
Abstract
Schools provide an ideal setting for early, accessible intervention according to research conducted in developed countries for adolescents experiencing adverse mental health (MH). Many schools in South Asia, however, lack structured and standardized school counselling services. Research indicates that where services do exist, students are reluctant to access them due to perceived high risks and low benefits in MH help seeking. This paper explores the challenges experienced in MH provision from the perspective of school counsellors. A qualitative approach was chosen, and three main themes emerged from the data using the thematic analysis: negative perceptions of MH and counselling, the unwillingness to invest in MH services, and the challenges inherent in the system itself. The findings reveal cultural implications behind these challenges and suggest grassroots level initiatives that can be implemented within schools to reduce the barriers to service provision without the need for legislative changes at a national level.
Keywords
Mental health (MH) issues across the globe have seen a sharp rise in prevalence and incidence, with a 13% increase in the decade leading up to 2017 (World Health Organization [WHO], 2019). Research indicates that adolescents are especially affected by MH issues, with over 16% of the population aged 10–19 years experiencing some form of adverse MH and suicide being the 2nd highest cause of death amongst those aged 15–19 years (WHO, 2019). Many studies point towards the recent rise in socio-emotional difficulties and other MH disorders in this age group (Collishaw, 2014), and the lifelong consequences of such issues (Underwood & Washington, 2017), asserting that systemic, accessible MH services for adolescents are of key concern today. This increasing need is further highlighted by systematic reviews on the impact of the COVID-19 pandemic on adolescent MH (Loades et al., 2020; Octavius et al., 2020).
The South Asian context
Existing research trends in South Asia (SA) attest to the global concerns on adolescent MH, although there is a dearth of evidence-based studies on the topic. In Sri Lanka (SL), a study screening for MH problems in urban school children indicated that over 45.5% of the sample displayed mild symptomatology (Perera, 2009a), while another national survey conducted in the same year revealed that 18.9% of the sample indicated emotional and behavioral issues and that 12.6% of them were severely affected by their difficulties (Perera, 2009b). In India, home to the highest number of adolescents in the world, Nebhinani and Jain (2019) indicate that a 2016 National MH Survey reported a 7.3% prevalence of psychological adversities among 13–17-year olds. Similarly, a scoping review conducted in Nepal indicated a 12.9%–17.03% prevalence of both emotional and behavioral difficulties in school samples (Chaulagain et al., 2019), while Pakistan reported that 17.2% and 21.4% of samples from school-based studies were exhibiting symptoms of depression and anxiety, respectively (Khalid et al., 2018). In Bhutan, 11.6% of a nationally representative sample reported MH issues such as suicide attempts (Dema et al., 2019).
National MH legislature can play an integral part in establishing and regulating systematic services by ensuring the provision of nonstigmatized primary care to all individuals, preventing human rights abuse by providing oversight, and compelling institutions to support individuals experiencing MH issues (Ayano, 2018). However, research in the SA region shows that MH services are still emerging fields as there is no updated and compelling legislature at the national level. SL, for instance, provides relief to those in need under the Lunacy Ordinance of 1873 and the MH policy of 2005–2015 that is currently under revision. The approach taken in these policies is very much a biomedical one that is focused on institutionalization and medication instead of a holistic, prevention orientation (Chandradasa & Kuruppuarachchi, 2017). Counselling itself is not regulated by any governing body. India, Nepal, Afghanistan, and Pakistan have redrafted their MH policies in the recent decade while Bangladesh, Maldives, Bhutan have not yet enacted specific laws regarding MH services (Weerasundera, 2012; WHO, 2006a,b).
This lack of state-mandated care necessitates the provision of MH services in existing community-based locations to which adolescents have regular access. Schools are recommended as ideal community-based institutions to provide care to children and adolescents (as they spend most of their waking time in schools; Fazel et al., 2014), and for carrying out early preventive and awareness measures in low-and-middle-income countries, which could reduce the burden of MH related disability on communities and states in the long run (WHO, 2014).
School counselling in SL
School counselling has been a service recognized for positively impacting study patterns of students, attendance, achievement, and learning behaviors (Rupani et al., 2012) and for leading to the general improvement of the well-being of students (Banerjee et al., 2013). A systematic review by Bains and Diallo (2015) also revealed that adolescents with MH issues were more likely to seek help in school-based health centers than at any other location and that school-based health services help eliminate many barriers to seeking help.
The majority of psychosocial support available in SL is focused on reconciliation, disaster response, and transitional justice efforts that fluctuate with governmental regimes and funding (The Asia Foundation, 2016) and only sporadic efforts to provide MH services within schools have been documented. Furthermore, a distinct reluctance to access services can be witnessed where MH services do exist. The few studies done in the island imply that students are not utilizing these services to their fullest capacity even though around 1,086 schools out of 9,905 (as of 2012) had school counsellors on site (Pathirana, 2016). One study highlighted that 52% of the students surveyed were not satisfied with counselling services offered by their school, and many students were afraid to even speak to the counsellor (Chathurika, 2015). A mixed-methods study done by Pathirana (2017) corroborates these findings. The researchers cited issues such as breaches in confidentiality, lack of a private counselling space, the tendency of the counsellors to give advice or berate the student, and stigmatization as some of the reasons for the reluctance to access services.
Due to the lack of national guidelines and school counsellors not being highlighted as important MH service providers, subject teachers who complete a Postgraduate Diploma in Education or individuals who have completed some studies related to psychology, philosophy, or theology are often recruited as counsellors (Pathirana, 2016). A similar plight can be witnessed in other countries in the region; literature indicates that in India, there are no national frameworks for the selection and recruitment of school counsellors (Bagrodia & Bhatia, 2017). In Bhutan, school counselling was introduced only recently, and studies expose inadequate training and high expectations placed on counsellors (Dem & Busch, 2018). Nepal tested and compiled a manual for guidance and counselling using a teacher-counsellor model for the first time only a few years ago (Kandel, 2020).
The authors of this paper contend that existing evidence on school counselling within SL could be understood through certain predictive factors indicated in the Health Belief Model (Rosenstock, 1974). The “social costs” of accessing service were high, as indicated in the studies by Pathirana (2017) and Chathurika (2015) and there was a perceived lack of benefits in seeking out MH care within school settings. The Previous studies also implied that MH issues were not considered a priority or perceived as matters that could have possibly severe repercussions. As the aversion to accessing school counselling seemed to be mainly attributed to the perceptions of high risks and low benefits in previous studies, specifically connected to the role the school counsellors seemed to play in this process, this study sought to examine these perceived barriers through the perspective of the counsellors themselves. A lack of evidence-based studies on counselling in SL and the SA region prompted the use of a qualitative design to obtain a depth of information. Furthermore, this study aimed to provide recommendations on the improvement of the system based on the experiences of counsellors.
Method
Design
As the study aimed to delve deeper into the barriers to service access uncovered by previous quantitative studies on the topic, and qualitative methods could offer a “rich and thick” narrative compared to quantitative methods (Smith, 2015, p. 1), a qualitative approach was deemed most suitable. Although the lack of primary data and validated quantitative measures were also reasons to employ a qualitative method, it must also be noted that not enough schools in SL have an onsite counsellor to conduct a comprehensive quantitative study. According to Palinkas (2014), qualitative research can be ideal in evoking and delineating the perspectives of the participants and in parsing issues that are underexplored. Therefore, as a study investigating the school counsellor's perspective for the first time, this approach was thought to be essential in gathering a broader scope of information that future studies could build upon rather than condensing their experiences into numerical values.
Participants
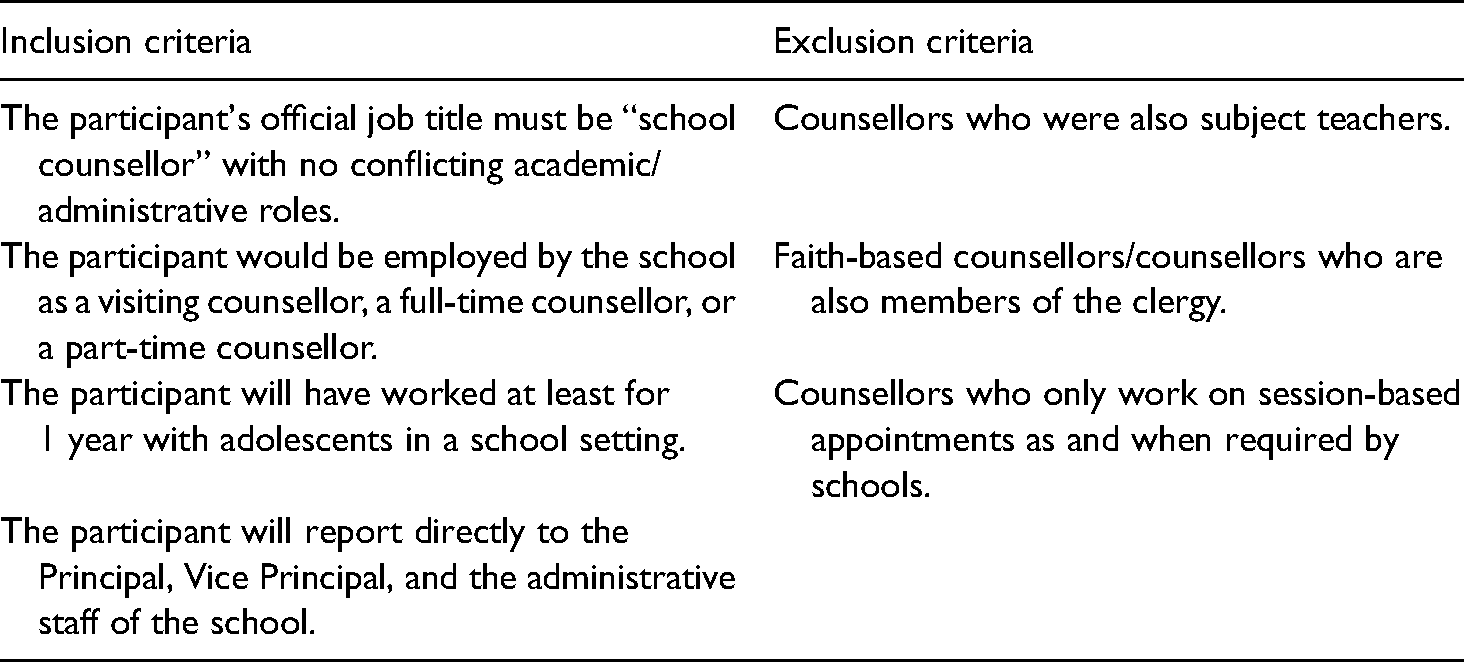
The study aimed to recruit six school counsellors after receiving ethics approval (from the Research Ethics Panel of the University of West London) and approval from relevant participant school authorities. Specific inclusion and exclusion criteria (listed in Table 1) were adhered to in the recruitment process.
Participant requirements for inclusion in the study.
A convenience sampling process was employed, and from over 400 schools in the district around 10 schools that had counsellors that fit the inclusion criteria were shortlisted. Principals of the schools were approached first and when they granted permission, the school counsellor was contacted next to determine willingness to participate in the study. The anonymity of the counsellors was guaranteed by withholding information on the type of school setting (public/private/international) they worked in and by removing any references to cues that could lead to the identification of the school. Eventually, four participants were interviewed as many schools were unwilling to participate in a study of this nature.
The researchers decided to exclude counsellors who also acted as subject teachers or religious figures within the school from the current study. They are often tasked with other responsibilities such as overseeing extracurricular activities, sports teams, disciplinary matters and have a full schedule from 7:00 am till well beyond school hours. They do not have dedicated time set aside for their role as counsellors, have less exposure to students in a counselling setting, and are sometimes not strictly required to have formal training in counselling practices. The dual role conundrum of the subject teacher-counsellor is often the result of a lack of resource personnel available for this role and should be explored separately. The researchers chose to focus on the experiences of only those who have dedicated their training and professional efforts for counselling with no conflicting interests (Table 2).
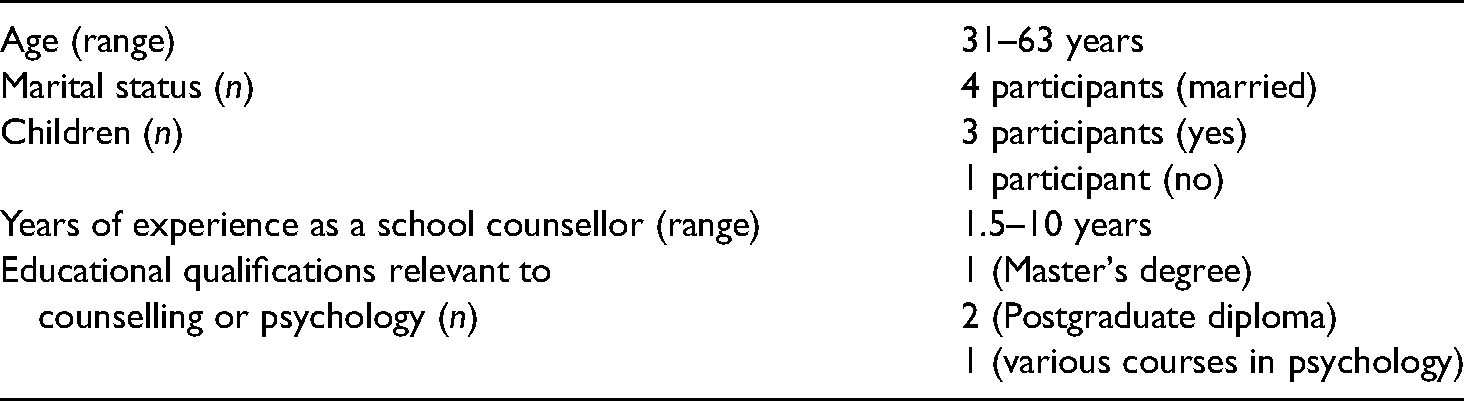
Summary of demographic data of participants.
Materials
The interview schedule started with questions requiring the participants to provide basic demographic information, followed by a semi-structured interview that allowed the counsellors to discuss their role, their scope of work, the school setting, and the role of school administration in their daily duties. The counsellors were also queried about the general needs presented by students and barriers to working to their fullest capacity as well as what factors they thought facilitated service provision.
Procedure
The interviews were conducted in a neutral setting away from the school such as a café chosen by the counsellor. The participants provided both written and verbal consent to participate in the study, after receiving written consent from their respective schools. The participants did not receive any incentives or any other reward for participation and it was voluntary. Transcribing of data was completed by the researcher to ensure confidentiality.
Analysis
The method of analysis that was used in this study was Thematic Analysis (TA), specifically within a critical realist/contextual framework, where it is acknowledged that while there exists a reality, the access to it would be shaped by contextual factors and generated through the interpretations of the researchers (Smith, 2015). Through this framework, the researchers of this study sought to construe how counsellors understood the challenges surrounding their work and their role. As the first qualitative study being conducted on the topic, it was considered necessary to allow the data to speak for itself and to provide a space for the counsellors to give voice to their interpretations of their reality. The Braun and Clarke (2006) guidelines for TA were followed as according to Nowell et al. (2017), TA allows the researchers to compare and contrast the different perspectives of the participants while also allowing the researcher to uncover unforeseen and insightful inferences.
The initial codes that emerged were presented to one of the participating school counsellors of the sample to provide feedback, thereby engaging in a process of “respondent validation” to enhance the trustworthiness of the study. The available literature on MH service issues within the country was referred to during analysis to further understand the socio-cultural setting and the participant's perspectives. The researcher also reflected on her own previous experiences of working with adolescents in a school setting as well as her current work related to national MH structures and policies, to gain insight into the data that has been collected. Accordingly, the codes were revised, and the themes were finalized.
Results
The analysis of the interviews revealed an expansive scope of information regarding the work and the experiences of school counsellors in SL. The discussions with the counsellors on their role and scope revealed that they often did not have a set agenda and that each counsellor was recruited on different selection criteria (although they mentioned that being over the age of 30 and being married and/or having children seemed to be a prerequisite). They also had varying degrees of authority within the school (with some having to report directly to the principal and others having to navigate complex hierarchies of class teachers and sectional heads) and were not required to engage in continuing professional development or any counselling-related training.
The initial thematic map of codes that emerged delving into service provision from the counsellors’ perspective can be found in the attached Supplemental Material. Of the many themes that emerged during analysis of data regarding barriers to service provision, the following are highlighted in this paper: negative perceptions of MH and counselling, perceived unwillingness to invest in MH services, and the challenges inherent in the setting (see thematic map in Figure 1).
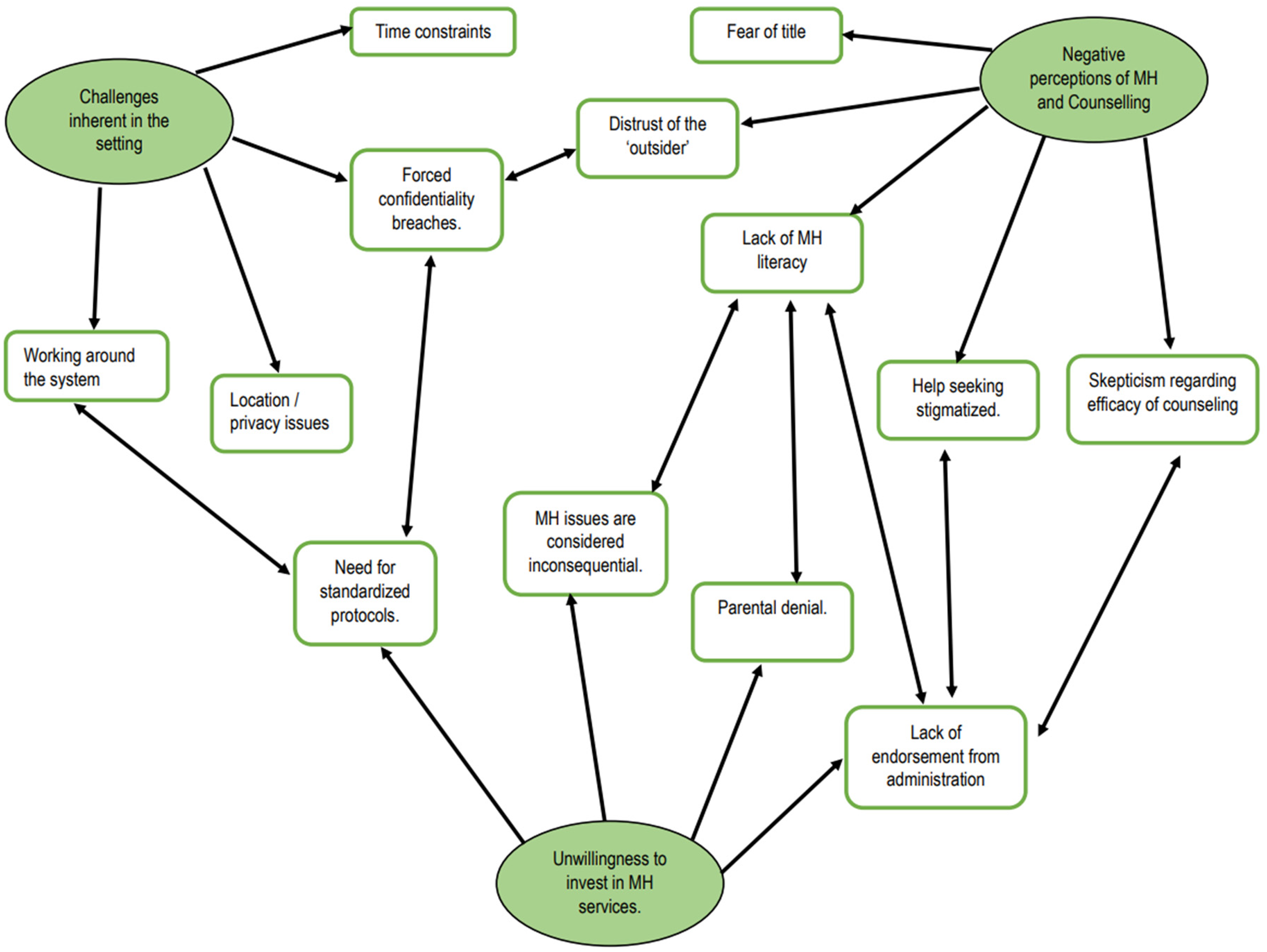
Barriers to MH service provision experienced by counsellors in SL.
Negative perceptions of MH and counselling
MH literary is an important factor that could influence an individual's help-seeking behaviors, as well as their reactions to others seeking help. As defined by Choudhry et al. (2016), it is attitudes towards, and beliefs, and knowledge a layperson has about MH issues and remedies. These are shaped by personal knowledge, interactions with an individual with mental illness as well as cultural stereotypes, and various other factors. The sample of counsellors in the study spoke of an alarming lack of awareness in all related parties on issues concerning MH. Many participants reported encountering situations where they realized that few around them understood what counselling was, and whether the service was even available within the school (“At least 50% wouldn’t know what counselling is. They didn’t even know that a person called a counsellor existed”). Those who did know the existence of the service and would seek help did not seem to understand that counselling was an on-going process and instead considered it to be a one-off chat that would offer an immediate solution to their difficulties (“Follow up sessions are very difficult to take. It is not like you drink medicine and you take it till you finish the course. It all depends—if they go back home and feel like they are fine, they won’t come back the next week”).
Due to this lack of understanding regarding the gravity of MH issues and of counselling services, the counsellors often experienced situations where they were alienated within the school system simply because of their title. All four of the counsellors in the sample spoke of their position itself as something that hindered them from providing this service to the students (“I think the title itself made my life difficult. The minute it says counsellor, here people look at you like… I don’t know….”) and that they were often faced with scepticism regarding the utility and the effectiveness of their services. Counselling is a complex relationship built on the therapeutic alliance of the parties involved, the skills of the counsellors and the self-efficacy of the client, and not simply “talking about problems.” However, it seemed that teachers would often assume this to be the case and express to children that visiting the counsellor was unnecessary, thereby delegitimizing the role of the counsellor. Overall, there was a distinct sense that MH issues were inconsequential and easily remedied by a “chat” that did not require any specific skill set, as revealed by one participant. And some of the teachers used to feel kind of intimidated when they see the child coming into the counselling room. They call the student and ask, ‘why did you go there, why won’t you tell me the problem, I can help you’ and so on.
Unwillingness to invest in MH services
Apropos the generally negative perceptions of counselling and lack of MH literacy that the counsellors felt were key barriers to service provision, another key theme that was recurrent in what they disclosed was a distinct unwillingness from the stakeholders to invest (time or resources) in any MH services. A school will generally invest in many resources such as its infrastructure, curricula, teachers, and students in various ways. All these investments are made in hopes of providing a fully rounded education to the students and of equipping the student with necessary life skills. The interviews with the counsellors revealed that, while schools did invest in many of these resources and considered them worthwhile investments, the need to invest in MH services was not acknowledged at all.
Firstly, the counsellors spoke of challenges in being acknowledged as a legitimate service within the school and of convincing the administration of the gravity of certain difficulties the students were experiencing. The onsite administrators of the school were often the principal, vice-principal, sectional heads, and in some schools a religious figure such as a priest who was attached to the school. All of them held considerable authority and had the final say over what could and could not be done for a student in distress. They could either compel involved parties to offer the child the necessary support or dismiss the matter entirely. The participants implied that the counselling unit was often merely established as a token gesture of addressing student needs and that the counsellor frequently had to work with no support from other stakeholders within the school (“most of the school in which I have worked though they have the unit… it has actually been my responsibility to develop the unit”).
It was found that oftentimes educational matters and extracurricular activities took prominence in any discussion and MH-related issues were only discussed in relation to how they might affect a student's performance. One participant mentioned, “I found that the administration didn’t realise the gravity of the situation… it was like ‘oh when we were in school, we were bullied, it isn’t a big deal’. That's the kind of attitude they had.” Teachers had both implicit and explicit duties to fulfil in the school setting and various goals to achieve. In contrast, the counsellors were not set any such requirements—they were often not incentivized to engage in skill development, given a clear job description, or assigned specific tasks.
In addition to the school administration, the counsellors frequently faced resistance from the parents as well. The inability of adolescents and minors to access and pay for healthcare by themselves is one of the key reasons for the existence of school counselling in the first place. Even with the service in place, parents are still a necessary part of the equation, as not all MH needs of an adolescent can be met by the school counsellor (such as prescribing medication or diagnosis of emotional, behavioral, or learning difficulties), and the cooperation of the parent is needed for some issues the student might be facing (such as severe sibling rivalry or instances of abuse). However, the lack of MH literacy highlighted and the lack of endorsement from the administration on the importance of addressing MH issues also manifested itself in the lack of support from parents (“Parents are sometimes in denial… and by the time they address the issue, it's too late.”).
Parental denial, consequently, had a limiting effect on what the counsellor could do for a child. Many of the counsellors experienced instances of parents refusing to meet them, refusing to take the child for much needed external help such as psychiatrists, and even of parents forbidding the child from meeting the counsellor (“I have had one incident with a parent where they have asked the school to never let their children talk to the counsellor”). A distinct pattern of comments that each counsellor provided also revealed that most of the issues the students were tackling originated from, and due to, their families (“….. because the issues these kids face are… 75% due to the home environment,”). Although the counsellors did not directly mention it, it was implied that parents were unwilling to address certain issues with an outsider (the counsellor) because private family matters might have to be disclosed.
When met with these challenges, each counsellor seemed to have taken a different approach in resolving the matter. One of the counsellors simply chose to allow the school and the students to become familiar with her over a period of years. Another attempted to conduct discussions and training sessions with the teachers to combat the lack of awareness within the school system and was often met with many restrictions, long waiting periods, and postponements, by as much as a full school year in some cases. … for the teachers even if we organise an awareness session it has to be after school or on a Saturday. But at the same time, there are very few teachers who realise why it is important. Sometimes they will just come sit there and grumble and go home. It doesn’t really work. So, they will turn up for it if it is something for their subject, without understanding that this part is important as well. I think I got lucky because I was a part of the staff. I know most of the things about how the school runs for instance, so I feel very much at home there. There was a plus there since I was not a total outsider coming into school to do this.
Additionally, in response to further probes on this sense of helplessness they seemed to convey, the counsellors unanimously voiced the need for structured services. The lack of standardized protocols offered by governing bodies such as the Ministry of Education and the flexibility given to schools to recruit and utilize counsellors in an ad hoc manner had heightened the confusion surrounding an already unfamiliar topic. If there is a methodical way of school counselling happening then that would be helpful, if the management can educate the staff officially—formally—then that would be better.
Challenges inherent in the setting
One of the most ubiquitous justifications the counsellors presented for their challenges when describing their daily routines were the barriers that were inherent in and generated by the school system itself. None of the counsellors, for instance, had a dedicated counselling space when they first joined their respective schools and had to make do with a repurposed spare room (“actually when I went in [laughs] there was a huge double bed in that room and a dressing table and a cupboard….”) or a corner of the staff room until they could make arrangements for a private space on their own. Whereas a teacher would have his or her own timetable and specific tasks, and there is an established relationship between the service providers (teachers) and service recipients (students), the school counsellors in SL seem to struggle with a different reality altogether. They spoke frequently of how their frustrations were compounded by the way the school schedules impact service provision but also of how they had to eventually learn to work around the system instead of within it.
Schools are institutions where children are accounted for at all times. Each class teacher and each subject teacher is often conscious of students who are not in school, and all students follow a strict timetable. In such a situation, it is extremely difficult for it to go unnoticed if one student needs to take time off a certain class to visit the counsellor. Considering the conspicuous nature of this, it is even more important for a visit to the counsellor to be “normal,” lest students are uncomfortable seeking help. The students and the teachers, however, had full schedules that did not allow them much flexibility either, and therefore, the counsellors struggled to make time for students who did seek help, often arriving early at school or staying well beyond school hours to wait for students. It’s very difficult to do a normal counselling session in school as the time is very limited. Even the interval is about 20–30 minutes and when one student is inside there will be another one standing outside so I can’t ask them to turn back. So sometimes I have to limit their time to 10 minutes or sometimes even 5 minutes. Whenever the children were to be punished for some issue in school, they would send the kid to detention. To me! I always used to tell the kids, I am here to help you, not to punish you. And I just talk to them about what happened. Now that I thought was not correct on the part of the administration.
Overall, the lack of MH literacy, prominence placed on educational matters over psychological well-being, lack of structured services leading to ad hoc service provision, breaches in confidentiality, distrust of the “outsider,” forced dual roles and the counsellors having to work around the system and stakeholder unwillingness to invest in MH services were key highlights of the counsellor's experiences of working within the school setting. However, despite the many barriers that prevented the school counsellors from helping students, all the school counsellors found the service to be a positive and essential thing. Many spoke about the sheer importance of availability; the fact that students did not have to pay for the service or require parental assistance or permission to access the service or even wait too long if they were having some difficulties was considered by them to be highly valuable. They were optimistic about the fact that their respective student bodies had a service available to them that the school counsellors themselves did not have access to when they were schooling. Yet, in the words of one participant, “overall, school counselling is helpful, but we can do better.”
Discussion
This study aimed to explore the perspective of the counsellors on perceived risks and benefits of seeking MH care adolescents have reported to experience within a school setting using qualitative methods. The results indicate that the counsellors often experienced a mirror reflection of the difficulties faced by students such as access to care, breaches of confidentiality and stigma.
On the whole, the results of the study are comparable to others done on barriers to MH help-seeking and service provision in other regions echoing concerns of lack of national policy, stigma, and negative beliefs towards MH professionals and MH services (Aguirre Velasco et al., 2020; Patalay et al., 2016). What was found to be unique was that all the counsellors in the sample made sense of the challenges they experienced by using explanations tied to culture and community beliefs. It is important to acknowledge that there exist wider economic, political, and other reasons for difficulties in establishing systematic MH care within schools. However, the counsellors’ reasoning points to deeply rooted cultural values found to be common to many countries in the region, such as collectivistic and feminine dimensions of the culture, “self-face” concerns (one's social image and worth based on evaluations of others; Ting-Toomey & Kurogi, 1998), distrust of outsiders, and reservations regarding “out-groups.”
A person's cultural context is known to influence help-seeking behaviors, treatment methods, and even the prognosis, both directly and indirectly. Many studies report cultural factors to be a barrier to help-seeking behaviors (Rostain et al., 2015), which are ultimately related to the extent to which a service provider will be able to function to the fullest of their capabilities. Studies conducted in SL divulge that stigma surrounding the topic of MH often prevents service providers from accessing those in need (Samarasekara et al., 2012) and that MH professionals themselves were stigmatized and alienated by their communities, corroborating the fear of the “title” and the active discouragement of help seeking the counsellors in this study spoke about (Liyanage et al., 2018).
The theme of stakeholder unwillingness to invest in MH services is further elucidated by literature that indicates cultural barriers that seemed to influence help seeking. For example, a study conducted by Fernando et al. (2016) in SL revealed that stigma had a greater delaying effect on the help-seeking behaviors of caregivers than on the patients themselves. Stigma associated with mental illness is prevalent across the region, with multiple studies in India (Anusha et al., 2017), Nepal (Adhikari et al., 2009), Bangladesh (Giasuddin et al., 2014), and Pakistan (Khalil et al., 2020) demonstrating this. An underlying cause for this can be understood if the issue is investigated through the perspectives of the Hofstede dimensions of culture (Hofstede, 2001), where SL is ranked as a collectivistic and feminine culture (Hofstede Insights – Country Comparison, n.d.). In effect, the low individualism score reveals that natives give higher prominence to cohesive, harmonious living, and the low masculinity score indicates that standing out from the crowd would not be considered admirable or favorable under any circumstance. Collectivistic cultures produce individuals with an interdependent sense of self, where identities are tied strongly with those in the in-group. In such a context, making important choices (such as seeking support) would not only be difficult, and not considered merely a personal, individual choice (as studies with Indian participants also corroborate [Savani et al., 2010]), but could also be perceived as liable to disrupting close relationships (Kim et al., 2006).
Moreover, feminine cultures, generally, have a low focus on personal well-being. Violating these basic principles by placing one's own needs (e.g., the need to see a psychiatrist) over the group's needs (e.g., the parents’ need to avoid embarrassment in front of family and friends) would result in harsh repercussions such as social isolation, ridicule, and shame (Heine, 2019). This could be especially difficult in a culture where saving “face” is of paramount importance. A startling study conducted in SL by Abeyasekera and Marecek (2020) illustrated that not even the act of suicide or near-fatal self-harm in SL was considered to be a personal act. The paper further illustrates a resolute denial in addressing emotional distress and the assumption that a person must simply “behave well” and “get over it” soon, as there are responsibilities that demand attention, further illustrating the subthemes of parental denial and the belief that MH issues were inconsequential.
Research carried out using individualistic and collectivistic participants further indicates that collectivistic cultures value in-group members significantly more than out-group members (Gomez et al., 2017). In collectivistic cultures, the relationships one has with one's in-group can be self-defining. There are strong, nonpermeable boundaries placed between the in-group and the out-group, and a lower level of trust is extended towards strangers (Van Hoorn, 2014). Both the students’ reluctance to divulge personal issues to the school counsellor and the parents’ disapproval of their children seeking help from the counsellor becomes obvious consequences of such a context. This unwillingness to open up to the school counsellor from an out-group was extensively illustrated by the counsellor who mentioned, very astutely, that she felt she had an easier time carrying out her duties in the school because she was well known to students and faculty in the school. Teacher-counsellors who are more familiar with the students might seem like the solution to this conundrum, but they pose other issues such as lack of training and being asked to prioritize subject matters.
All these insights point to the fact that cultural beliefs are strongly tied to the challenges of service provision in schools. Even though national level policy changes would require an attitudinal change towards MH as a whole, several key recommendations can be made to improve MH service provision through school counselling that does not require large-scale systemic changes. Instigating change within schools themselves is important especially considering that the current national MH policy in SL under revision does not indicate any guidelines or budgetary allocations to develop school counselling at a state level. As the results revealed that endorsement from stakeholders is important, the school administration would have to promote existing counselling services within the school by way of general announcements, posters on MH topics, and including it as a discussion point during parent-teacher meetings. Such open discussions should serve as a starting point to demystify the counselling process and make it appear less taboo and secretive. To increase parental trust in the service, the schools would also have to put into place a confidentiality policy and incentivize school counsellors to engage in continued professional development to cultivate new skills and to legitimize their expertise. Additionally, it would also be important to tackle the issue of counsellors being “outsiders” by giving counsellors increased opportunities to meet the students and teachers regularly in a noncounselling setting, such as workshops, school activities, and career guidance. In the long term, school counsellors might also need to lobby for standardized protocols and policy level acknowledgement and changes that compel the institutions they are attached to provide more systematic care.
Strengths and limitations
This study was the first known qualitative study to be done in the island on school counselling, and the literature of studies done previously in the island and within the SA region suggests that the findings would be transferable to similar contexts. A few key limitations of the study would be that the data were collected from a limited number of female participants and the study conducted prior to the closure of schools due to COVID-19. However, it must be emphasized that the study was conducted as an exploratory research that would provide insights that future studies could build upon.
Future studies
Future studies would need to include male school counsellors in a larger sample size that could also include quantitative elements in data collection and analysis. A study that includes stakeholders within the school setting, parents and teacher-counsellors would be imperative in further understanding how service provision could be improved. Qualitative studies examining barriers to service provision, especially in relation to cultural and administrative barriers, are required in other SA countries as well, which could help elucidate short-term, practical solutions that can be implemented to improve MH service provision within schools.
Conclusion
This study brought to light the importance of exploring the service provider's perspective of barriers to MH help seeking, not only to understand what would promote better service provision but also to understand how they make meaning of their experiences. Especially as MH is not a widely spoken of a topic in many cultures, attempting to make changes at the grassroots level could act as a catalyst for wider societal change.
It is anticipated that the findings of this study will draw attention to the experiences of school counsellors that will instigate further research into documenting the limitations and the core strengths of existing resources as well as facilitate successful evidence-based initiatives to upskill school counsellors and standardize the profession.
Supplemental Material
sj-docx-1-spi-10.1177_01430343211043062 - Supplemental material for Exploring challenges in mental health service provisions for school-going adolescents in Sri Lanka
Supplemental material, sj-docx-1-spi-10.1177_01430343211043062 for Exploring challenges in mental health service provisions for school-going adolescents in Sri Lanka by H. Kaushi H. Jayawardena and Gayani P. Gamage in School Psychology International
Footnotes
Authors’ note
This study was conducted while the corresponding author was reading for her master's degree in a Sri Lankan university affiliated with the University of West London's Master of Health and Clinical Psychology program. The Research Ethics Committee of the University of West London provided approval for this study. The study was accepted and displayed in the poster presentation segment of the British Psychological Society's Division of Health Psychology Annual Conference in 2019 of the study was published in the British Psychological Society's Division of Health Psychology Annual Conference in 2019.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.