
Abstract
The purpose of this study was to compare the impact of two teacher trainings, both focused on identifying student anxiety and implementing empirically supported anxiety reduction strategies in the classroom. A comparison of teachers’ satisfaction with their training was examined along with pre–post training changes on measures of teachers’ knowledge and use of evidence-based anxiety reduction strategies, perceived confidence in assisting students with anxiety, and teaching self-efficacy. Volunteer elementary teachers in New England USA were randomized to receive either a six-hour interactive training (Teacher Anxiety Program for Elementary Students; TAPES; n = 41) or a three-hour didactic (Teacher Anxiety Training; TAT; n = 37). Fifty-four teachers completed their respective training (mean age 40.9; SD = 10.2; 98% female; 96% White). Results from t-tests indicated that levels of training satisfaction were high and similar across trainings. Mixed-design ANOVA analyses found that teachers receiving both trainings showed significant improvements in teacher knowledge and use of anxiety reduction strategies, confidence, and self-efficacy. Teachers receiving TAPES, compared to TAT, showed greater improvements in their knowledge of anxiety reduction strategies. Findings highlight the need and perceived value of training teachers on topics related to identifying and managing student anxiety.
Keywords
Introduction
Excessive anxiety is among the most common form of pediatric psychopathology in the United States of America (USA) and globally and impairs academic functioning (Battaglia et al., 2017; Ghandour et al., 2019; Racine et al., 2021; Swan & Kendall, 2016). Students with anxiety present challenges to teachers who are tasked with managing their students’ social, emotional, behavioral, and educational impairment caused by excessive anxiety. For instance, data show that students with higher (compared to lower) levels of anxiety are more dependent on, and have more conflict with, their teachers (Zee & Roorda, 2018), and a majority of teachers report that student anxiety negatively impacts their classrooms (Birnbaum et al., 2017). While teachers are not responsible for diagnosing student anxiety, their accurate observations of student anxiety often affect their teaching methods (i.e. how they respond to students in the classroom to optimize their learning); moreover, teachers may refer a student to a school mental health professional. The mental health needs of students internationally have risen dramatically in light of the global COVID-19 pandemic, highlighting the likelihood that teachers globally will encounter excessive student anxiety (Chavira et al., 2022; World Health Organization, 2022).
In many countries, federal regulations mandate schools provide supports for students with emotional, behavioral, developmental, or learning challenges that interfere with learning. For students in the USA, a student with an anxiety disorder may have an Individualized Education Program (IEP), a 504 Plan, or specific classroom modifications (e.g. sitting next to the teacher, frequent breaks to see the nurse or counselor; additional time to complete tests; not presenting in front of the class). However, most students with excessive anxiety do not receive any supports or interventions (Merikangas et al., 2010; Olfson et al., 2015). Moreover, some evidence indicates that school-based supports present in IEP or 504 Plans for students with anxiety may actually be at odds with long-term anxiety reduction (Conroy et al., 2020; Phillips et al., 2022) These data support the need for additional training in evidenced-based anxiety reduction strategies for school-based personnel. Despite the challenges that students with anxiety present to teachers, teacher training on how to identify and reduce student anxiety is lacking (Sindelar et al., 2010). Recent data from a small sample of elementary teachers (N = 51) who took a knowledge test on student anxiety revealed that the average score was 57% correct (Ginsburg et al., 2022). Moreover, teachers themselves report a need for more training and support in this area (Maclean & Law, 2022; Moon et al., 2017). The consequences of this gap in teacher knowledge and skills related to anxiety management can be grave for both teachers and students. Teachers with minimal training in identifying and managing students’ anxiety are less likely to feel efficacious and may engage in teaching practices that maintain anxiety, such as allowing students to avoid what they are frightened of (e.g. reading a loud in class). Allowing students to avoid anxiety provoking situations, a term in the psychological literature known as accommodation of anxiety and referred to throughout this manuscript, is associated with higher student anxiety (Ginsburg et al., 2022).
Although the vast majority of teachers never receive any training in evidence-based strategies for identifying and assisting students with excessive anxiety (Reinke et al., 2011), meta-analyses indicate that, with adequate training and coaching, teachers can effectively deliver “universal” classroom-based social-emotional curricula with numerous positive effects on student outcomes (Werner-Seidler et al., 2017). To the best of our knowledge, only one teacher-led anxiety specific intervention, called FRIENDS (Anticich et al., 2013; Barrett et al., 2005; Barrett & Turner, 2001) has been evaluated (research groups in Australia, Canada, and the UK), and evidence for its effectiveness on students is mixed; moreover, no evaluation of the training's impact on teachers’ knowledge or behavior has been reported.
No study has investigated the effectiveness of anxiety specific trainings on teachers’ knowledge and skills. However, a growing literature has investigated the effects of general mental health training for teachers. Anderson et al. (2019) conducted a systematic review of the effectiveness of mental health training programs on improving teacher knowledge (e.g. of adolescent depression, anxiety and other related mental health concerns). Of the eight studies identified, all reported an improvement in mental health knowledge and attitudes toward mental health at post training using teacher report questionnaires. For instance, Kutcher et al. (2016) evaluated the mental health literacy knowledge of 38 secondary school teachers before and after a 3-day mental health literacy training course. Mental health literacy, defined as “knowledge and beliefs about mental health problems which aid their recognition, management or prevention” (Jorm et al., 1997), was assessed using a teacher completed knowledge assessment survey. Results indicated that after training, teachers’ scores on the knowledge survey increased significantly and that 84% of teachers reported that they had identified a student who had a mental health disorder or mental health problem. While this study shows teachers’ ability to learn information about mental health, it did not include a comparison training group and no follow-up was conducted regarding the accuracy of teacher identified students.
In a larger study, Long et al. (2018) examined the impact of an online mental health role-play simulation on changes in teachers’ attitudes and self-reported helping behaviors for students experiencing psychological distress. Elementary school teachers (N = 18,896) were randomly assigned to a 45–90-minute online training or a wait-list control. In the intervention condition, the role-play simulation taught motivational interviewing (MI) skills with a virtual student and parent experiencing psychological distress. The Gatekeeper Behavior Scale, which assessed attitudinal dimensions (i.e. preparedness, likelihood to implement and self-efficacy in implementing interventions with students and parents) was administered at baseline and post training (three months later). Results demonstrated that post-training scores in the intervention group were significantly higher than the wait list control group on all attitudinal dimensions measures. Similar to Kutcher et al. (2016) and other studies, findings demonstrate that with training, teachers are able to retain new knowledge of skills related to mental health. However, although studies report an improvement in teacher knowledge and attitudes, little evidence suggests that programs improve teachers’ behavior in regard to helping students’ mental health. Further, none of these studies have examined the impact of an anxiety-specific training on elementary school teachers’ knowledge and behavior.
To further contribute to the literature on teacher training on mental health, we developed two teacher trainings as part of a larger study to examine the effects of a teacher-led home-school intervention for student anxiety (Ginsburg et al., 2019). Both trainings focused on the assessment of student anxiety and evidence-based intervention strategies for reducing anxiety that could be applied to students and in the classroom. The current study compared teachers’ satisfaction with these two trainings (described below) as well as the pre-post impact (i.e. after 10 weeks) of these trainings on teachers’ knowledge of student anxiety, use of evidence-based anxiety reduction strategies (including reductions in their own accommodation of anxiety), perceived confidence in assisting students with anxiety and teaching self-efficacy. The first training, referred to as the Teacher Anxiety Program for Elementary Students (TAPES) was a six-hour interactive training. The second training was referred to as the Teacher Anxiety Training (TAT) and was a three-hour didactic training that was developed to serve as a comparison condition that mimicked typical teacher professional development seminars. Considering the literature showing that interactive trainings (e.g. those using role plays and corrective feedback) enhance learning (Fixsen et al., 2005; Sholomskas et al., 2005), we hypothesized that while teachers in both trainings would demonstrate an increase in knowledge, skills (including reductions in anxiety accommodation), confidence, and self-efficacy; those teachers who received the TAPES training would show greater gains relative to those who received TAT.
Methods
Participants
Fifty-four public elementary school teachers in New England USA were randomized and trained in TAPES (n = 28) or TAT (n = 26). Demographic and professional characteristics of the 54 teachers and comparisons by group (TAPES vs. TAT) are presented in Table 1. Teachers instructed kindergarten (n = 9), first (n = 9), second (n = 1), third (n = 15), fourth (n = 8), and fifth (n = 6) grades, and six were special education teachers.
Teacher demographics and professional characteristics (n = 54) n (%) or mean (SD).
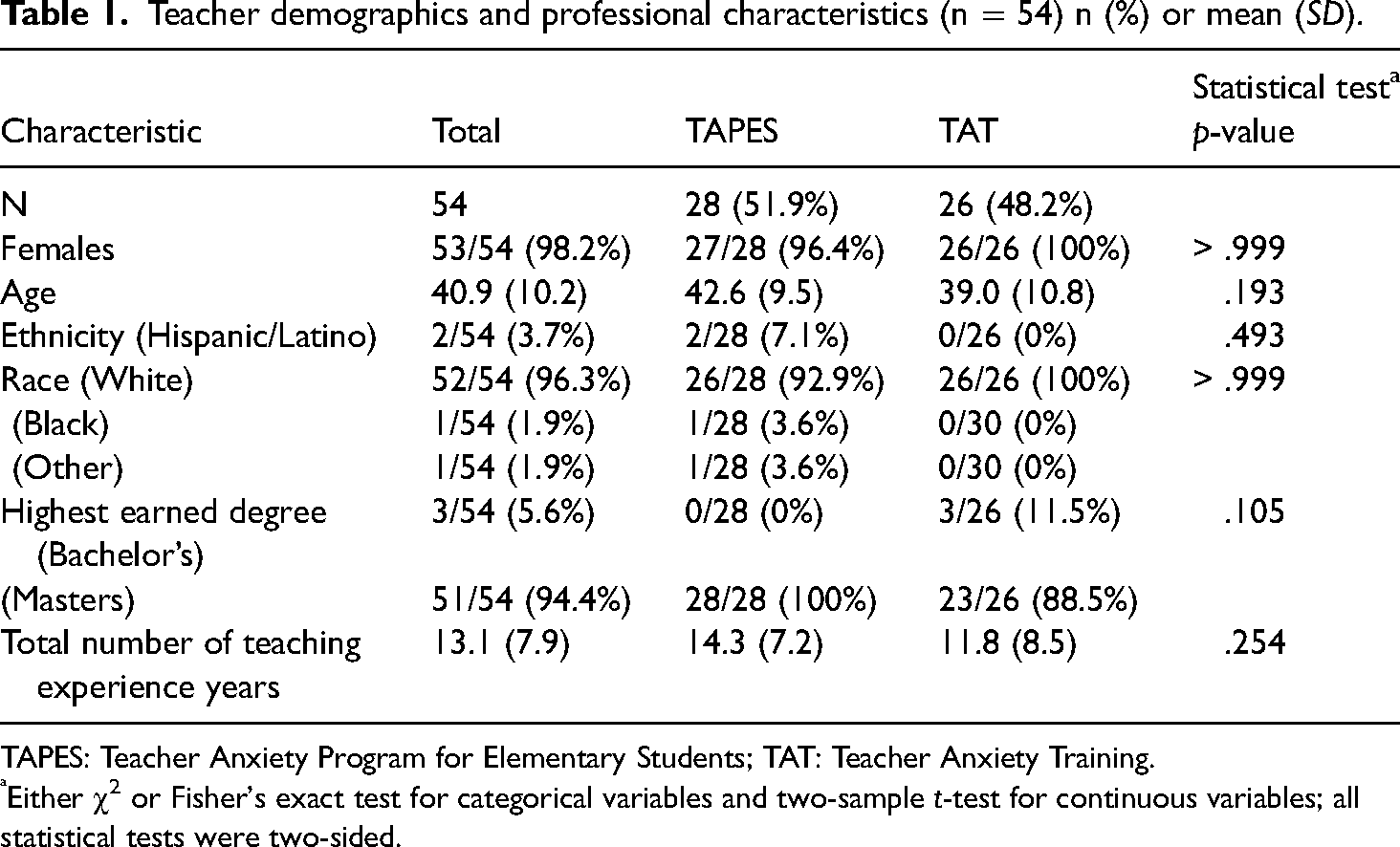
TAPES: Teacher Anxiety Program for Elementary Students; TAT: Teacher Anxiety Training.
Either χ2 or Fisher's exact test for categorical variables and two-sample t-test for continuous variables; all statistical tests were two-sided.
Description of trainings
The entirety of the TAT training and the first 3 h of the TAPES training presented teachers with identical didactic information. However, teachers in the TAPES training also received training in how to apply the information to individual students in the context of five conjoint parent–student–teacher meetings using role-playing and receiving direct feedback from trainers.
Procedures
This study was approved by the host university's Institutional Review Board and each school's principal. Teachers were recruited using a variety of strategies including flyers distributed to teachers directly, from school principals or school district administrators announcing the opportunity for teachers to participate in a research study that included free training on how to assist students with anxiety. All interested teachers were contacted to obtain informed consent. After teachers completed informed consent, they were randomized to TAPES or TAT (1:1 stratified by grade). Before beginning the training (baseline), teachers completed the baseline knowledge assessment and other measures listed below. Approximately 8–10 weeks after the training (post), teachers completed the same measures, as well as a measure assessing their satisfaction with the training. In addition, after training, teachers were asked to identify a student with anxiety with whom to apply their training skills and to complete a measure of anxiety accommodation (i.e. the Teacher Accommodation Scale of Anxiety or TASA; described below). Thirty-nine teachers identified at least one student and completed the TASA pre and post-enrollment of the student (i.e. 8–10 weeks later). Teachers were compensated with a $50 gift card for attending the training.
Measures
Teacher training satisfaction items (seven common items only) mean (SD).
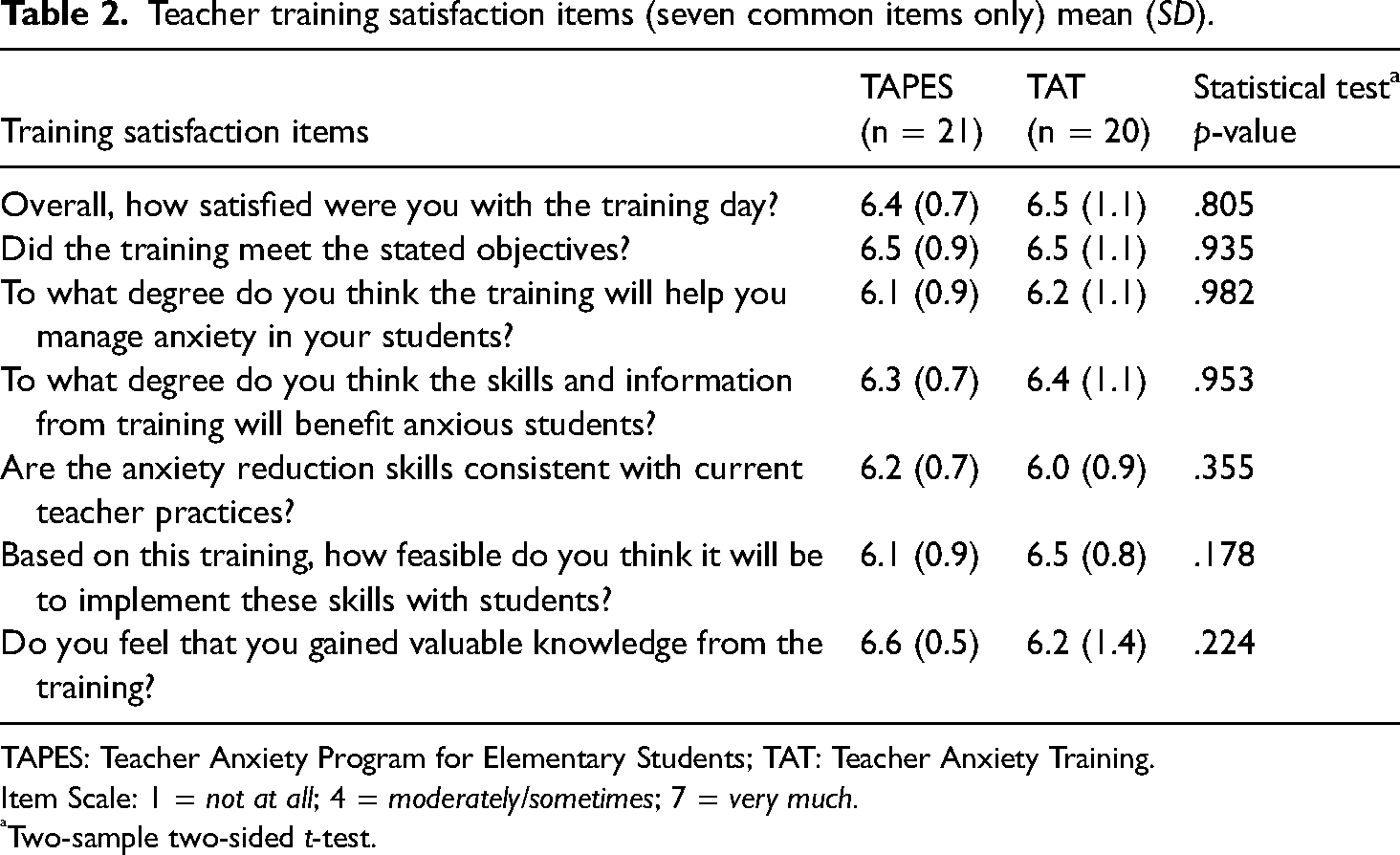
TAPES: Teacher Anxiety Program for Elementary Students; TAT: Teacher Anxiety Training.
Item Scale: 1 = not at all; 4 = moderately/sometimes; 7 = very much.
Two-sample two-sided t-test.
Data analyses
Attrition analyses were performed to determine whether trained teachers who did not complete one or more post-training/intervention measures differed from those who provided completed data on baseline teacher demographic characteristics and their randomized training group assignment using Fisher's Exact and Wilcoxon Rank Sum tests. Between-group differences at baseline on demographics and teacher characteristics were examined using a two-sample t-test and Wilcoxon Rank Sum test for continuous variables and χ2 or Fisher's exact test for categorical variables. Within-group pre–post changes and between groups comparisons on other measures were examined using mixed-design ANOVA that included a group-by-time interaction term. Specifically, a statistically significant interaction implied that pre–post changes differed by group. All statistical tests were two-sided at significance level of 5%. All parametric statistical tests’ assumptions had been checked and their results were compared with non-parametric tests whenever appropriate. Only results of statistical tests that met assumptions were reported. Moreover, when non-parametric tests agreed with parametric tests, only parametric tests were reported. Cohen's d effect sizes were calculated for both between- and within-group differences from test statistics and corresponding degrees of freedom using the effect size R package (Ben-Shachar et al., 2020, https://cran.r-project.org/web/packages/effectsize/index.html, https://easystats4u.shinyapps.io/statistic2effectsize/). In the traditional interpretation of Cohen's d, an effect size of 0.2 and above is considered small, 0.5 and above represents a medium effect, and 0.8 and above is considered a large effect (Cohen, 1988). However, clinically meaningful effects should be determined in relation to the scale of each instrument.
Results
Preliminary analyses and baseline group comparisons on teacher characteristics and student anxiety severity
There was no difference in the percentage of teachers randomized to TAPES (13/41 = 31%) and TAT (11/37 = 30%) who failed to complete training. There were also no differences between teachers who enrolled and did not enroll a student with respect to randomized training programs, teacher age, and years of teaching experience. There was no difference in enrolled student anxiety severity at baseline between those recruited by TAPES-trained teachers verses TAT trained teachers based on independent evaluators’ rating on the 7-point Clinical Global Impressions
Pre- and post-training and first student comparisons for teacher outcomes mean (SD) [n].
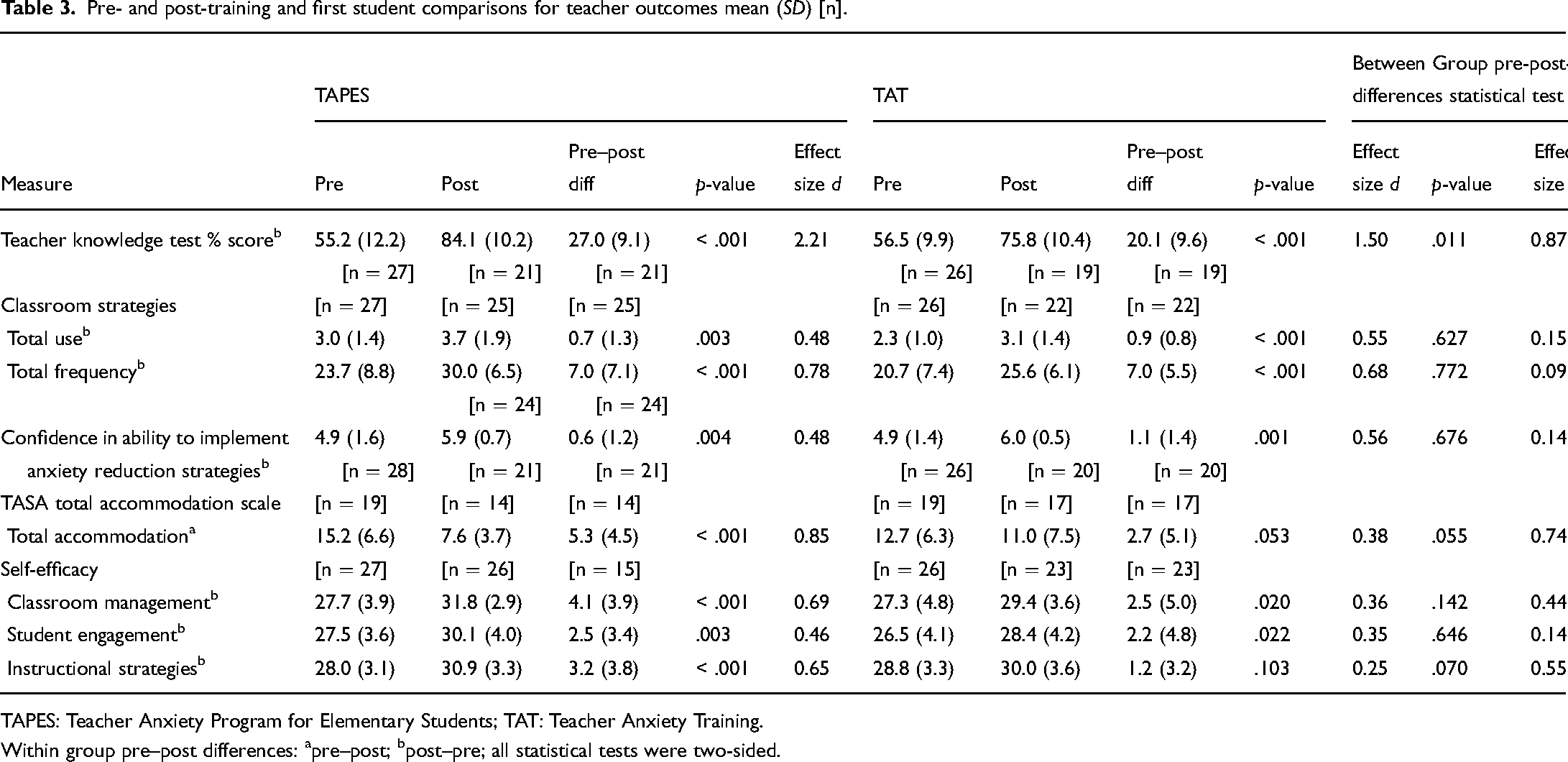
TAPES: Teacher Anxiety Program for Elementary Students; TAT: Teacher Anxiety Training.
Within group pre–post differences: apre–post; bpost–pre; all statistical tests were two-sided.
Discussion
The current study examined the impact of two elementary teacher trainings focused on identifying student anxiety and the use of anxiety reduction skills in the classroom. Overall, results indicated that teachers were highly satisfied with both trainings, and both trainings resulted in a broad range of improvements (e.g. in the knowledge of student anxiety and frequency in using anxiety reduction strategies in the classroom, teaching self-efficacy). Teachers who received the TAPES, compared to the TAT training, evidenced greater improvements in teacher knowledge.
In contrast to our hypothesis, however, there were no differences between the two trainings in levels of satisfaction, despite the fact that the TAPES training included active learning approaches such as modeling, and rehearsal/role plays which are associated with enhanced learning (Beidas & Kendall, 2010; Fixsen et al., 2005; Sholomskas et al., 2005). One interpretation of this finding is that both trainings offered new and important information to teachers and included access to materials to support implementation (e.g. handouts, resources), which may have increased the satisfaction of the teachers receiving TAT. The high level of satisfaction with the brief TAT training suggests that future trainings may be as effective using automated, virtual, and asynchronous options, which would allow access to the training to a broader population of teachers and be less costly. Specifically, while the current study was conducted in the United States, teachers in other countries, and particularly teachers working in low-resourced countries, may benefit from a similar brief training on student anxiety.
With respect to the use of anxiety reduction skills in the classroom, teachers in both trainings reported a significant increase in the frequency of using skills such as relaxation skills (e.g. deep breathing, progressive muscle relaxation, and a calm down corner), coping self-talk (e.g. encouraging students to use coping self-talk and modeling it for students), supporting students in facing (rather than avoiding) anxiety-provoking situations and increasing their autonomy/independence (rather than seeking reassurance), and promoting a collaborative and prosocial classroom environment (e.g. focusing on teamwork rather than competitive activities). Impressively, the effect sizes of changes in both knowledge and use of anxiety reduction strategies were medium to large (with most values greater than d = 0.5).
Pre-post training effects in teachers' use of accommodation of their student's anxiety also improved. Specifically, teachers in TAPES reported. Specifically, teachers reported that they were less likely to modify classroom activities to accommodate their student's anxiety, assist the student in avoiding things that might make them anxious, do things that are normally the students’ responsibility, or modify their work schedule (e.g. lunch, planning period) due to their student's anxiety. These types of activities by parents (i.e. accommodation of anxiety), have been associated with higher child anxiety and are often a key component of interventions to reduce anxiety (Thompson-Hollands et al., 2014). As noted, in a recent study, greater teacher accommodation of avoidance was associated with higher levels of students’ behavioral avoidance and anxiety severity (Ginsburg et al., 2023), highlighting the importance of addressing this teacher behavior in training.
These findings are consistent with the theoretical models of Han and Weiss (2005) and Guskey (2002) which detail the mechanisms of teacher behavior change in adopting mental health interventions. Specifically, the current findings suggest that the trainings improved a key teacher characteristic (i.e. self-efficacy and confidence) that has been linked to higher rates of implementation and sustained use of new skills (Stein & Wang, 1988; Tschannen-Moran & Hoy, 2001). That is, training can promote behavior change when it enhances teachers’ understanding of and beliefs that the new skills (a) will solve an important student problem, (b) are efficacious, and (c) are compatible with their teaching style and beliefs about children's behavior (Kealey et al., 2000).
Limitations and future directions
The results of this study should be interpreted in the context of several study limitations. The sample of teachers was comprised of volunteers, and they were relatively homogenous in terms of geographic region, race, ethnicity, gender, and school type (elementary schools only), thus restricting the generalizability of results. Additionally, the study utilized some measures that were modified or developed for the current study and have not been empirically validated (e.g. the internal consistency of the Classroom Strategies Questionnaire was .62, which may be a result of poor reliability or small sample size). The impact of the trainings was evaluated using teacher self-reports and may not reflect changes in actual behavior. Future studies using observational data on teachers’ use of classroom strategies are needed. In addition, the impact of the trainings was examined eight to ten weeks after the training, thus the longer-term impact of the trainings is unknown. Finally, future evaluation of these trainings on student anxiety and academic functioning is needed.
In summary, enhancing the capacity of teachers to identify and assist students with anxiety in their classroom via brief trainings shows promise. The improvements in teacher knowledge, skills, confidence, and perceived self-efficacy and reductions in self-reported accommodation of student anxiety suggest that teachers’ benefit even from brief trainings. School districts may benefit from exploring ways to increase access to and offerings of these types of trainings via online platforms for their teachers.
Footnotes
Compliance with ethical standards
This research was approved by the University of Connecticut School of Medicine's Institutional Review Board. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Institute of Education Sciences, U.S. Department of Education, through Grant # R324A170071 to the University of Connecticut School of Medicine. The opinions expressed are those of the authors and do not represent the views of the Institute or the U.S. Department of Education.
Informed consent
Informed consent was obtained from all participants.