
Abstract
Malaysia is a major importer of migrant labour within the ASEAN region, and migration has adverse implications for the sexual and reproductive health (SRH) of women migrant workers. Given the centrality of the workplace to the lives of such women, this article reports a qualitative analysis of interview data with women migrant workers (N = 14) and wider stakeholders (N = 10) and considers the extent to which they are able to effect change in workplace SRH policy and practice. Informed by Jo Rowlands’ typology of power and model of empowerment, the analysis considers the extent to which normative expectations of process and collective mobilisation upon which feminist empowerment models are predicated operate in such contexts, and discusses the implications of the findings for research to advance workplace democracy.
Introduction
Sexual and reproductive health (SRH) is a basic human right enshrined within the Programme of Action of the International Conference on Population and Development (1994); UN SDG3 (‘good health and well-being’) and SDG5 (‘gender equality’); and the Convention on the Elimination of all Forms of Discrimination Against Women (1979). While migration affects the ability of women to manage their SRH, research on safeguarding women migrant workers’ SRH remains limited, especially in the developing world. In this journal, migrant workers’ informal employment (e.g. Clark and Colling, 2016), mobilisation and organisation (e.g. Cam, 2014; Refslund, 2018; Tucker, 2020) and motivations for migrating (e.g. Cam, 2017) have received attention. Research on how they manage their health-related needs however remains underexplored – although this is considered as part of wider analyses in the context of workplace occupational health and safety (Hopkins, 2017; Walters and Wadsworth, 2020). We contribute by investigating how factory women migrant workers in Malaysia manage their sexual and reproductive health needs and, given the centrality of the factory to their lives, the extent to which they can effect change in workplace SRH policy and practice. Our study is timely and important given increasing levels of female migration within the Association of Southeast Asian Nations (ASEAN) region, and the significance of Malaysia as employer of migrant labour in the region.
Sexual and reproductive health of women migrant workers
Within the ASEAN region, women account for half of the 6.9 million intra-ASEAN migrants (The ASEAN Secretariat Jakarta, 2017). Barriers to SRH include lack of relevant knowledge (Manoyos et al., 2016), cost (Webber et al., 2015), language difficulties in an unfamiliar environment (Tangmunkongvorakul et al., 2017) and unsympathetic migration regimes (Boonchutima et al., 2017; Lasimbang et al., 2016). Social and cultural taboos concerning SRH further compound the problem (Hegde et al., 2012; Jordal et al., 2014) as does the extent to which they can access healthcare, often dependent on collaborations between the state and other institutions (Truong et al., 2014). Consequently, millions of women migrant workers remain at risk of sexually transmitted diseases, reproductive disorders and unwanted pregnancies.
In clarifying how factory women migrant workers manage their SRH, and the extent to which they can effect change in factory policy and practice, we employ a feminist empowerment lens. Using such a lens to frame our discussion helps us understand the wider causes of gender-based inequities and of the need to transform gender norms and relations harmful to women (Cornwall and Edwards, 2010). Indeed, even if access to SRH care were available to these women, this does not mean that they are able to engage with these services. Feminist scholarship stresses the importance of adopting a gendered understanding of subjectivity attendant to women’s experience of power. In the context of the factories within which these women work, we unravel the multi-layers of power influencing the degree to which they are able to make, and influence, decisions about their health.
We make three contributions to the literature. First, we identify the subtle, and often hidden, factors preventing such women from managing SRH needs in the workplace. Secondly, we make an empirical contribution in documenting the SRH experiences of a highly marginalised and sizeable working population which remains underexplored. Thirdly, in applying Jo Rowlands’ model of empowerment to the workplace, we offer theoretically-informed insights into the challenges of shifting the overall terms of exchange in favour of this segment of workers.
Below, we engage critically with the concept of ‘empowerment’ in the context of women migrant workers’ SRH. We surface limitations of Foucauldian understandings of the relational nature of power: principally an abstract and de-gendered formulation of the nature of the subject which erases women’s experience of power, and an agonist reading of the nature of power which fails to address empowerment processes. We then critically assess an alternative typology of power which directly attends to these shortcomings and offers a conceptual framework better suited to the context of women migrant workers’ SRH rights (Rowlands, 1995, 1997, 1998). Having done so, we introduce the Malaysian context and its implications for our empirical study, which considers the extent to which these women are able to manage SRH needs and effect change in the workplace to accommodate these needs.
Empowerment
Power has historically been considered in terms of coercion, whereby one person or group controls the actions of another (Bachrach and Baratz 1970: 105; Lukes, 1974; Weber, 1947). Foucault offers an alternative in which power is reconceptualised as an effect – a relational property embedded in a network of social relationships (Foucault, 1982) such that it circulates and exists only in its exercise (Foucault, 1980). Resistance – consisting of challenges between individuals over identities and relations – is an inevitable corollary to power.
The Foucauldian understanding of power as an effect rooted in social networks has been criticised by feminists for an inadequate conceptualisation of the ‘subject’ which erases women’s experiences of power (Bartky, 1988); and for offering no account of the processes required for women’s empowerment (Deveaux, 1994). Foucault fails to account for the gendered nature of disciplinary norms and practices – the extent to which self-surveillance and normalisation processes are experienced as differentiated rather than totalising, and the degree to which women are docile or active in relation to discipline, whether through individual or collective struggle (Deveaux, 1994). Neither is there consideration of the ways in which women may mediate contradictory demands made of them as gendered subjects (Bordo, 1989), such as the requirement to comply with labour market demands while simultaneously being denied basic reproductive rights. Similarly, the assertion that power is manifest when exercised (Foucault, 1980) is not used as a starting point for considering women’s agency – masking power relations as experienced specifically by women (Deveaux, 1994). Women may, for example, experience the disempowering effects of self-consciousness, shame and unreciprocated emotional care (Bartky, 1990). Foucault’s emphasis on external obstacles to the exercise of political power to the exclusion of interior obstacles within the realm of emotion and affect (Held, 1993) fails to recognise gendered expectations, address women’s internal affect-based barriers to agency and choice or acknowledge that women’s lack of freedom may result from men’s freedom in a zero-sum game (Deveaux, 1994).
In contrast, a specifically feminist analysis of empowerment embraces women’s subjective experiences of power informed by dynamics of self-actualisation to expound possibilities for resistance and change. These concerns have specific resonances in the context of developing countries, informing directly theories of women’s empowerment. Rowlands (1995, 1997, 1998) exemplifies these considerations, as elaborated below.
Feminist empowerment: Rowlands’ typology of power
Rowlands rejects Foucault’s abstracted (gender-neutral) conceptualisation of the subject and agonist framing of power, offering instead a gendered analysis of processes informing agency and choice, and a model of empowerment which considers personal, relational and collective dimensions. Of course, a general limitation is the difficulty of deploying concepts and theories developed mainly in the West (UK and US) in the very different context of ASEAN and especially Malaysia, which has the most ethnically diverse population and institutionalised discrimination. We note that while Rowlands’ theory of power and model of empowerment were developed in the West, they have been successfully applied widely in the global south, both by development NGOs and researchers (Cornwall, 2016; Monkman, 2011; Rowlands, 1997).
Rowlands (1997) emphasises the impact of internalised oppression on the exercise of power, and the generative role of oppression in continued inequities between men and women over time. Internalised oppression reduces the need for coercion by the extent to which women voluntarily enact a subordinate status (p. 13). She distinguishes the various forms which power can take. ‘Power-over’ is a controlling power and may be met with compliance, resistance or manipulation, whilst ‘power-within’ is based on self-acceptance and self-belief, enabling people to believe that they can make changes in their lives and imagine new ways of being. ‘Power-with’ is forged through organisation, solidarity and joint action, in which people act together to improve conditions for themselves. Finally, ‘power-to’ means the capability to decide actions and carry them out (Rowlands, 1997: 13).
As power takes multiple forms, empowerment may mean many things. It could refer to achieving ‘power -over’ or, alternatively, development of generative power such as ‘power -to’ and ‘power-with’, in which people realise their common interests and mobilise around them. It could also incorporate ‘power-within’, which includes processes that lead people to perceive themselves as able and entitled to make decisions (Rowlands, 1997).
Empowerment is conceptualised as a process (Rowlands, 1995) in which women first become aware of their own interests and then move from insight into action. Rowlands suggests that empowerment operates in three dimensions: personal, in developing a sense of self-confidence and capacity and undoing the effects of internalised oppression; relational, in the ability to negotiate and influence the nature of relationships; and collective, where women work together to achieve an impact greater than that which any individual could have done on their own. On each dimension, inhibiting and encouraging factors influence a set of core values and lead to change (Rowlands, 1997, 1998: 24).
On amassing collective power, researchers, including those from the employment relations tradition, have drawn upon elements of social movement theory (Klandermans, 1997; McAdam, 1988; Tilly, 1978) to identify under what conditions marginalised populations can be mobilised into collective action against issues which they perceive as unjust and how they determine what actions can be taken to change them. Però (2014), Jiang and Korczynski (2016) and Alberti and Però (2018) detailed how migrant groups in the UK organised mass mobilisation by addressing barriers to mobilisation and building collective identities among these highly fragmented workers. In some cases, collective consciousness and collective action were facilitated through building ‘communities of coping’ (Jiang and Korczynski, 2016; Korczynski, 2003; Yilmaz and Ledwith, 2017). These are defined as ‘oral-based informal networks in or beyond the workplace’ where people turn to each other for emotional support (Jiang and Korczynski, 2016: 814; Korczynski, 2003). The NGO in Jiang and Korczynski (2016) created safe spaces (notably in its monthly meetings) for domestic migrant workers in the UK to form communities of coping, which spilled over into houses, restaurants, churches and parks after work where migrants formed their own social circles (pp. 825–826). The women’s liberation movement developed out of the 1960s civil rights movement in the US (Evans, 1980), taking an identity-focused direction in which women developed a fresh conceptualisation of themselves and the inequalities they were subject to. They brought new understandings, radical politics and personal networks together to create the movement. Development of ‘insurgent collective identity’ requires a combination of social spaces where women can develop a new sense of worth; role models that encourage action; an ideological framing of sources of oppression which justifies revolt and imagines an alternate future; a threat to the newfound sense of self which forces women to confront inherited cultural definitions; and a network through which a new interpretation can spread, activating a social movement (Evans, 1980). Yet, we note that organising collective action is complex, especially in large groups; each member has their own interests which differ from those of others. Individuals in such groups are thus likely to free-ride on the efforts of others, especially if the group seeks to generate a public good for everyone within it. Indeed, in the absence of incentives and personal gain to motivate individual participation, collective action is unlikely to occur despite the sharing of common interests (Olson, 1965).
The Malaysian context
Successive National Development Plans have emphasised a need to move to higher value-added, knowledge-intensive activities. However, Malaysia’s electronics sector remains a major contributor to its economic growth. Export processing zones in Penang offer incentives such as exemptions from taxes, low rental rates and reduced regulatory oversight to foreign investors such as Canon, Bosch, Microsoft, Intel, HP, Dell and Foxconn. Working conditions in these factories are highly regulated as they strive to meet tight production deadlines.
A significant portion of workers in these zones are migrant women. Although official figures suggest that there are half a million women migrant workers in the country (Ministry of Home Affairs, 2019), other reports suggest that the total number of foreign workers could be as high as 5.5 million, rather than 2 million (Yi et al., 2020). Numbers of women migrant workers in Malaysia are thus likely to be much higher than official estimates.
A migration regime intolerant of SRH needs and a patriarchal civil society combine to make these women vulnerable to challenges related to both labour and gender. As migrants, they are excluded from many legal protections enjoyed by citizens. This differential treatment means that the most privileged are given access to world-class healthcare facilities, whilst the poorest and most vulnerable experience the worst health outcomes (Ormond and Nah, 2019). As women, they are at greater risk of exploitation than male colleagues, given patriarchal practices replicated in the workplace and relationships of subordination with male supervisors and male union leaders (Evans, 2017). Women migrant workers have been instrumental in supporting Malaysia’s economic growth and local women’s labour force participation rate, yet live in precarious and exploitative conditions, subject to stringent state and employer control (Anderson and Franck, 2019; Elias, 2014; Hierofani, 2020).
The confluence of patriarchy and a migration regime inimical to SRH needs results in widespread denial of women migrant workers’ SRH rights. The requirement to take an annual pregnancy test under threat of deportation if found pregnant contravenes the Convention on the Elimination of All Forms of Discrimination Against Women formally ratified by Malaysia in 1995. Forced deportation is defended on the grounds that, as Malaysia’s foreign workers are employed on fixed-term contracts, foreign workers having children poses social problems and legal complications. Women migrant workers testing positive for STIs are also deported, on the basis that they are no longer fit to work. De Genova (2019) notes that their susceptibility to deportation is a virtually universal feature of migrants’ non-citizen status, and that ‘this possibility of being deported, of being forcibly expelled from the space where migrants are actively engaged in making their lives and livelihoods – has profoundly disciplinary repercussions’ (pp. 93–94; see also De Genova, 2010, 2014). Women cannot bring their families, marry a Malaysian or a citizen of another country. This prohibition on marriage is imposed on migrant workers who hold the Visit Pass (Temporary Employment) (Immigration Department of Malaysia, 2021). However, Islamic law permits citizens to marry migrant workers (Malay Mail, 2017), although these workers then forfeit the right to work under the Visit Pass (Temporary Employment). They are also prohibited from changing employers or employment sector (Fair Labour Association, 2018: 22).
Abortion has been legal since 1989 (Section 312 Malaysian Penal Code), but the law is applied to discriminate against women migrant workers. The case of Nirmala Thapa, a Nepalese woman migrant worker and the first woman to be charged for undergoing abortion in a registered clinic in Malaysia, reveals the catastrophic consequences of abortion for women migrant workers, including loss of employment and threat of imprisonment (Archer, 2018). Migrant-related policies and laws in Sabah, Malaysia focus on controlling the adverse social effects of migration and do not protect SRH rights (Lasimbang et al., 2016). Migrants pay twice the fee for health treatments compared to citizens and face discrimination by healthcare providers.
Finally, stigma and taboo associated with SRH mean that it is typically excluded from advocacy work. Unions do not address the SRH needs of women workers because they are perceived as falling within the private domain, even if SRH conditions prevent them from being able to work. Many women’s organisations, while sympathetic to their health needs, exclude women migrant workers from programmes due to lack of resources (Miles et al., 2019).
We explore empirically below conditions for the personal, relational and collective empowerment of women migrant workers within Malaysia in the context of their SRH. We draw on Rowlands’ typology of power as a conceptual lens to offer an original qualitative analysis of experiences reported by women migrant workers, together with the views of a range of respondents drawn from service providers, NGOs, government agencies and private firms. This abductive analytic framing enabled us to elaborate respondents’ subjective experiences of power within the factory setting, tracing the power effects which ultimately impede actions to influence workplace health practices.
Methods
The research team collected data reported here as part a wider project on capacity building and empowerment related to the sexual and reproductive health rights of women migrant workers in Malaysia, funded by the United Nations (UN). We adopted a qualitative case study design (Stake, 1995) informed by rapid appraisal principles (Kumar, 1993). We collected semi-structured interview data to explore women migrant workers’ beliefs, feelings, values and motivations (N = 14). Given the relational nature of power implied by our theoretical framework, we also sought views from representatives of unions, healthcare providers, NGOs, employers and governmental agencies (N = 10). We collected data between August 2017 and February 2018.
We adopted a purposive approach to sampling for both migrants and stakeholders. The Malaysian authors identified initial relevant stakeholders from their knowledge of local advocacy agencies. Additional stakeholders were recruited through application of snowball sampling techniques to capture representatives of healthcare providers, unions, NGOs and employers. While snowball sampling may be considered a weakness due to its opportunistic nature (Emmel, 2013), we were purposive to the extent that we ensured coverage of the range of relevant stakeholders. A total of 10 stakeholders were recruited in this way. All of the women migrant worker respondents (N = 14) worked in factories in the consumer electronics and electronics components sector in Penang, Malaysia, in product assembly operations for global firms. Recruitment of women migrant worker participants was not straightforward. As they work long hours and live in migrant worker hostels we adopted a pragmatic approach to participant recruitment through local gatekeepers (healthcare providers and unions) drawn from our sample of stakeholders. Due to topic sensitivity, the possibility of negative repercussions and the potential vulnerability of these participants, we were careful to ensure that informed consent was elicited, and data collection undertaken, by female Malaysian members of the research team. Of the 14 interviewees who were women migrant workers, eight were recruited via a union as gatekeeper, and another six via a healthcare provider. Interviews typically lasted for an hour.
Respondents were of Indonesian or Nepalese origin. All of them had up to secondary school education. In order to establish trust, the research team approached gatekeepers such as unions and healthcare providers, who were already known to women migrant workers. Members of the research team are ethnically diverse, and spoke the language of the Indonesian women. Interviews with the women from Nepal were conducted in English, which was their stated preference. Before commencing interviews, women migrant workers were fully briefed on the purpose of the research and were invited to clarify any questions. If they did not wish to respond to questions, they were assured that this would not be frowned upon. We asked women migrant workers what they understood SRH to mean, barriers to meeting SRH needs and how their agency to do so could be improved. Through provision of a safe, non-judgemental and respectful forum (Oakley, 1981) we created a level playing field between researchers and women and elicited in-depth information which they might have concealed if they felt that they were being criticised. Interviews were recorded, transcribed and analysed thematically (Braun and Clarke, 2006).
Data analysis
Given our research questions, we undertook an abductive thematic analysis of the qualitative interview data (Tavory and Timmermans, 2014). This approach entailed using Rowlands’ typology of power as a starting point in categorising respondents’ answers to interview questions – collating the data associated with each form of power in the typology and exploring the range of experiences related to each. This approach allowed us to elaborate the typology and explore its contours within the present context. In this way, respondents’ narratives enabled us to explore the different kinds of power which shaped agency to manage SRH. Consistent with our analytic approach, we organise and present our findings through the lens of Rowlands’ typology of power, considering power-over, power-within, power-with and power-to in sequence.
Findings
While access to economic opportunities lifted women and their families out of poverty, employment through migration exposed them to many health and healthcare vulnerabilities.
Life as a migrant worker (power-over)
Within the factory, women experienced a highly structured regime. A range of barriers within the factory prevent them from being able to manage their SRH. Work hours, meal times, rest and toilet breaks were closely regulated, on the assumption that temporal regularity would better enable workers to meet production targets. No formal concessions were made in terms of rest or reduced workloads for those struggling with menstruation-related pain and any support offered was informal.
I always experience intense period pain. So, I go to toilet to apply some balm . . . my co-worker beside me took over my job. My supervisor didn’t care for me. I wish someone would just give me a chair to sit and work. But I never got a chair. I have to stand for 12 hours and withstand the pain. (WMW#1)
Women were wary of their supervisors, often male, and who became angry if women did not meet their production targets. Consequently, women dared not approach supervisors with SRH-related concerns, for fear of being reprimanded. In fact, the power imbalance between these women and their male supervisors often led to sexual harassment and violence. Yet women migrant workers were afraid to ‘make a police report because that has repercussion for their jobs’ (NGO#1).
Women were not permitted to leave the factory to seek SRH care during working hours, but SRH care was not provided within factory clinics. Standard practice within factory clinics was to offer painkillers for all presenting conditions, including SRH.
They didn’t even check us. They ask us to sit, then start to be busy with the medical report, and then give us the pink Panadol. Ask us to take a cup and get some drink then back to work. (WMW#1)
Respondents made frequent reference to prohibitions against pregnancies. While some supervisors were sympathetic to health conditions, no such discretion was available should a migrant worker’s pregnancy became known to employers. This constituted a breach of the employment contract, automatically resulting in deportation to their country of origin: . . . women migrant workers cannot get pregnant here. Everything is by law, if we get pregnant, we will be sent back to our home country. (WMW#2)
Where women visited private clinics outside of the factory premises, they reported experiences of discrimination from local healthcare providers on the basis of their migrant status: Many clinics out there do not appreciate foreigners at all . . . the nurse gave us very quick and perfunctory instructions on how to consume the medicine ‘eat this a little, eat that a little’. Sometimes when we are sick, our hearing is not good, and we feel dizzy. So, we asked again what did she say? She shouted at us ‘can’t you just read this and that?’ (WMW#2)
Finally, women’s SRH was considered unimportant by employers, to the extent that many employers challenged claims for SRH service provision for women migrant workers. The view was expressed that these women were, in fact, privileged, as they were legally allowed to work longer hours than citizens, thereby increasing their earning capacity (Employer#1). Women migrant workers’ SRH status is monitored rigorously, with annual pregnancy tests imposed, and pregnancies result in termination of employment and deportation. Yet no support was offered to women to manage their SRH within factories; one government agency we contacted claimed that it was a private issue and women were themselves to blame for not taking care of their own SRH (Gov#1).
Women also reported that their respective embassies and consulates rejected pleas for help from pregnant women migrant workers, which was again considered a private issue: If you have trouble with work or wages, yes, you can complain to the consulate. Breast cancer, yes. But if it is about pregnancy, we cannot tell them. (WMW#3)
‘I am weak and don’t deserve anything’ (power-within)
Women’s sense of entitlement to SRH was low. Many women did not understand what SRH was and stoically put up with pain and discomfort (WMW#4). Many women migrant workers internalised low expectations and did not express the opinion that they were entitled to challenge the social order. Many blamed themselves, saying that it was their fault that they fell pregnant and that they deserved to be deported: Law is law. We were well informed during our time in Indonesia. If it’s stated in contract and you still got pregnant, factory will send you back. (WMW#4) We are the ones who always do bad things. We should follow factory’s rules and laws, right? Before we came to work, the factory already asked us . . . work in this factory, you can’t do this and that. We agreed and signed. But we break the rules, right? So, it is our fault. (WMW#3)
Women relayed to us that those who fell pregnant often left employment of their own accord, becoming undocumented migrants.
. . .and she confessed about her pregnancy. She tried to do abortion by herself, such as drink medicine. But she did not succeed, perhaps the baby is already stable. After that, she tried soda, pineapple juice and all sort but nothing worked. At last, she ran away from the factory. (WMW#4)
WMW#2 explained: If pregnant, will be sent back. So most of our friends, if they get pregnant, they won’t tell, they will keep quiet. Some just go back. Some stay here without permit, some went back to Indonesia. They ran away, and I don’t know where they are now.
These responses show a reactive approach toward addressing SRH needs. NGOs confirm this orientation. Indeed, one NGO expressed frustration that some unmarried women migrant workers viewed termination as the ‘end of the problem’ and did not change behaviour: After abortion, we talk to them about contraception, they actually are totally in denial. They say, ‘It’s only once, I never do it again. I will never do it again’ and of course, they come back again with the same problem. So, it’s often a second visit before we manage to tell them, ‘look you know, why don’t you just use precaution?’ (NGO#2)
NGO respondents providing healthcare services attributed the lack of ability to manage SRH to limited education and poor access to information. While SRH education and training were valued by women as essential in supporting their SRH, they were seldom able to take advantage of SRH lectures and workshops organised by NGOs (where allowed to do so) because tight production schedules did not allow them to make use of these services: . . . on a few occasions . . . we go to the factories . . . the auditorium is for about 60 people . . . you get only 15 or 20 because of the shifts . . . if their production schedule is so tight, the factory is just not prepared to allow the women to attend to their health. (NGO#2)
Women struggled with language barriers when attempting to access SRH services: So, our problem with getting the hotline number out is that we are communicating mainly in English . . . our website is in English . . . if you type Malay ‘penguguran’ (abortion) on Google, our hotline number doesn’t show. It is because you cannot search in Malay for a thing like this. So, the people that search and find our hotline number are English educated or . . . they speak English. We are not catching a big spectrum of our clients. (NGO#1)
Sense of the whole being greater than the sum of individual parts (power-with)
The factory setting afforded possibilities for developing expanded friendship networks which can offer support in times of need and sources of SRH information. Some women recounted use of social media platforms to forge friendships, which enabled them to share SRH needs, take on colleagues’ work (WMW#2) to alleviate discomfort caused by SRH conditions, while others (WMW#6) took leave to accompany friends to SRH clinics outside the factory.
Yet such friendships remained fragile given the enormity of the negative consequences of placing trust in the wrong person. Women were selective of who they turned to, especially so in cases of unwanted pregnancies and abortions, for fear that co-workers might report them, which would result in instant termination of contract and deportation: . . . later if we have an argument, she might tell my secret out loud. (WMW#7)
Mobilising these women collectively to assert SRH needs was problematic. Both NGOs and unions provide some support here, although their emphases differ. NGOs cater for the SRH needs of both local and migrant populations in Malaysia. They provide services such as SRH related in-house training, lectures, STD screening tests, counselling, shelters for women in crisis, etc. However, they are often under-resourced, limiting their capability to address these needs. Unions are focused on occupational health but do not specifically address SRH issues as these are regarded as private and falling outside of their domain.
One union official informed us that while the union did organise health seminars, these were narrowly focused on diet, nutrition and safety at work (Union#1). Many programmes were also directed at local women. Another union respondent informed us that unions did not get involved in SRH issues as these were not considered to be work-related (Union#2), fragmenting opportunities to build solidarity around SRH.
NGOs were invisible to women migrant workers. Many women had not heard of local NGOs and even if they had, never thought to approach them: [Are there] any NGOs? I don’t know. We have no connection with them . . . We can solve the problem by ourselves. (WMW#7) They didn’t look for me. I also don’t understand how to find them. What is their job? (WMW#3)
Conversely, NGOs themselves noted difficulties is accessing women migrant workers, unless factories saw a value in educating their workforce about health: . . . what I did is write to a lot of factories to offer talks to women migrant workers . . . to inform employers that reducing cost of healthcare treatment would reduce the burden on the factory also. Because they are not interested in [any] other thing besides money. (NGO#3)
While some women migrant workers expressed the desire for leaders emerging from among their own to mobilise around SRH provision, this was not achieved. Women lacked the SRH knowledge to be able to lead, and for many, the priority was to earn an income. Health issues were peripheral: . . . when you come here as a woman migrant worker, you are already disadvantaged . . . you don’t have money, you don’t have a place to stay, so all those things are more important to you than contraception. (NGO#2)
New possibilities and actions to manage SRH? (power-to)
As opportunities for collective organisation were limited, women drew on individualised means to secure their SRH. Our respondents discussed agency related to SRH in terms best described as ‘surreptitious’; drawing on fragile informal networks and ‘clandestine’ knowledge gleaned for the purpose of evading coercive power. Thus, it was common for women migrant workers to attend to SRH reactively – by ‘dealing’ with pregnancies as they occurred, hiding them from others as far as possible and making their own provision for termination. This also necessitated timing terminations to avoid routine factory screening, avoiding detection and consequent deportation: . . . in [month], I must go through medical check-up to enable me to continue working another two years. If I do not do the abortion earlier, and my factory finds out about my pregnancy, I will be sent back. (WMW#3)
Where abortions were performed too near to a mandatory screening date, it was common for women to substitute their boyfriends’ urine sample for their own, to avoid detection of having been pregnant: You have this abortion and when you go for your medical check-up, get your boyfriend’s urine . . . it works every time. So, that’s it. After all, she is not pregnant anymore, so why should she be discovered? (NGO#2)
Many women attended to SRH through use of traditional medicines. For example, ‘jamu’ from Indonesia (made from natural materials such as roots, bark, flowers, seeds, leaves and fruits) was known for boosting women’s internal health, maintaining energy and even for ‘overcoming period pain’ (WMR#3).
Jamu was easily accessible as women migrant workers prepared the medicines themselves, and women regularly took it to revitalise their bodies: One bottle RM4. Finish it in one shot. Back in Indonesia, our mother will make that for us also. Here we don’t have time but some of them are hardworking and they can make this Jamu. So, we buy from them. (WMW#5)
Discussion
Power lies at the heart of Rowlands’ work, manifest in its exercise, and taking one of four forms. We applied Rowlands’ typology of power to women migrant workers’ narratives of SRH management, revealing how the various forms of power intertwined to prevent them from exercising responsibility for their SRH, let alone influence factory practices to accommodate these needs. The women lived restricted and highly regulated lives. They accepted patriarchal power structures within the factory. They did not influence new areas of activity; they neither organised collectively to claim SRH rights nor influenced the behaviour of their supervisors toward their SRH needs. While they were able to identify a series of interventions that may enable them to improve their SRH, they did not articulate an alternative, let alone mobilise around it. Nor were they able to forge collective identities (Alberti and Però, 2018; Però, 2014) or build robust ‘communities of coping’ (Jiang, 2018; Korczynski, 2003). Their networks were fragile which prevented them from coalescing around a common cause (Evans, 1980). Their ideological framing of their situation was one of ‘deservedness’ and ‘helplessness’ and no women migrant worker we interviewed could imagine an alternative way of being.
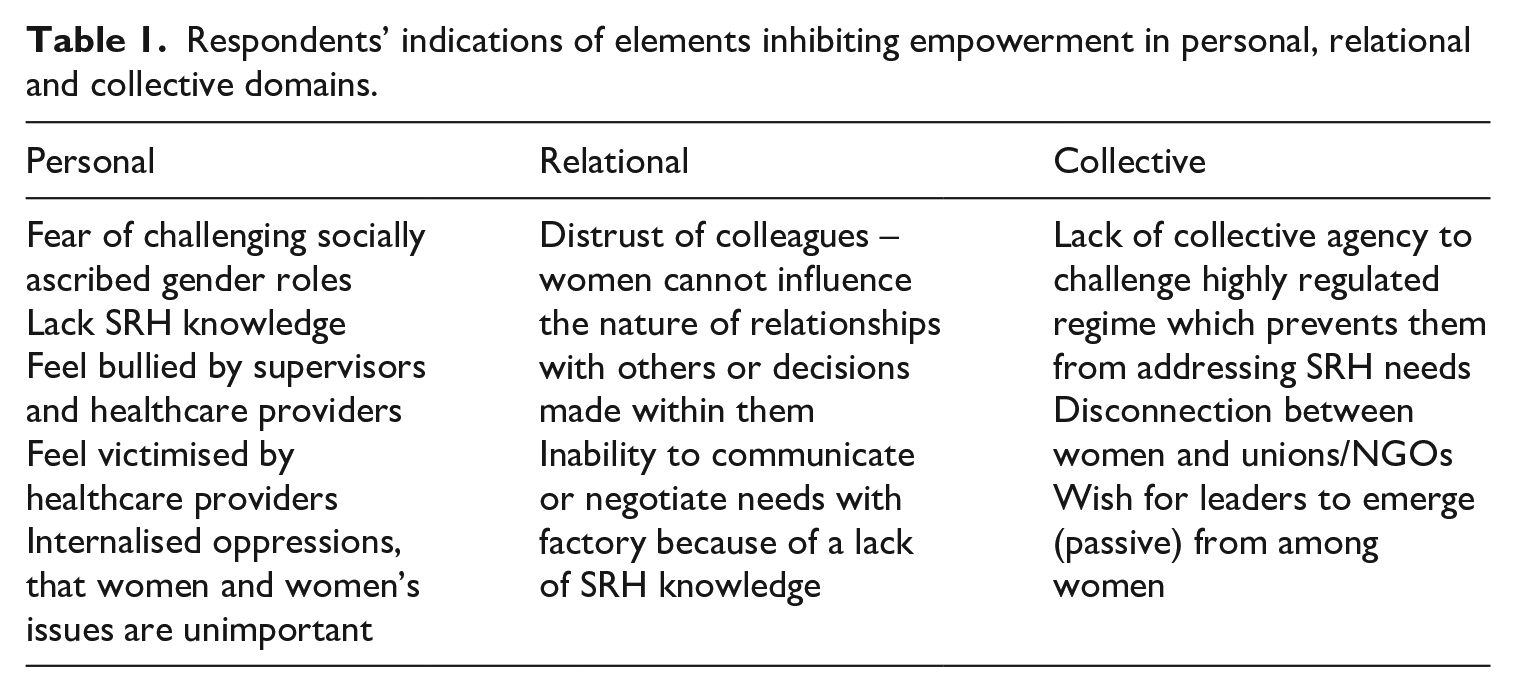
Rowlands argued that within the three dimensions of empowerment, factors may either inhibit or encourage change. Organising things in such a way as to support empowerment processes can be done either by increasing the strength and likelihood of the encouraging factors, or by reducing, avoiding or counteracting those which inhibit change (Rowlands, 1998: 24). We summarise the experience of respondents across empowerment dimensions (Table 1).
Respondents’ indications of elements inhibiting empowerment in personal, relational and collective domains.
The importance of context is emphasised, and Rowlands urges us to identify specific factors within each category of empowerment, as appropriate to local circumstances (Rowlands, 1998: 25). We present below two themes relevant for these women’s advocates (e.g. trade unions, NGOs) in doing so. We also consider the extent to which a new ‘road map’ for empowerment, prerequisite for women managing and influencing SRH in the workplace, is required.
Processual nature of empowerment
Rowlands envisaged empowerment as a process. Specifically, in relation to personal empowerment, she asserted that ‘the work needed for raising levels of confidence and self-esteem among poor and marginalised people in such a way that will enhance their ability to take charge of their own needs is necessarily time-consuming. It is a process that each individual has to do at her or his own pace’ (Rowlands, 1995: 105). Rowlands also envisaged that empowerment in one dimension can influence the development of the same in others. Arguably, the attainment of SRH knowledge and confidence at a personal level has a spill-over effect to positively influence others, and over time, can galvanise collective action to claim SRH in the workplace.
In building personal empowerment, advocates can cultivate SRH knowledge, self-esteem and confidence among these women. They can consider what resources are present which can support this task. But it takes time to nurture these positive qualities. Empowerment is time-consuming and self-confidence cannot be built quickly (Rowlands, 1995). This is problematic for women migrant workers as contracts are typically awarded annually without guarantee of renewal. Pregnancies, illnesses and disabilities result in deportation on the grounds that these women have become unfit to work. Workforce turnover in factories is high and is a signature feature of employment-related migration. Women migrant workers are generally granted short-term (two or three year) contracts, although under the law they are allowed to remain in Malaysia up to a maximum of 10 years (Immigration Department of Malaysia, 2021). While in employment, they undergo regular health checks, performed by a government appointed body (FOMEMA, 2020). Those who fail the medical check-up are deported. Women can also opt to discontinue their employment contracts once their original term expires. As women migrant workers disperse into their respective communities upon return to their home countries, any personal empowerment gained is subsumed. The likelihood of achieving relational and collective empowerment is severely attenuated in these circumstances, and will take time, as these forms of empowerment are dependent on the involvement of many actors and require deep structural transformation (Huis et al., 2017; Rowlands, 1995).
Collective empowerment
Rowlands asserts the importance of collective action in securing change for women: ‘while individual empowerment is one ingredient in achieving empowerment at the collective and institutional levels, concentration on individuals alone is not good enough. Changes are needed in the collective abilities of individuals to take charge of identifying and meeting their own needs’ (Rowlands, 1995: 105–106). Through collective empowerment, marginalised populations can access political structures and formal decision-making processes. The social movement literature suggests how subordinated groups can come together, experience cognitive liberation (McAdam, 1988) from a starting-position of low self-esteem and feelings of powerlessness, develop a collective sense of injustice and act collectively to seek redress (Evans, 1980; Tilly, 1978).
Despite originating from different countries, study respondents shared similar socio-economic backgrounds, cultures, ages and levels of education. Many held religious faiths in common, worked in the same factories and shared accommodation and they had similar SRH needs and concerns. These factories exhibit many of the attributes of ‘communities of coping’, intimate, dense, oral-based networks in which women can turn to each other to seek support from each other in the face of collective work problems and can even play a part in the wider social relations in the workplace (Korczynski, 2003). Such communities may forge collective identities, even among highly fragmented peoples, existing as transformative (liminal) sites – forging collective agency by providing safe spaces for socialising, mutual trust and exchange of work grievances (Jiang, 2018; Yilmaz and Ledwith, 2017).
Yet, despite working in circumstances propitious to forging collective consciousness around SRH, respondents largely distrusted each other, particularly so in the context of unwanted pregnancies and abortions. This mistrust and the subordinate power relationships with their factories mitigate against social solidarities (Evans, 1980). The potentially catastrophic implications of being found to be pregnant or having undergone an abortion or an SRH disorder acted as a strong disincentive to collective action. Their predicament is resonant of Olson’s (1965) contention that large groups will not work toward common objectives unless individual members are motivated to do so. While the women in our case study shared a common interest, they were, due to lack of knowledge, a sense of solidarity and resources, reticent to organise collective action. They were further disincentivised due to their short stay in the country – there was no personal incentive or gain for them to do so. In theory, women likely free-ride on the efforts of others, given that collective action seeks to generate a public good. Paradoxically, however, the likelihood of any public good being generated by collective action is so limited that it is difficult to anticipate that women conceived that they could derive any benefit.
Legal limitations on the open mobilisation of women migrant workers in Malaysia should also be acknowledged. While union membership may offer collective support, membership rates are low. The right to organise is controversial in Malaysia, which has ratified ILO Convention 98 (Right to Organise and Bargain Collectively), but not Convention 87 (Freedom of Association and Protection of the Right to Organise) (Chu, 2019). Migrant workers are allowed to join unions but prohibited from holding the role of union office bearers or forming their own unions (Section 28, Trade Union Act 1959). Migrant workers currently form less than 3% of union membership. Wider prohibitions against joining any association are imposed in work permits (ITUC, n.d.). Additionally, migrant workers work under fear of dismissal if they joined unions. There have been cases of migrant workers being cautioned, prior to accepting employment, that they would be deported if they joined a union (Chung, 2019). Wherever migrants gather in public places, they can be dispersed under the Peaceful Assemblies Act 2012.
Women migrant workers risk being arrested and deported for participating in public assemblies. Given severe repercussions for migrant workers becoming visible, advocates need to envisage alternative ways of mobilising the collective empowerment of these women. While it may be possible to harness seemingly disconnected and fragmented migrant workers to develop into resistive solidarity in the UK (Alberti and Però, 2018; Jiang and Korczynski, 2016), this requires rights of free assembly not currently available within Malaysia.
While unions have a critical role in advocating protection of SRH of women migrant workers, currently this aspect of health falls outside of their approach (Miles et al., 2019).
A new road map for empowerment of this sui generis group?
The Malaysian case shows the oppressive environment in which women migrant workers live and work, with seemingly limited possibilities for successful progress toward empowerment for SRH. This experience is unlikely to be unique to Malaysia as similar production regimes are replicated globally within export processing zones. Strict regulation of SRH within factories is not unusual; Thailand, Taiwan, Singapore and most Gulf Countries mandate their women migrant workers to meet specific SRH status (e.g. pregnancy and STI tests) on either a yearly basis or upon contract renewal (Fair Labour Association, 2018).
From a feminist perspective, the role of collective action in achieving social transformation is celebrated as fundamental (Kabeer, 2005; Rowlands, 1995; Stromquist, 1995, 2002). Yet, this logic assumes that the subject actors (women migrant workers) have a place and role in the society in which they are acting, and wider societal acceptance of the legitimacy of these actors’ empowerment. These prerequisites are not met in the case of millions of women migrant workers; their needs and interests remain adjunct. Women migrant workers do not have an interest or incentive in changing societal norms because their presence in the country is temporary. They are a sui generis group – their experience cannot be compared with the empowerment experiences of women citizens who have a long-term incentive in changing their worlds and whose governments and wider society recognise an interest in improving their situations.
Given the above, what is to be done for the sui generis group in theorising their empowerment journey if few of the prerequisites for empowerment are present? Feminist conceptualisations of empowerment – starting at the personal level and aspirant toward harnessing women’s collective agency to challenge gender relations – are not evident within our study. Yet, women migrant workers could and did cope with their SRH needs, although only over the short term. They also managed to stay in employment, earned wages in their host country and remitted these back to their families. They did get what they wanted out of their situations and fulfilled their aspirations, even if they did not organise collectively to further their SRH interests. Many women migrant workers applied to continue their employment, as it was financially lucrative for them to do so. Purely from a feminist point of view, can these women be theorised as empowered peoples, and if so, where along the empowerment journey do they sit? Or are these women not regarded as such, and if so, why not?
Given the centrality of the workplace to women migrant workers’ lives, one avenue open to advocates is invocation of corporate social responsibility (CSR) discourses related to global value chains to exert pressure on factories to be more accommodating of SRH needs. Using Rowlands’ typology of power to analyse whether employment within global value chains empowered women workers in the Kenyan tea and cut flower industries, Said-Allsopp and Tallontire (2015) showed the benefits of supportive management structures in doing so. Concern over company reputation linked to a ‘business case’ enabled HR managers to ensure good labour practices. In our study, some factories did allow NGOs to conduct SRH lectures and workshops for women migrant workers in order to demonstrate their CSR. Others were mindful that whilst they can send women workers back to their home countries, they would also lose the outlay costs paid to recruit these women. Thus, factory goodwill may offer some avenues toward empowering women migrant workers to manage and influence SRH in the workplace.
Calls for CSR scholarship to attend to gender issues in relation to global supply chains and working conditions have increased in frequency and volume (Prieto-Carrón, 2008). CSR viewed as a suite of interlocking governance arrangements (involving civil society, international institutions, business and government) attending to standard-setting, oversight and enforcement could offer a ‘new governance’ framework (Wofford et al., 2016) – and such a regime offers potential for women’s health, including SRH, as a strategic focus area rather than a ‘business case’. External recognition of a company’s CSR has been shown to be a driver for its women’s occupational health and safety management (de Celis et al., 2017) and, while CSR practice already addresses gender issues, feminist theory could more systematically inform CSR scholarship (Grosser and Moon, 2019). This could open new avenues for researchers to explore how women’s advocates can capitalise on CSR to influence working conditions, including SRH provision.
Conclusion
This article’s originality lies in its employment of a feminist lens to document how factory women migrant workers manage health needs in Malaysia. By using a gender lens to reveal the forms of power shaping these women’s ability to manage their SRH, we also open the way to explore how barriers can be addressed both by women and their advocates to effect change. Our contribution is timely given the growing numbers of women who migrate for work – particularly within the global south – in countries with less developed infrastructures. These women’s SRH continues to be overlooked in this part of the world.
Our findings have important implications for research to advance workplace democracy in migrant labour dependent countries such as Malaysia, where strong political and economic interests determine workplace processes and workers’ lives. Strict state policies on migration, combined with highly unequal power structures within the factory, and a large labour surplus which weakens worker bargaining power, severely militate against these women exercising control to accommodate their health needs in the factory. How women migrant workers such as those in our case study, and their advocates, can extend control over the workplace to enhance SRH care are critical research and policy areas. The extent to which health struggles (specifically SRH) inform union advocacy in Malaysia remains a critical issue.
Footnotes
Acknowledgements
A special thanks also to Professors Noraida Endut and Sue Lewis for their roles in the funded research project. The authors would also like to thank anonymous reviewers for their constructive comments on the draft of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors thank the United Nations Gender Theme Group, Malaysia for their generous funding of the project ‘Sexual and reproductive health rights of women migrant workers in Malaysia: NGOs, capacity building and women’s empowerment’, Grant Number 304/PKANITA/650896/U151 – on which we draw.