards, she explained to [her] partner . . . In the past month she said that her partner understood, and is no longer forcing her to have sex. [R4(Z)]
Valuing empowerment for all women
Interviewees shared their new knowledge with family and friends: My friend is also Vietnamese. She wasn’t sure what a pap smear was so I explained to her. I told her that I wanted to do a pap smear and explained to her what it is about and she agreed to also . . . [R1(F)] I told my three [close] friends . . . I shared that in having sex, we have to take precaution, and not just jump in and do it, we don’t know of any diseases the boy may transmit to your body, so I shared the purpose of condoms. [R7(Z)]
The agency reflected in this narrative enables the accumulation of knowledge and adoption of practices necessary for women to control their fertility, avoid STIs and ensure their continued fitness to work – while simultaneously allowing for sexual expression. The subjectivity reflected in the progressive narrative is consistent with the ideal self, underpinning SRH standards while at the same time enabling women to comply with migration regime requirements to avoid pregnancy and STIs.
Conservative self
Within this narrative, marriage confers entitlement to specific forms of SRH knowledge and associated practices – an entitlement denied to unmarried women. Our interventions were delivered to mixed groups – of 25 interviewees, three were married, one widowed, and one divorced. As conservative sexual mores ascribe very different expectations of SRH behaviour to married and unmarried women, interventions in which these two groups were combined provided a site in which these expectations unfolded. We consider the behavioural expectations of married and unmarried women in sequence below.
Behavioural expectations (married women)
Some married interviewees were conservative in their expectations of how women should behave. They drew distinctions between the types of knowledge – and by implication behaviours – considered appropriate for married and unmarried women.
One educational component included discussion of the benefits of contraception and a demonstration of the application of barrier methods on anatomical models. Access to such knowledge was considered taboo for unmarried women by some interviewees. Specifically, objections were raised about unmarried women being in the same class talking about contraceptives. One married interviewee stated that: . . . the doctors show the genitals in explaining how to insert contraceptives into the vagina [female condom] . . . That’s kind of disgusting right? A little bit shy . . . if I can suggest maybe a separate programme for those who are married and unmarried. Not everyone who joins is married. Not everyone already has a partner. [R3(Ak)]
The implication is that certain types of SRH knowledge are inappropriate for unmarried women. The married interviewee believed that she had a right to police this boundary. This perception arose in the context of cultural beliefs that unmarried women are ‘little sisters’, i.e. that they are to be protected from engaging in sexual relations until they are married. The inclusion of both married and unmarried women in the same learning environment provided the context for disapproval to arise.
The importance and exclusivity of the marriage bond is such that the invasive nature of pap smears may even be experienced by married women as embarrassing – the body is owned by the husband and not for sharing: So, I have a [sexual] relationship just with my husband only, I never see a doctor for a check . . . So, I do feel a little embarrassed. [R3(Ak)]
The implication here is that there are limitations to the entitlement afforded to married women. While marriage confers certain privileges in relation to SRH knowledge, marriage also restricts the willingness of married women to share their body with healthcare providers.
Behavioural expectations (unmarried women)
Another element of the conservative narrative reflects the reluctance of unmarried women to reveal concerns about their vaginal health to others, as discussion of vaginal health may be interpreted by others as evidence of promiscuity: . . . for example, checking vaginal health . . . sometimes there are those women who, sorry to say, aren’t married but are sexually active . . . these women want healthcare providers to check their vaginal health, but are embarrassed because [in fact] they are still single, so I’m afraid they did not get themselves checked. [R10(F)]
Differences in the perceived relevance of information by marital status were also reflected in the narratives of unmarried women. This may be clearly seen in the following extract, in which R9(Z) – who is 24 and unmarried (Table 2) – explained that lessons about abortion were not relevant to her because unmarried women do not get pregnant: INTERVIEWER: But do you know about safe sex? Do you remember? Have you learned any of that knowledge from the programme? R9(Z): What knowledge? About the abortion? No, it has no relation to me.
R3(Ak) – a married participant – noted that unmarried women may be inhibited from asking questions about contraception because they fear that this would be frowned upon as they are unmarried: . . . there are some women who are not married . . . they are interested in knowledge about sexual health, but are reluctant to ask questions because they don’t want to be judged negatively by their peers, as their peers know they are not married . . . those who are strongly religious may also not want to ask such questions until they are married.
To avoid stigma, unmarried women wait for married women to ask the very questions that they themselves want to ask: The unmarried ones are kind of shy, but keep listening, because the married ones dare to speak up. The unmarried ones don’t dare to ask, but listened until the end. So, they were able to learn in the end. [Unmarried women] . . . dare not speak up because they don’t want to be judged. [R3(Ak)]
While the subjectivity reflected in the conservative narrative is congruent with migration regime expectations with regard to avoidance of pregnancy and STIs, it contrasts sharply with the ‘empowered woman’ envisaged by international SRH standards. The traditional mores embedded within this narrative hamper unmarried women from developing the types of SRH knowledge, attitudes and practices which would empower them in the manner encoded within international standards.
Passive self
A third narrative indicated a passive construction of subjectivity with regard to SRH. This narrative indicates the importance of following directions from authority figures – supervisors, labour agents
2
and programme service providers. Supervisors and labour agents were responsible for work planning/shift patterns. Without their permission, these women felt that they could not participate in the programme: . . . [some] supervisors would permit, others, wouldn’t. [R4(Z)]
Even when granted access to the programme, women were unable to engage with the content to draw out meaning for themselves. This runs counter to the model of agency anticipated under international standards – rather, women attended because they were directed to do so by their supervisors, without necessarily understanding the nature of the programme: The agent told me [as part of the programme] that we are going to have a check-up at clinic. So, I asked why, because I don’t have any health issues . . . he told me that we will have an interview with the doctor. That they [the programme providers] are going to teach us something. So, I just agreed. [J4(Ai)]
Once inside the classroom, many women indicated a passive orientation to the educational sessions; not wishing to interrupt the tutors, or inconvenience their peers by taking up time within the session to explore their own questions. Given the narrow window for delivery of the educational component agreed with the factory, women were reluctant to interrupt as they were aware of the time constraints. R1(F): We’re afraid we might drag their time by asking so many questions. We felt that we might disturb the flow for the others. So, we are a little [nervous] . . . Interviewer: So, you do have questions but you are too afraid to ask and that you might take too much of their time? R1(F): For me, if we keep asking we’ll be disturbing. INTERVIEWER: Disturbing the trainers or the participants? R1(F): The trainers. Them too including the operators. Their supervisors only let them out for one hour so they can’t afford to stay much longer. So, I don’t want to be of inconvenience, disturbing people.
Similar passive behaviours were exhibited within the clinic setting. Participant J9(F) submitted to a blood test. What is striking is her lack of understanding about what the clinic visit was for, what would happen and why the clinic was providing the specific interventions offered. Indeed, she simply accepted the service without question: J9(F): I didn’t know that they were going to take blood . . . So, I was surprised when they took my blood. INTERVIEWER: . . . you don’t like giving blood or were you surprised that the doctor took blood? J9(F): I was a bit surprised because I thought [clinic name] was simply for a kind of consultation, that we were not going to be examined . . .
A final element of this narrative concerns those who participated in the interventions, yet were not able to retain or act on information – such that they were unable to change their SRH knowledge, attitudes or practice. Passivity towards the programme is a function of its relative lack of importance compared to the need to make money for transfer remittance. Any time that is not taken up by work is spent in ways that women choose – and the programme was not considered important enough compared with the need to sleep, recuperate and socialise: INTERVIEWER: May I know why you didn’t follow the [lesson]? J3(Ai): Because I don’t have time. I am working and I sleep right after coming back from work. I only have one day off a week . . . I’m not really interested and because I don’t have time too.
Similarly, J2(Ai) indicated study as a competing priority and a factor in limited engagement with the programme: I felt so tired . . . I also need to attend [my own] class right afterward . . . Just simply because I don’t have time. If I got time then I will definitely join it [the programme of interventions]. Because I study and work at the same time so I need to split my time.
The consequences, in terms of engagement and retention of knowledge, were stark. One indicative example shows how low engagement was for such participants: R4(Z): I joined 5 [sessions] but I do not remember the titles. Don’t remember the kinds of programme. The first programme, I joined the session, what’s the name, gender, is that correct? INTERVIEWER: Gender, yes. R4(Z): And then, what else. . . (laughs) forgot, Miss.
Interviewees drawing on this narrative did not improve their knowledge, attitudes and practices towards SRH – the interventions were not central to their lives. This narrative provides limited scope for agency in relation to SRH: it falls short of international expectations of empowered women taking charge of their SRH.
Discussion
Governmentality (Foucault, 2007) hypothesises the active self-governance of subjects through three interlocking processes: existing procedures and expectations; power–knowledge nexus; and self-surveillance through technologies of the self. Our findings reveal three narratives of engagement with, and agentic use of, the SRH interventions provided by the programme. These narratives – identified as ‘progressive’, ‘conservative’ and ‘passive’ – reveal strikingly different orientations to programme interventions and the subjectivities constructed by women (Clegg, 2019). Three important aspects which inform women migrant workers’ self-surveillance practices related to SRH are contained within these narratives: salience; the role of affect in gendered subjectivity; and the promotion of a universalist ‘ideal’ moral self within programme design and delivery.
Salience
Our findings demonstrate empirically the importance of perceived salience of SRH as a motivating force in self-surveillance practices. The three narratives reveal differentiated strategies of self-surveillance, informed by the dynamics operating between procedures and expectations, and the knowledge–power nexus. Two of these narratives – progressive and conservative – are clearly related to active self-surveillance with regard to SRH practices. The difference between them is that they are informed by opposing cultural expectations. The third – the passive narrative – reveals evidence of agency, but does not indicate active self-regulation with regard to SRH. Self-surveillance is generated in response to incentives encoded within procedures and expectations and the operation of knowledge–power nexus regimes. Implicitly, where such incentives are perceived as weak or irrelevant to the individual agent, self-surveillance will not be undertaken.
The progressive narrative presupposes high salience, in which women manage their SRH concerns proactively, to avoid unwanted pregnancy and reproductive health disease. This very salience encourages them to undertake the entrepreneurial work on their selves (Cooper, 2015) necessary to comply with the SRH requirements of Malaysia’s strict migration regime – revealed most clearly in use of barrier methods of contraception (both pregnancy and STIs render women liable to deportation). This progressive narrative also enables women to meet many of the universalist standards of the idealised empowered woman in terms of avoiding STIs, rejecting sexual coercion, and making choices about their SRH.
The conservative narrative also reflects high salience of SRH. However, this is refracted through a patriarchal lens (Agu et al., 2016; Metusela et al., 2017; Sciortino, 2020), placing restrictions on who may legitimately access SRH knowledge and practices. The need to secure external approval of one’s moral character provides the motivation for self-surveillance. Our findings show a core of patriarchal values embedded within the narrative – that SRH is only appropriate for married women. Specifically, married women are afforded entitlement to SRH services, including cervical smears and contraception, and are empowered to ask questions within educational settings. However, such agency is discouraged for unmarried women. Due to the patriarchal value-base, unmarried women proved reticent in engaging with programme interventions, and expressed embarrassment about sexual behaviour before marriage. They also comply with the ‘policing’ of boundaries of SRH knowledge by married women. For unmarried women, self-surveillance may thus be enforced socially, through self-consciousness (Bartky, 1991) and fear of being seen to transgress mores, leading to guilt and social shaming (Held, 1991).
The conservative narrative enables women to meet the expectations and procedures of the migration regime through two routes. The first of which, abstinence, is open to all. The second route, involving SRH knowledge and practices (e.g. use of contraceptives), is open only to married women – unmarried women are subject to a power–knowledge nexus on the part of those married women who seek to place restrictions on them. In turn, married women’s own empowerment is circumscribed to the extent that they are bound by patriarchal values inimical to international standards (e.g. sharing the body only with the husband, excluding medical professionals).
The passive narrative is consistent with a subjectivity which does not recognise the salience of SRH. Agency in relation to the SRH programme here is framed broadly in terms of compliance with the requirements of supervisors, labour agents and programme service providers. It reveals an active decision not to engage with the programme in the face of issues accorded greater salience – such as income maximisation, sending remittances home, and even pleasing supervisors. The proximal issues associated with work and its location in the factory and the pressing concerns associated with production targets and continued fitness for work are accorded primacy – the need to attend to their SRH was simply not a priority. Within this narrative, women felt no need to become entrepreneurs of their selves (Cooper, 2015) in order to accommodate the demands of procedures and expectations and the power–knowledge nexus with regard to SRH. In such circumstances, self-surveillance is considered unnecessary.
The relationship of this passive narrative to Malaysia’s strict SRH requirements for migrant workers is ambiguous, in the sense that it does not provide a clear pathway for compliance through either proactive SRH management or abstinence. Women drawing on this narrative were unable to extract meaning for themselves and did not connect programme content to their lives. They also failed to meet the universalist prescriptions of an ‘empowered woman’ – such as making choices in relation to their fertility, applying SRH knowledge to their lives, and viewing SRH as a right for all women.
Gendered subjectivity
Foucault never specifically applied his theory of power to women. Feminist analysis of women’s agency, however, requires sensitivity to women’s subjective experiences of power, to unmask power relations as experienced specifically by women (Deveaux, 1994). Feminists argue that women may have a propensity to internalise the belief that they are subordinate to men, entrenching gender inequity by harnessing women’s own agency to reproduce inequality through time (Rowlands, 1995, 1997). We see this in the ‘passive’ narrative, where women migrant workers accept, without question, direction from their male supervisors and labour agents. If their supervisors did not permit them to engage with SRH interventions, due to the requirements of shift work, women complied with the direction not to attend [R4(Z)]. Similarly, women who were directed to engage with the interventions complied with the direction, even though they did not understand the nature of the programme [J4(Ai)]. Thus, while technical interventions may improve the availability of SRH care, the gendered and patriarchal norms embedded within these women’s lives may continue to limit their autonomy, decision-making power and control over resources (Lim et al., 2020). In order for SRH interventions to be truly transformational, provision needs to be contextualised, challenging such unequal power structures (Chan, 2022; Sciortino, 2020).
Foucault’s failure to address directly the role of affect in subjectivity (Bartky, 1988; Held, 1991) is a serious omission. Within the conservative narrative, affect informed agency such that women’s self-consciousness and sense of shame may prevent them from engaging with SRH interventions. Indeed, our findings indicate the active and agentic role of other women in ‘policing’ engagement with SRH interventions. Unmarried women were reluctant to share concerns about their sexual health, and reticent in asking questions in class. They distanced themselves from the interventions, avoiding the stigma and shame associated with transgression of SRH behaviours expected of them. Self-surveillance and normalisation processes were thus differentiated on the basis of marital status, rather than experienced as totalising (Deveaux, 1994). Our findings demonstrate the importance of considering the role of affect in SRH agency – Foucault’s failure to do so offers an inadequate model of female agency (McNay, 1991; Rowlands, 1995, 1997).
Universalism
Considerable efforts have been expended internationally to secure empowerment for women migrant workers across South East Asia, so that they may confidently and proactively manage their SRH. Many such efforts focus on raising awareness of SRH, and providing women migrant workers access to healthcare services (Brody et al., 2016; Chhoun et al., 2019; Thein and Thepthien, 2020). Overwhelmingly, interventions reflect universalist aspirations and promote a standardised model (Ginsberg and Rapp, 1995).
While our programme was informed by universalist standards, it was implemented by local NGOs in a culturally sensitive manner. Careful attention was paid to the language used, and discussion was contextualised within local lifestyles and cultures. The images used were of local people and places, consideration was taken of social etiquette, and clinical and medical personnel were women, reflecting cultural preferences (Chan, 2022; Smith-Oka, 2009). Despite these sensitivities, the majority of women within our study remained passive.
A point which invites reflection is the extent to which universalist assumptions are desirable and/or practical in meeting such women’s SRH needs – however culturally sensitively they are implemented. In considering the former, our programme logic was that women would regard SRH as an important aspect of their health, and engage with interventions to improve their knowledge, practice and attitudes. Yet, our interview data revealed that some participants challenged universalist global aspirations. Specifically, this related to the composition of groups: married women expressed a preference for group composition to be organised on the basis of marital status, and unmarried women themselves felt uncomfortable engaging in debate with SRH issues such as contraception in a mixed environment.
In considering the latter, practicability, the institutional constraints facing women migrant workers are significant. Given the dominant interest of the government in recruiting low-paid labour, worker protection is a secondary consideration. Existing policies are designed to defend national security rather than protect migrant workers, resulting in weak rights for them (Sok, 2019), including rights to appropriate SRH care (Lasimbang et al., 2016; Loganathan et al., 2020a). Their stay is designed by the state to be temporary and short term, with most workers returning to their home countries upon completion or termination of employment (Anderson and Franck, 2019). Women migrant workers also live in dormitories or housing provided by the company, often located away from urban centres. They may thus be linguistically and socially detached, preventing them from acquiring knowledge of or access to local resources (Anderson and Franck, 2019: 1214). Given their transience, language barriers and exclusion from rights and resources, the extent to which it is practicable for these women to attain the ‘idealised empowered’ selves anticipated by universalist SRH standards is questionable. The lack of a sympathetic context and the limited resources discourage self-actualising behaviours. More fundamentally still, those whose moral frame of reference rejects universalist assumptions will not engage with programme content.
Conclusion
Our primary theoretical contribution is in identifying the importance of perceived salience as the motivating force within self-surveillance practices. While salience is implicit within Foucault’s formulation of governmentality processes, its role has remained underexplored. We draw this out empirically, identifying the conditions required for active self-surveillance on the part of women migrant workers in Malaysia in receipt of SRH interventions. They face significant challenges in managing SRH in a country unsympathetic to their needs. For women’s advocates in such contexts, an understanding of salience is vital in ensuring women’s engagement with SRH interventions.
Additionally, we empirically assess the importance of affect in gendered subjectivities – specifically, the role of self-consciousness and shame in moderating the SRH self-surveillance practices of these women, and their effects on programme engagement. Our findings concur with feminist frameworks that emphasise the importance of recognising women’s experiences as women. This is underdeveloped within governmentality, but is crucial in understanding the self-surveillance practices of women. These considerations of affect are likely to be highly relevant in other South East Asian countries, given the predominance of patriarchal assumptions about SRH. Some of the barriers to SRH service access experienced by women migrant workers within South East Asia are technical and easily addressed – such as location of services and prohibitive costs. However, those barriers which are derived from patriarchal assumptions – such as deference to male partners’ preference not to use condoms – are more difficult to counter. We encourage careful reflection on the implications for developing SRH interventions within these contexts.
Finally, with regard to universalism, and notwithstanding the emphasis on the importance of cultural sensitivity in SRH interventions within the literature, we found that cultural sensitivity was not sufficient cause to ensure women’s engagement with our programme. For many women, institutional constraints informed their value judgements of the practicality of universalist interventions. Our findings suggest that ultimately, the desirability, or otherwise, of such programmes is a function of the extent to which women migrant workers’ own moral values accord with the value-base inscribed within universalist global aspirations about SRH. This incongruence between competing values poses a serious dilemma for women’s advocates in seeking change to workplace practice designed to secure SRH care.
Footnotes
Acknowledgements
The authors would like to thank the anonymous reviewers for their constructive comments on the earlier draft of this article. A special thanks also to Professor Noraida Endut, Dr Suziana Mat Yasin and Dr Lai Wan Teng for their roles in the funded research project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors acknowledge the British Council for their generous funding of the project ‘Health Interventions to Advance the Sexual and Reproductive Health of Women Migrant Workers in Malaysia’ under the Newton Fund Impact Scheme (Grant Number 536753284) on which we draw.