
Abstract
Anxiety and depression are among the most common mental health concerns in youth, with rates of these internalizing problems continuing to rise. Universal school-based interventions have shown promising results in improving poor mental health outcomes; however, more research is needed across different cultural contexts. This study is part of an ongoing evaluation of A Lust for Life Schools Programme, a universal process-based cognitive behavioral therapy intervention for Irish primary school children. This study investigated the efficacy of the program through a cluster randomized controlled trial. Nine schools were randomly allocated to the intervention or control groups. Four hundred and seventy participants completed measures at three timepoints (baseline, post-intervention, and 6-week follow-up) assessing internalizing problems, anxiety, and depressive symptoms (primary outcomes) and avoidance, problem-solving, seeking social support, academic self-efficacy, social self-efficacy, and emotional self-efficacy (secondary outcomes). Although participants reported that they were mostly satisfied with the intervention, results revealed that the intervention did not have a significant effect on the outcome variables compared to the control group. Implications of the findings and recommendations for future research are discussed.
Keywords
Mental health difficulties often emerge in childhood and adolescence (Paus et al., 2008). It has been reported that one in every seven young people between the ages of 10 and 19 experience a mental health disorder (WHO, 2021). Approximately 50% of adult mental health conditions have their onset before the age of 14 (Kessler et al., 2005), and mental health difficulties experienced in youth increase the risk of psychiatric disorders in adulthood (Caspi et al., 2020). Anxiety and depression are among the most common mental health concerns, with rates of these internalizing problems continuing to rise in youth populations (Michaud & Fombonne, 2005; NHS, 2018). The My World Survey 2 (Dooley & Fitzgerald, 2012), a national survey on youth mental health in Ireland, indicated that anxiety and depression symptoms affect adolescents in the early years of secondary school, with difficulties persisting into later adolescence. The COVID-19 pandemic has also been associated with adverse mental health effects in young people, including increased feelings of depression and anxiety (O'Sullivan et al., 2021; Racine et al., 2020).
Mental health difficulties in childhood and adolescence are associated with lower levels of educational attainment and poorer emotional and social functioning (Bittner et al., 2007; Black et al., 2017). Furthermore, mental health disorders are one of the leading causes of illness and disability throughout the life span (Erskine et al., 2015; Vos et al., 2015), leading to an international recognition of the importance of implementing effective interventions for youth mental health (Kieling et al., 2011). Evidence-based interventions, such as cognitive-behavioral therapy, are effective in treating emotional problems in young people (Compton et al., 2004; James et al., 2020). However, there are many barriers to children accessing appropriate and timely supports (Ford et al., 2003), and many children with emotional disorders will often not receive intervention (Olfson et al., 2003).
School has been identified as one of the most effective settings to implement initiatives to promote positive mental health in young people (Oberle & Schonert-Reichl, 2017). School-based interventions are recommended as initiatives to promote emotional well-being and reduce psychological distress in children and adolescents. Universal school-based programs are delivered to all students regardless of need, whereas selective programs are targeted toward students who have been identified as at risk of mental health difficulties. The advantages of universal programs include having wide reach, potential for reducing stigma, and not requiring the screening needed for selective programs (Humphrey et al., 2011; Pössel et al., 2018).
Systematic reviews and meta-analyses have indicated the effectiveness of universal school-based programs, highlighting positive effects on social and emotional skills, positive mental health, psychological distress, prosocial behavior, and academic achievement (de Pablo et al., 2021; Dray et al., 2017; Sklad et al., 2012). In a meta-analysis of 108 trials, school-based universal and targeted programs demonstrated significant, positive effects on symptoms of depression and anxiety (Werner-Seidler et al., 2021). The authors reported interventions had a small effect on depression and anxiety symptoms and that targeted programs may be more effective than universal programs. Reviews have indicated that optimal outcomes have been achieved for programs implementing a “whole-school” approach (Goldberg et al., 2019; Wells et al., 2003), which involves teacher education, parental liaison, and wider school and community involvement (Waters, 2011).
The overall effectiveness of universal school-based interventions has also been questioned (Spence & Shortt, 2007). Caldwell et al. (2019) found insufficient evidence that school-based interventions were effective for the prevention of anxiety and depression in children and young people in their review of 109 studies. Mackenzie and Williams (2018) concluded that universal school-based interventions had neutral to small significant effects in their systematic review of 12 UK-based programs, with more positive effects found for poorer quality studies. Reviews consistently highlight issues that may affect findings, such as intervention heterogeneity and an overall low quality of studies. These conflicting results in relation to the efficacy of school-based programs have led researchers to caution that the intervention effects reported in reviews may not translate to effectiveness in real settings (Dray et al., 2017). Nonetheless, it has been indicated across reviews that further research is needed to determine the circumstances under which school-based programs will be the most effective.
The majority of reviews have explored programs developed and implemented in USA or Australia, with limited systematic reviews focusing solely on studies conducted within UK or European countries (Mackenzie & Williams, 2018). Although findings from international research are promising, the generalizability of manualized programs to wider educational systems and different cultural contexts remains unclear (Durlak et al., 2011; Humphrey et al., 2016; Sklad et al., 2012). A lack of fit between an intervention and cultural context can act as a barrier to successful implementation (Castro et al., 2004). Furthermore, a lack of cultural adaptability can lessen the effectiveness of school-based programs (Wigelsworth et al., 2016), and evidence-based programs cannot be assumed to work across contexts (Berry et al., 2016). Therefore, there is a need to develop and robustly evaluate school-based programs designed to respond to the psychosocial needs of youth in specific contexts.
Background to the a lust for life schools programme
A Lust for Life (ALFL) Schools Programme is a universal school-based intervention (A Lust for Life, 2019) delivered by teachers to Irish primary school pupils across ten weekly lessons. The ALFL Schools Programme was designed to meet the psychosocial needs of Irish children. The development process was informed by existing evidence in relation to school-based programs and consultations conducted with pupils, their parents and teachers, and a national educational agency.
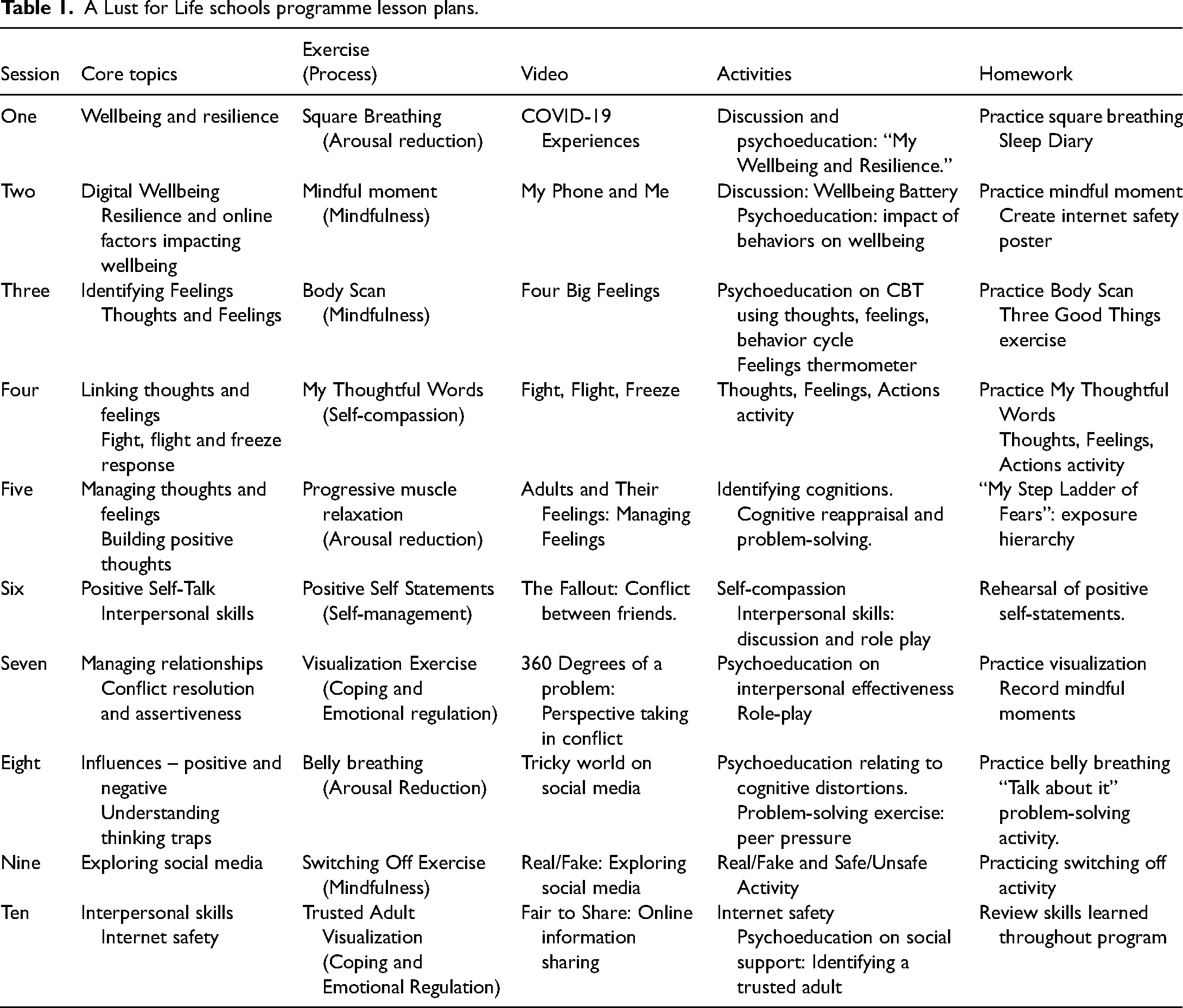
School-based social–emotional programs are more likely to have positive effects if they are sequenced, active, focused, and explicit (i.e., SAFE; Durlak et al., 2011). Therefore, the program delivers a step-by-step training approach (Sequenced) for the experiential exercises in each lesson, in that pupils begin with basic mindfulness skills, such as simple breathing exercises, then gradually move toward more complex skills such as a body scan or visualization. In addition, pupils are provided with psychoeducation about the cognitive behavioral therapy (CBT) model early in the program, then provided with opportunities in subsequent lessons to connect their behaviors to this knowledge in relation to social and emotional skills. The program uses different forms of learning (Active) throughout the lessons, including experiential activities, role-plays, and videos, and provides clear and explicit learning objectives for each lesson (Explicit). Lesson plans for the program set dedicated time for skill development at home by providing a “Try it at home” journal. With support from the pupils’ parents, concepts and tasks are practiced and reinforced outside of school (Focus).
The program is informed by the principles of process-based CBT (PB-CBT; Hayes & Hofmann, 2018). Process-based cognitive behavioral therapy involves the contextually specific use of evidence-based processes of change (e.g., therapeutic skills learning), targeting desirable treatment outcomes to promote well-being and problem-solving (Hofmann & Hayes, 2019). In line with the tenants of PB-CBT, the ALFL Schools Programme aims to support the emotional well-being of pupils through the use of evidenced-based procedures, such as problem-solving techniques, cognitive reappraisal, arousal reduction, and interpersonal skills. To ensure contextually appropriate use of these processes, the intervention involved Irish pupils, teachers, and parents in program development and linked content to the national school curriculum.
The initial evaluation of the ALFL Schools Programme was conducted in 2021 (O’Connor et al., 2022). O’Connor et al. (2022) reconceptualized the ALFL Schools Programme as a PB-CBT intervention underpinned by the extended evolutionary meta-model (EEMM), a theoretical framework for PB-CBT and a model suggested to be applicable to all empirically supported processes of change (Hayes et al., 2020). Extended evolutionary meta-model applies to the key evolutionary concepts of variation, selection, and retention, in a given context, which are focused on biopsychosocial domains and levels (Hayes et al., 2020). The psychological version of the EEMM reflects maladaptive and adaptive processes on a psychological level, organized across six dimensions (affect, cognition, attention, self, motivation, and overt behavior; Hayes et al., 2019), nested within two additional levels (sociocultural and biophysiological). These “dimensions” are understood as the domains in which processes of change are organized. For example, reappraisal is considered a process of change within the dimension of cognition. Likewise, emotional acceptance is considered a process within the dimension of affect. Process-based cognitive behavioral therapy interventions that integrate such theoretically derived processes have the potential to promote positive mental health and reduce psychological distress in youth (Hayes & Hofmann, 2018); however, there is a lack of research focusing on the development and evaluation of such initiatives.
The evaluative framework of the ALFL Schools Programme includes ongoing qualitative explorations of parent, teacher, and student perceptions of the program, in addition to research examining the efficacy of the program on a range of student outcomes (Hoctor et al., 2023; O’Connor et al., 2022). The first evaluative phase of the universal PB-CBT intervention examined the efficacy of the program on measures of positive mental health, resilience, emotional literacy, and mindfulness for early adolescents (O’Connor et al., 2022). The cluster randomized control trial did not support the efficacy of the ALFL Schools Programme on these outcomes and the authors suggested further research would be required to determine the efficacy of the program in improving poor mental health outcomes. Following the initial evaluation, the program was revised in consultation with teachers, pupils, and a steering committee. The revision included extending the program from six to ten lessons and replacing program content to make the intervention more culturally relevant for Irish school children. The program was originally developed for Irish children, and was readapted to include new video content involving Irish pupils and an updated representation of social media applications.
In sum, the ALFL Schools Programme was strengthened by adapting the program to draw from existing theoretical frameworks and appropriately adapting evidence-based procedures to the school context and curriculum, thereby setting up conditions for programs to have the greatest impact (Domitrovich et al., 2008). The development of any complex intervention requires continuous research (Campbell et al., 2000), and this study adds to the ongoing evaluation of a universal PB-CBT intervention newly developed to meet the needs of Irish primary school children. This study builds upon O’Connor et al.'s (2022) evaluation of the universal program and specifically addresses recommendations for future research by investigating the impact of the program on clinical-oriented outcomes.
Aims of the present study
The primary aim of the present study was to examine the effectiveness of the ALFL Schools Programme for reducing symptoms of anxiety and depression, comparing student outcomes of schools randomized to the intervention and control at two time-points: post-intervention and at a six-week follow-up. It was hypothesized that the intervention group would have statistically significant reductions in anxiety and depression symptoms when compared to the control group. The secondary aim was to determine the program's effectiveness for improving coping skills (seeking social support, avoidance, problem-solving) and self-efficacy (social self-efficacy, academic self-efficacy, emotional self-efficacy). It was expected that participants in the intervention group would demonstrate improvements in problem-solving, avoidance, seeking social support, emotional self-efficacy, social self-efficacy, and academic self-efficacy relative to a control group. Post hoc subgroup analyses, exploring the main aims among participants in the medium to high severity range for internalizing symptoms were also conducted to account for the potential of floor or ceiling effects. The present study was preregistered on a public trials registry (ClinicalTrials.gov ID NCT05061381).
Method
Design
The study is part of an ongoing evaluation of the ALFL Schools Programme, which includes a series of qualitative and quantitative research projects aiming to contribute to an understanding of the program's acceptability in Irish primary schools and to guide the program's continued development. A two-arm parallel-group cluster randomized controlled design was conducted with schools as the unit of randomization. A randomized controlled design was chosen with the aim of evenly distributing potential factors that may impact intervention effects across the two groups. A cluster RCT was determined as the best fit, given the intervention was delivered to the entire cluster (i.e., class group) and due to the chance of contamination occurring between trial arms if pupils themselves were randomized (Donner & Klar, 2000). Schools provide a naturalistic environment to deliver mental health initiatives, and cluster randomization is in line with the natural clustering found in the school environment (e.g., multiple classes within the same school year group) (Goesling, 2019). Questionnaires were completed by participants before the intervention, post-intervention, and at a six-week follow-up.
Participants
Participants were 5th and 6th class pupils (10–12 years of age) in Irish primary schools during the academic year 2021/2022. Eligibility criteria for participation included (i) signed parent/guardian consent (ii) participant assent and (iii) enrollment in a primary school in Ireland participating in the trial. An a priori power analysis was conducted in G*Power, which indicated that a total sample size of 260 (130 per group) would provide 95% statistical power at α = .05 to detect a small time × condition interaction effect on the outcome measures. Participating schools were recruited by self-selection between June and September 2021. The recruitment process and participant flow can be seen in Figure 1.
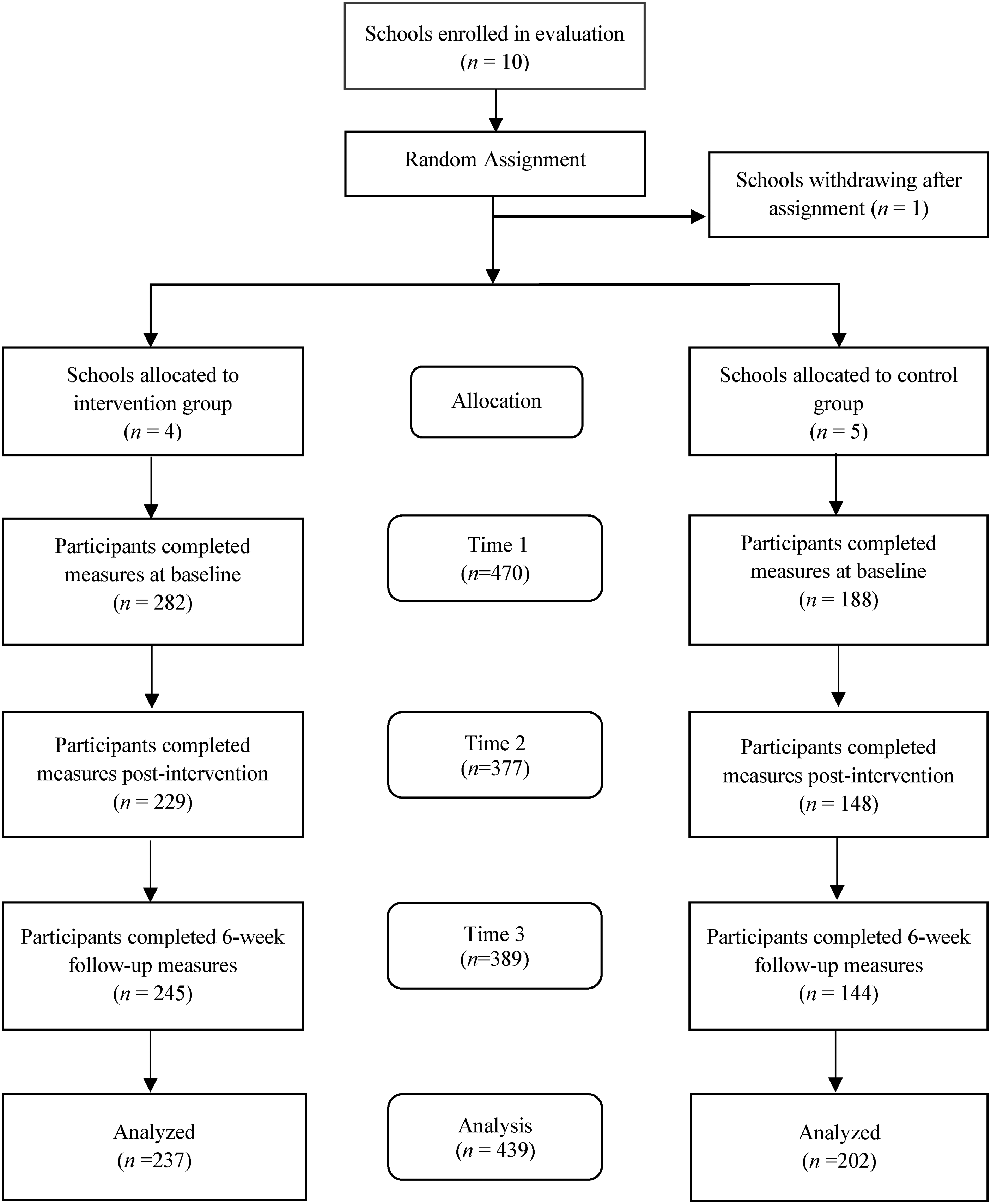
Participant flow.
Procedure
Schools from across Ireland were recruited to participate in the ALFL Schools Programme through online advertisement. Participating schools were provided with details of the program evaluation and were invited to opt-in to participate in the study. Those who expressed an interest in taking part completed a screening survey before registration. Ten Irish primary schools were randomly allocated to intervention or control groups, with school used as the unit of random assignment. Stratified block randomization was conducted to facilitate matching on school characteristics with respect to gender (mixed sex, single sex) and socioeconomic status (as determined by “Delivering Equality of Opportunity in Schools (DEIS)” school status, a national initiative that targets support at disadvantaged communities). Schools were then contacted and informed of their assigned group. Following group allocation, one school within the intervention group withdrew from the study. Randomization was undertaken at the school level, not the class level, to minimize potential contamination within schools. IBM SPSS Statistics was used to randomize schools into the two groups.
All parents of participating schools received an information sheet describing the intervention and the research project. Only students with completed parent/guardian informed consent and informed assent were eligible to participate. Outcome measures were administered to both the intervention and control group through Qualtrics Survey Software at baseline, immediately after the program was delivered to the intervention group, and at a six-week follow-up, and this was supervised by a researcher in the classroom. The control group in this study is considered a waitlist control group, as the intervention was delivered to the group following administration of the six-week follow-up measures. Ethical approval was obtained from the University College Dublin Human Research Ethics Committee – Humanities (Ref HS-21-38).
Intervention
The ALFL Schools Programme involves ten 40-min weekly sessions that are delivered by school teachers in the classroom. The intervention was delivered between October 2021 and February 2022. Due to issues related to the Coronavirus Disease 2019 (Covid-19), not all schools commenced the intervention at the same time and some schools required more than ten weeks to complete the intervention due to teacher absences. Pupils learned coping skills for managing difficult emotions, problem-solving, and conflict resolution through interactive teaching strategies. Each session involved a mindfulness or experiential exercise, a video, and individual and classroom-based activities. Irish primary school children were involved in the production of program content and filming of videos. Table 1 provides a description of each of the ten lesson plans. Before delivering the program, teachers were directed to watch training videos accessed through the teacher portal of the ALFL Schools Programme website. Training videos and a detailed teacher guide provided psychoeducation, intervention targets, and signposting for additional resources. As materials were accessed online, it was not known which teachers engaged with training videos. The sessions were provided by the teacher and did not include any external input from the researcher.
A Lust for Life schools programme lesson plans.
Measures
The primary outcome was symptoms of anxiety and low mood as measured by the short version of the Revised Child Anxiety and Depression Scale-25 (RCADS-25; Ebesutani et al., 2012). Secondary outcomes were measured using the Coping Strategy Indicator (CSI; Amirkhan, 1990) and the Self-Efficacy Questionnaire for Children (SEQ-C; Muris, 2001).
The RCADS-25 is a 25-item scale measuring levels of anxiety and low mood in children and adolescents. The scale has two subscales (Total Anxiety and Total Depression) and an overall score (Total Internalizing) (Ebesutani et al., 2012). Question items are scored on a four-point Likert scale from 0 to 3. The subscales of the RCADS-25 demonstrated acceptable reliability both in clinic and school samples. Cronbach's alpha (α) for the RCADS-25 (α = .92; Muris et al., 2002) was reported to have “excellent” internal consistency. In the present study, the measure displayed good internal consistency (Total Internalizing α = .92, Total Anxiety α = .87, Total Depression α = .86). The construct validity for the two subscales of the RCADS-25 was established through hypothesis testing in previous research (Klaufus et al., 2020).
The CSI (Amirkhan, 1990) is a 33-item scale that measures three coping strategies: the subscales of seeking social support, problem-solving, and avoidance. Respondents are asked to indicate the extent to which they used the different coping strategies to deal with a stressful event within the last six months, through the use of a three-point scale (“A lot,” “A little,” or “Not at all”). Responses are combined to form the three scales, which relate to the different coping strategies. While the measure was originally developed for adults, Amirkhan and Auyeung (2007) provided psychometric support for using the CSI with child populations. Cronbach's alpha (α) demonstrated high levels of internal consistency for the three subscales for the “Pre-teen” group (seeking social support α = .96, problem-solving α = .94, and avoidance α = 0.92; Amirkhan & Auyeung, 2007). The subscale measures displayed adequate internal consistency in the present study (seeking social support α = .88, problem-solving α = .85, and avoidance α = 0.79).
The SEQ-C (Muris, 2001) is a 24-item measure for youth that consists of three subscales: social self-efficacy (ability to relate and get along with peers), academic self-efficacy (ability to do well in school and engage in appropriate learning behaviors) and emotional self-efficacy (ability to regulate difficult emotions). Each of the three subscales includes eight items in which participants answer on a 5-point scale (1 = not at all, 5 = very well). Cronbach's alpha (α) demonstrated satisfactory internal consistency (total self-efficacy score α = .88, and between .85 and .88 for subscale scores). In the present study, the subscale measures demonstrated adequate internal consistency (academic self-efficacy α = .83, social self-efficacy α = .79, and emotional self-efficacy α = .85).
Satisfaction with intervention was measured post-intervention with a Brief Satisfaction Scale (O’Connor et al., 2022), a program-specific measure of satisfaction developed for the original evaluation of the program. The scale includes eight items that are rated on a seven-point scale from 1 (strongly disagree) to 7 (strongly agree). Higher scores on the scale signify higher levels of satisfaction with the program.
Intervention fidelity
A fidelity checklist was provided to monitor the fidelity with which the program was delivered by the teachers. Each fidelity checklist for the ten lessons specified all lesson components with a tick box to indicate whether it had been completed. Following each session, teachers ticked appropriate boxes to confirm that each part of the program had been delivered and specified if any adaptations of content were made. A total adherence rating was given for each lesson. Mean ratings for intervention fidelity are shown in Table 2. Results show an overall high level of intervention fidelity. The National Institute of Health Behavior Change Consortium defined high fidelity as 80–100% adherence to program checklist, whereas 50% constitutes low fidelity (Borrelli et al., 2005). Only one lesson did not reach high fidelity and would still be classified as medium fidelity. While self-reported program fidelity was in the medium to high range, only two out of the ten teachers who completed the checklists covered the “Try at Home” activity in every lesson, while two out of ten teachers omitted explaining the homework practice entirely in all ten lessons.
Mean fidelity ratings recorded for each lesson.
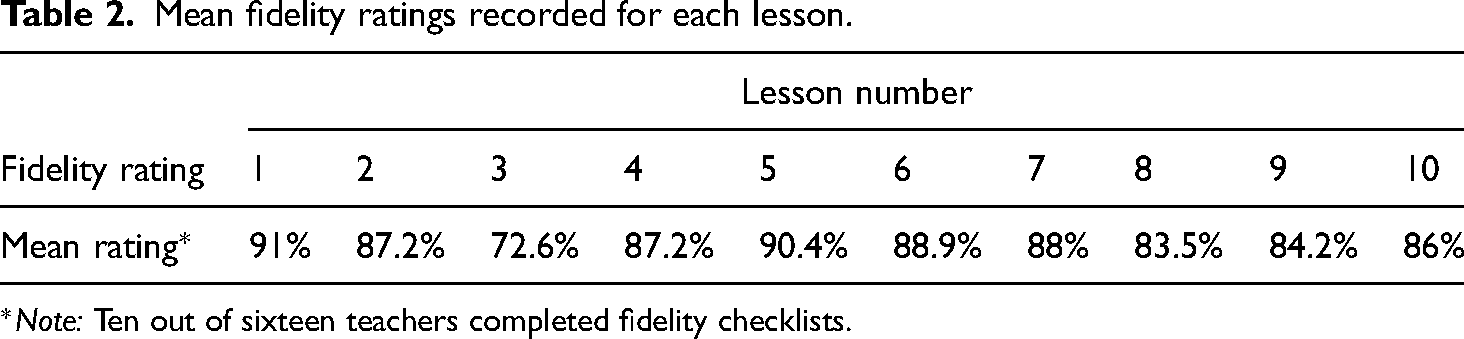
Note: Ten out of sixteen teachers completed fidelity checklists.
Data analysis
Intention-to-treat (ITT) analysis was conducted in this study by using all available participant data. Participants with data at baseline and data at one or both of post-intervention or six-week follow-up assessments were used in the analysis, regardless of participant characteristics or how much of the intervention a participant received (Hill, 1961). The Qualtrics survey was designed so if a participant skipped an item in any questionnaire, they were prompted to answer the item before they could progress to the subsequent questionnaire. This resulted in entire outcome measures being fully completed before being submitted to Qualtrics, reducing the likelihood of missing data within a questionnaire. Outcome measures not completed by participants were considered missing data and handled with listwise deletion. To reduce the impact of this on analyses, multilevel models were fitted that incorporated available participant data.
The linear mixed-effects models (MIXED) procedure in IBM SPSS Statistics 26 (IBM Corp, 2019) was conducted for repeated measures analyses of primary and secondary outcome measures. The MIXED procedure facilitates modified ITT analysis by using all available data. In comparison to standard linear regression models, mixed models have the advantage of managing missing data points and accounting for the likelihood of data points not being independent of each other. MIXED extends repeated measures models used in General Linear Model procedures to handle situations in which experimental units are nested in a hierarchy (Heck et al., 2014). For this multilevel analysis, time-points were nested within participants, who were located in trial group conditions (intervention vs control). For each outcome, mixed-effects linear regression models were developed with fixed effects for time (baseline, post-intervention, and the six-week follow-up), group condition (intervention and control), and their interaction (time × condition), in addition to random effects for time. Mixed-effects models account for data clustering by including random effects in the analysis (McNeish & Kelley, 2019; Stiratelli et al., 1984).
T-scores were calculated for participants’ scores on the total internalizing scale, and the anxiety and depression subscales of the RCADS-25 (Chorpita et al., 2000). A subgroup analysis was completed for those participants who were in the medium to high severity range for internalizing symptoms (i.e., T-score of >65 on the RCADS-25) using the linear mixed effects procedure for each of the primary and secondary outcome measures.
In line with recommendations in the Consolidated Standards of Reporting Trials statement (Moher et al., 2012), significance testing of baseline differences was not performed. Statistical literature points to the inappropriateness of using significance testing in randomized controlled trials (Austin et al., 2010), inferring that using p-values for baseline differences serves no useful purpose and can be misleading (Pocock et al., 2002). The process of randomization in a randomized trial indicates that testing is occurring between two samples from the same population, and any resulting p-value can be considered to be random (De Boer et al., 2015).
Results
Participant characteristics
Sociodemographic characteristics at baseline are displayed in Table 3. Data were provided by 470 participants at baseline. Of those 470 participants, 377 participants provided data post-intervention (attrition rate 19.79%) and 389 participants provided data at six-week follow-up (attrition rate 17.23%). Reasons for drop-out were largely due to students being absent on days of follow-up data collection. Data from 439 participants (including those with data at baseline, and data at one or both of post-intervention and follow-up) were used in the main analysis. Scores from 56 participants fell in the medium to high severity range for internalizing symptoms at time 1 (intervention, n = 37; control, n = 19), and these participants were included in the subgroup analyses.
Baseline characteristics of participants in Irish primary schools.
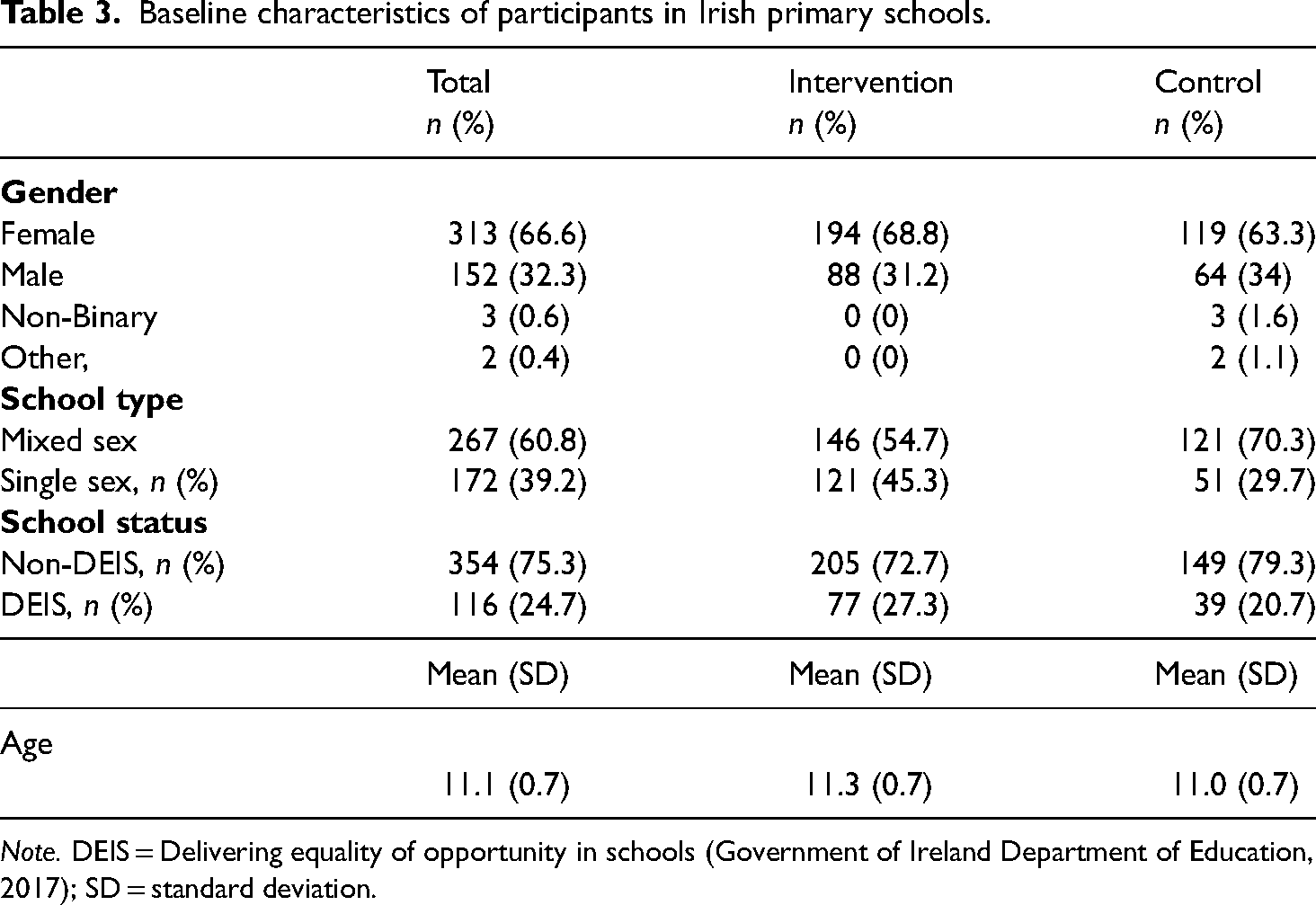
Note. DEIS = Delivering equality of opportunity in schools (Government of Ireland Department of Education, 2017); SD = standard deviation.
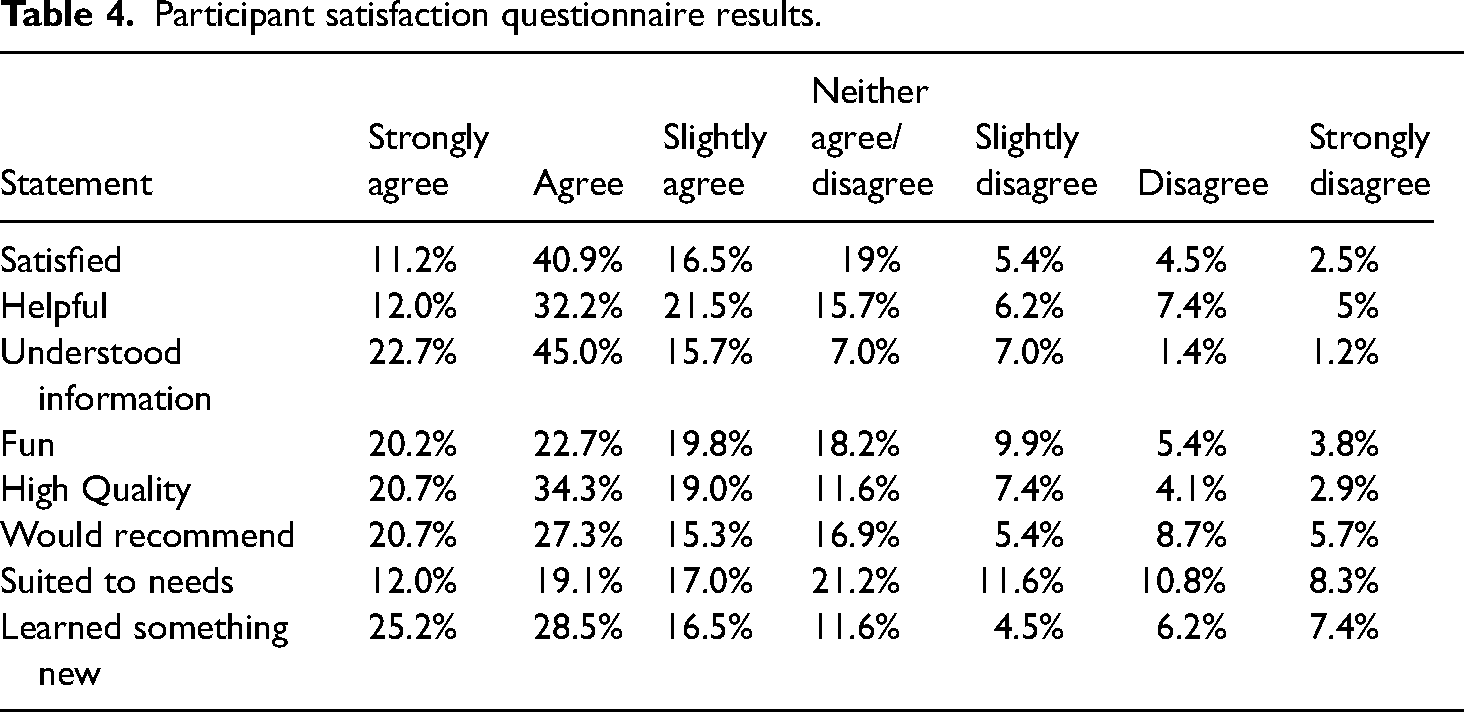
Participant satisfaction
Results of the analysis of satisfaction with the ALFL Schools Programme by the intervention group are displayed in Table 4. A combined 68.6% of participants strongly agreed/agreed/slightly agreed that they were satisfied with the ALFL Schools Programme, 65.7% of participants strongly agreed/agreed/slightly agreed that it was helpful, and 83.4% of participants strongly agreed/agreed/slightly agreed that they understood most of the information in the program. A combined 62.7% of participants strongly agreed/agreed/slightly agreed that the program was fun, 74% of participants strongly agreed/agreed/slightly agreed that the program was of high quality and 63.3% of participants strongly agreed/agreed/slightly agreed that they would recommend it to a family member or friend. Finally, a combined 48.1% of participants strongly agreed/agreed/slightly agreed that the program was suited to their needs and 70.2 of participants strongly agreed/agreed/slightly agreed that they learned something new.
Participant satisfaction questionnaire results.
Primary outcome measures
Table 5 shows the mean scores and T-scores for the outcome variables at all three time points for the intervention and control groups. A multilevel model analyzing variability in internalizing problems trajectories between the intervention and control groups revealed no statistically significant time × condition interaction, β = −1.39, p = .114, 95% confidence interval (CI) [−3.12, 0.34]. Similarly, no statistically significant time × condition interaction in anxiety symptom trajectories was detected β = −0.94, p = .09, 95% CI [−2.03, 0.15]. A multilevel model investigating variability in depression symptom trajectories also revealed no statistically significant time × condition interaction β = −0.38, p = .317, 95% CI [−1.12, 0.36].
Mean scores and T-scores for outcome variables for intervention and control groups.
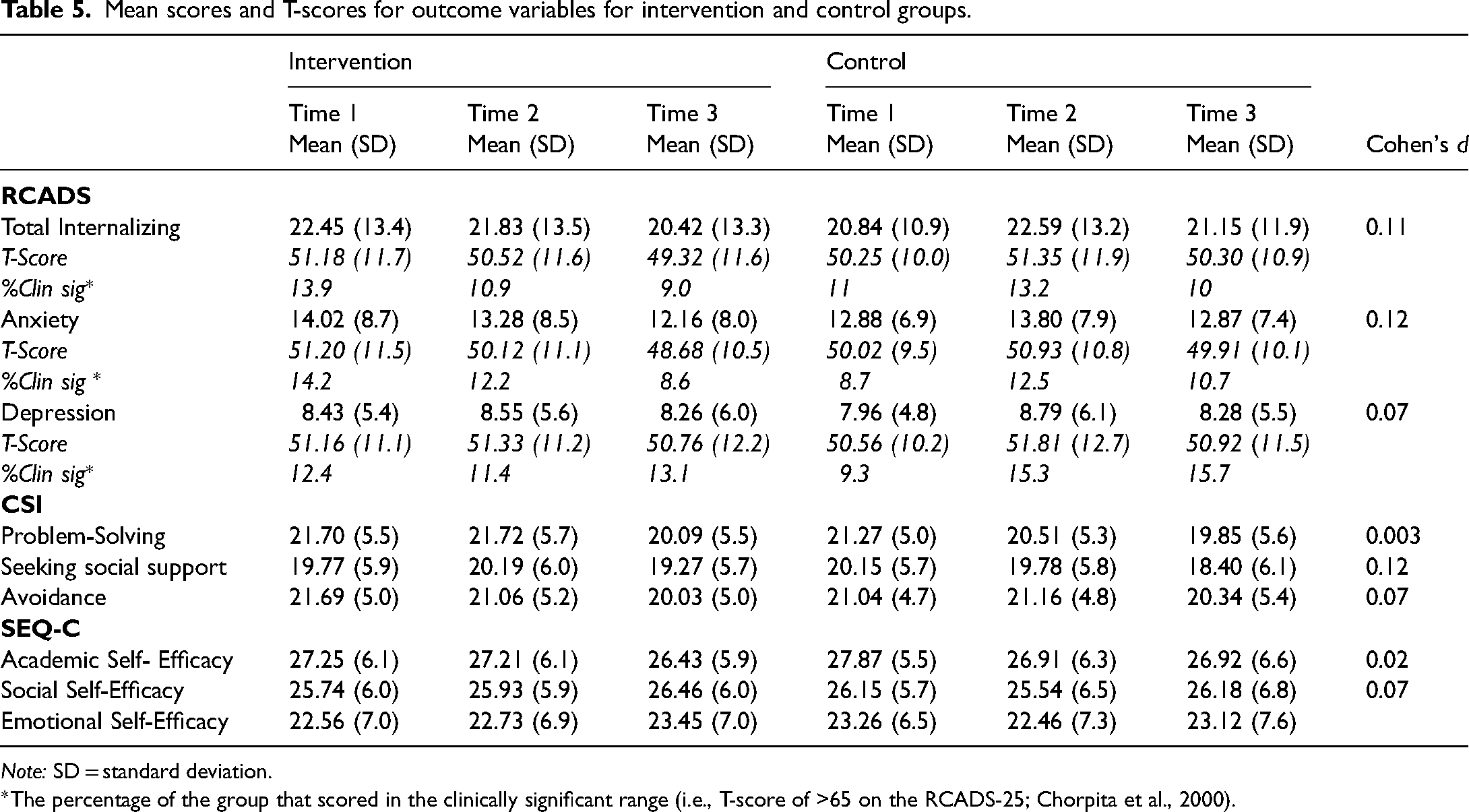
Note: SD = standard deviation.
The percentage of the group that scored in the clinically significant range (i.e., T-score of >65 on the RCADS-25; Chorpita et al., 2000).
Secondary outcome measures
The variability in problem-solving growth rates between the intervention and control groups was analyzed with a multilevel model, which revealed no statistically significant time × condition interaction, β = −0.015, p = .968, 95% CI [−0.75, 0.72]. Similarly, no statistically significant time × condition interaction in seeking social support rates was found, β = 0.7, p = .083, 95% CI [−0.9, 1.48]. For avoidance, a multilevel model detected no statistically significant time × condition interaction between the intervention and control groups, β = −0.36, p = .301, 95% CI [−1.03, 0.32].
The variability in academic self-efficacy rates between the treatment and control groups was investigated with a multilevel model, which indicated no statistically significant time × condition interaction, β = 0.12, p = .775, 95% CI [−0.7, 0.93]. Similarly, no statistically significant time × condition interaction in social self-efficacy was revealed β = 0.51, p = .224, 95% CI [−0.31, 1.32]. A multilevel model investigating variability in emotional self-efficacy also revealed no statistically significant time × condition interaction, β = 0.47, p = .331, 95% CI [−0.48, 1.42].
Subgroup analyses
A subgroup analysis was completed for participants who were in the medium to high severity range for internalizing symptoms on the outcome measures of internalizing problems, anxiety, depression, problem-solving, seeking social support, avoidance, academic self-efficacy, social self-efficacy, emotional self-efficacy, and the pattern of results for these outcomes were comparable to findings from the main analysis. Results for the subgroup analyses are included in Appendix 1.
Discussion
This cluster randomized controlled trial evaluated the effectiveness of a universal school program for internalizing problems, coping strategies, and self-efficacy in Irish primary school children. There was no statistically significant difference between the intervention and control group for any of the primary or secondary outcomes. Therefore, the hypothesis that the intervention group would demonstrate a greater reduction in total internalizing problems, anxiety, and depression scores compared to the control group was not supported. Similarly, the findings did not support the hypothesis that the intervention group would show a greater improvement in problem-solving, seeking social support, avoidance, academic self-efficacy, social self-efficacy, or emotional self-efficacy. Subgroup analyses revealed no statistically significant difference between the intervention and control group for primary and secondary outcome measures.
Research has highlighted the importance of developing and evaluating culturally sensitive universal school-based programs, particularly within European contexts (Mackenzie & Williams, 2018; Sklad et al., 2012). This study evaluated a PB-CBT intervention developed within an Irish context and extended the initial evaluation of the ALFL Schools Programme to evaluate the impact of the intervention on internalizing problems, coping strategies, and self-efficacy in Irish primary school pupils. The results of the current study are in line with the findings of O’Connor et al. (2022), who did not find support for the efficacy of the program in promoting mental health in primary school children. Similar to the initial evaluation, the majority of participants in the present study were experiencing subclinical levels of psychological distress and functioning well at baseline. This likely resulted in a “floor” or “ceiling” effect in the sample population whereby there was little room for improvement in outcomes (Clarke et al., 2014; Gresham, 2017). Although such an effect may contribute to comparable outcomes from control and intervention groups, research has suggested that, despite floor effects, universal programs can demonstrate positive outcomes (Reavley et al., 2015; Stallard et al., 2014). Nonetheless, the effects of universal programs may be reduced when compared to targeted programs (Werner-Seidler et al., 2021), as there is more potential for improvement in children who are at risk of, or already displaying symptoms. As floor and ceiling effects are recognized as an expected occurrence among students targeted by universal programs, subgroup analyses, focused on participants reporting medium to high internalizing symptoms, were also conducted. Effects were not significant for these analyses; however, note that the number of participants with clinical levels of internalizing problems was small, and the present study was not powered to examine time × condition interactions within this subgroup.
The findings of the current study contrast with previous findings reported in systematic reviews, which indicate the positive effects of universal school programs on psychological distress, anxiety, and depression (Dray et al., 2017; Werner-Seidler et al., 2021), coping skills (Kraag et al., 2006), self-perceptions, such as self-efficacy, and social skills (de Pablo et al., 2020; Durlak et al., 2011). Conversely, the current findings are consistent with reviews that did not support the efficacy of school programs for reducing anxiety and depression symptoms (Bastounis et al., 2016; Caldwell et al., 2019). Previous literature exploring the effectiveness of school-based interventions has highlighted the role of methodological and implementation factors as contributing to varying intervention effects. Therefore, further exploration is required to determine possible mechanisms contributing to the current findings.
Another explanation for the nonsignificant findings may be due to the classroom-based model of the intervention. Research suggests that brief, isolated interventions at the class level may not be sufficient, and that for optimal and enduring effects, program components need to be embedded within a wider “whole school” approach positioned at the school and community level (Goldberg et al., 2019; Shoshani & Steinmetz, 2014; Weare & Nind, 2011). However, a school-wide approach requires more resources, making it challenging for schools to undertake. For the ALFL Schools Programme, this study's findings may point to a need for an integrated, sequenced approach of program delivery in the later primary school years as the program progresses to being delivered from 3rd to 6th classes (ages 9–12 years), in combination with strategies to foster mental well-being at the school and community level. The involvement of parents is an area of development within the program's evaluative framework, and the addition of a direct parental component would not only align with a whole school model of delivery but may support students’ focused learning of skills. Hawkins and James (2018) conceptualize schools as evolving and interacting complex human systems. The authors note this includes students, staff, parents, and wider systems and that there is potential for substantial and influential interactions between these groups, supporting the need for a whole school approach for school-based programs.
It is also necessary to consider factors relating to the implementation of the program that may have interfered with the program's integrity. While the program was being delivered, the COVID-19 pandemic. The attendance of pupils was not recorded; however, it was reported by teachers that there was a high level of COVID-19-related student and teacher absences throughout the intervention. As a result, program delivery was not always delivered on a weekly basis. Research further indicates that COVID-19-related school issues negatively impact learning outcomes in children (Kuhfeld et al., 2022) and it is possible that such disruptions to program delivery may have impacted student's ability to learn key concepts and practice skills in school and at home.
In addition, while self-reported program fidelity was high, the “Try at Home” activity was not consistently explained or covered in the lessons, with some teachers omitting the homework assignments in all ten lessons. An integral component of the intervention is repetition and practicing newly acquired skills (Ramdass & Zimmerman, 2011); therefore, if these skills were not reinforced or encouraged to be practiced at home this might have compromised the program's effectiveness. However, it is unclear whether the program skills were being practiced in the school classroom outside of weekly lessons and it is not possible to draw strong inferences as not all teachers completed fidelity checklists.
Structured teacher training is not offered explicitly for teachers providing the school program. Despite teachers being directed to videos prior to delivering the program, their engagement and participation was not monitored. Fenwick-Smith et al. (2018) reported greater intervention effects when teachers received ongoing support and training while delivering interventions. Providing teachers with more rigorous training and supervision may have a significant impact on program implementation, including enhanced delivery of techniques, higher program fidelity, and improved monitoring and completing homework tasks. Program implementation is a crucial component in school-based interventions (Durlak & DuPre, 2008), and the findings of this study offer further support for the need to consider the active ingredients of school-based programs and the processes involved in their implementation when developing novel school-based interventions.
Despite the aims of the program aligning with SAFE characteristics (i.e., Sequenced, Active, Focused, Explicit; Durlak et al., 2011), the outlined issues with homework completion and implementation may have resulted in insufficient time being devoted to skills for learning and consolidation to occur. Moreover, different intervention components may not have been intensive enough over the ten lessons to learn and apply skills in practice. While the program provided some sequenced learning, the program materials offered less repetition in relation to skill development and homework practice across the ten lessons. Further developments of the program could adapt program components to align more closely with SAFE characteristics.
Limitations
There were several limitations found in this study. Firstly, self-reported questionnaires were used, which can lead to reporting bias in participants (Shoshani & Steinmetz, 2014). Moreover, the present study only included perceptions of school children but collecting data from multiple respondents can improve data quality (Schniering et al., 2000). Future research could obtain parent or teacher report measures to increase the reliability of the data gathered in the current study. Secondly, the majority of schools included in this study were from urban areas in Ireland (eight out of nine schools). Therefore, the findings do not represent children in more rural locations and may not generalize to wider populations. Thirdly, program fidelity was self-reported, and there was no direct assessment of how the program had been delivered and as a result there may have been differences in content delivery. There was also no assessment of homework practice or pupils’ understanding of the homework. Note, however, the current approach may be more generalizable to the real-world setting. No difficulties have been identified with using the CSI with similar populations in previous studies (Amirkhan & Auyeung, 2007; Collins et al., 2014).
A further limitation is associated with the cluster randomized controlled design of the study. Compared to a trial randomized at the individual level, this approach can impact the balance between the intervention and control groups and decrease the precision of study findings (Dron et al., 2021). Stratified block randomization was implemented to help address this limitation, through randomization of clusters by gender and socioeconomic status. In addition, clustered designs can reduce the statistical power of the study (Brown et al., 2015; Leyrat et al., 2018). The statistical power of the study to detect a small effect was reduced when considering the clustered nature of the sample, and the analysis may have not found an effect given the reduced statistical power. These limitations are also true for subgroup analyses, which were limited by a small sample size (n = 56).
Implications
The present study offers guidance for school psychologists who are involved in the implementation of school-based programs. While the findings did not provide evidence that implementing the program improved outcomes in children, findings do inform several considerations for the development and delivery of the program and wider school-based interventions. School psychologists can play a role in the design and implementation of school-based programs by working with school staff and administrators to identify interventions that include adequate training components for teachers, or indeed provide training and support to staff implementing programs. Although requiring further exploration, the findings also intimate the importance and role of homework activities and SAFE characteristics for effective interventions. As such, school psychologists can work with other educational professionals to develop comprehensive mental health and well-being interventions that focus on skill learning and consolidation or can use this information to advocate for the implementation of appropriate interventions in their school district.
Future directions
Due to the program's ongoing development and widespread implementation in Ireland, there is a need for continued research to determine the effects of the universal program. Future research may address program implementation factors previously discussed. Adopting a whole school approach, in combination with the ALFL in-class lessons, may support children's learning and well-being at a wider level. Given that schools have removed COVID-19 social restrictions and are reengaging with former procedures, it may be helpful to replicate evaluations of the program without the discussed COVID-19-related issues. Future research may explore the impact of more rigorous teacher training, program fidelity, and homework practice. It may also be helpful to investigate the efficacy of the program with selective or indicated populations.
Conclusion
In conclusion, the findings of the current study did not support the efficacy of the PB-CBT intervention in reducing internalizing problem or improving coping skills or self-efficacy in Irish primary school children. Although the ALFL Schools Programme is based on evidence-based processes of change, there is currently no evidence that supports the program's effectiveness across a range of mental health outcomes. Given the ongoing development of the PB-CBT intervention, further research is needed to evaluate program effectiveness inclusive of these adaptations. Methodological and program implementation factors may also be explored in future research. This study contributes to the ongoing evaluation of the ALFL Schools Programme, a culturally sensitive PB-CBT intervention, and to the research evidence in relation to universal school-based interventions.
Supplemental Material
sj-docx-1-spi-10.1177_01430343231216971 - Supplemental material for Effectiveness of a universal school-based intervention for reducing internalizing problems in irish primary school children: A cluster randomized control trial
Supplemental material, sj-docx-1-spi-10.1177_01430343231216971 for Effectiveness of a universal school-based intervention for reducing internalizing problems in irish primary school children: A cluster randomized control trial by Aoife Clancy, Martin O’Connor, Eddie Murphy, Leda Connaughton and Gary O’Reilly in School Psychology International
Supplemental Material
sj-docx-2-spi-10.1177_01430343231216971 - Supplemental material for Effectiveness of a universal school-based intervention for reducing internalizing problems in irish primary school children: A cluster randomized control trial
Supplemental material, sj-docx-2-spi-10.1177_01430343231216971 for Effectiveness of a universal school-based intervention for reducing internalizing problems in irish primary school children: A cluster randomized control trial by Aoife Clancy, Martin O’Connor, Eddie Murphy, Leda Connaughton and Gary O’Reilly in School Psychology International
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The corresponding author is currently completing her doctorate in clinical psychology. An external agency (Health Service Executive, HSE) annually funds the training of doctoral students in clinical psychology which requires University College Dublin to assign a supervisor to these students and the funder specifies the area of research it would like investigated (i.e. the Lust For Life schools programme). This funding corresponds to salaried employment as a Trainee Clinical Psychologist within the HSE and does not correspond to funding of the student's research project.
Ethical approval
Ethical approval was obtained from the University College Dublin Human Research Ethics Committee – Humanities. Ref: HS-21-38-Clancy-OReilly.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.