
Abstract

The first case of severe acute respiratory syndrome coronavirus 2 was reported in Wuhan, China, in December 2019; the first case in the UK was reported in January 2020. By March 2020, reports were emerging that some coronavirus disease 2019 (COVID-19) survivors were left with persisting health problems rather than making a complete recovery. These people are commonly referred to as having Long COVID or post-COVID-19 condition. The UK government has invested over £50 million in Long COVID research 1 and over 200 symptoms associated with Long COVID, in adults and in children and young people (CYP), have been identified.2,3 Yet, there is stark heterogeneity in the literature regarding the implementation of, and approach to, treating Long COVID. The purpose of this commentary is to reflect on what we know and what we need to know about Long COVID and to provide a springboard for suggestions on how to be better prepared for future pandemics.
What we know
Findings from UK government investments and the broader literature have yielded three points of note. First, the presentation of Long COVID demonstrates broad similarity across different age ranges, showing comparable reported symptoms in both CYP and adults (Table 1). Additionally, predictors of Long COVID (e.g. female sex and co-morbidities) are similar in both CYP and adults. Notably, while prevalence estimates vary greatly, 4 NHS England data suggest that Long COVID increases healthcare utilisation and costs. 5
Pooled prevalence estimates (%) of symptoms in children and young people (CYP) and adults after COVID-19 infection. a
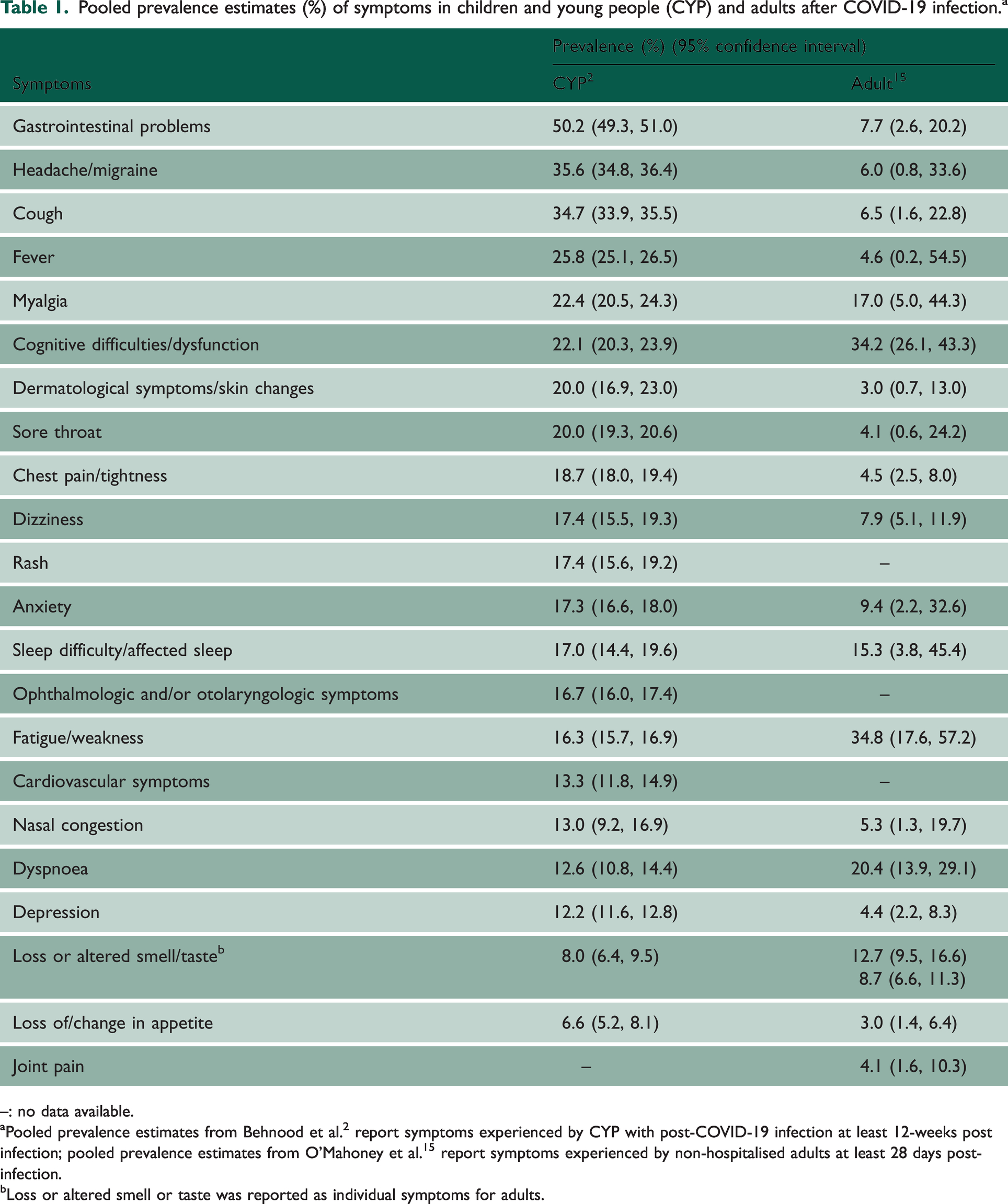
–: no data available.
Pooled prevalence estimates from Behnood et al. 2 report symptoms experienced by CYP with post-COVID-19 infection at least 12-weeks post infection; pooled prevalence estimates from O’Mahoney et al. 15 report symptoms experienced by non-hospitalised adults at least 28 days post-infection.
Loss or altered smell or taste was reported as individual symptoms for adults.
Second, the value and purpose of a Long COVID definition warrants consideration. Nationally funded researchers were the first to produce a Delphi research definition for Long COVID in CYP, 6 allowing for consistent application across scientific studies. This was closely followed by the World Health Organization clinical case definition, 7 which broadly aligned with the Delphi definition and the definition in adults, 8 allowing for a comparison of Long COVID across the age range. However, the formulation and implementation of a Long COVID definition could vary depending on its purpose: for example, for diagnosis or treatment or research. Identifying Long COVID from GP records remains challenging, given that coding of symptoms and diagnoses is incomplete and researcher access to narrative clinical notes is limited. 9 Furthermore, while critics argue that Long COVID definitions are imprecise, we acknowledge that definitions are not immutable and can change over time.
Third, methodological challenges when researching Long COVID are ranging from selection of an appropriate comparison group, complexities in accounting for time-related changes in the virus, immune landscape and mass-testing policies, to potential biases in analytical samples compared with target populations. Given these challenges and observed heterogeneity in implementing definitions of Long COVID in different datasets, it is unsurprising that the literature provides diverging estimates of Long COVID prevalence. 4 A firm epidemiological grounding is invaluable to conducting well-designed studies, and a comprehensive understanding of the ability, and limitations, of statistical methods to address biases is essential in any future work.
What we don’t know
With over 200 symptoms being attributed to Long COVID,2,3 it is clear that there is a dearth of pre-pandemic normative data on these symptoms, including long-term symptomology following other common respiratory infections, across all ages in the general population. This information is necessary to provide baseline comparisons. Thus, it highlights the importance of continuing large-scale data collections such as from the UK Birth Cohorts and longitudinal community household cohorts of seasonal respiratory infections, to ensure that normative data collection is maintained as a baseline before the next pandemic. In addition, the value of routine data sources (e.g. weekly surveillance data from the Royal College of General Practitioners, and electronic health record research databases, such as the Clinical Practice Research Datalink) is acknowledged. Large-scale epidemiological studies complement routine data sources (and vice versa) with each data resource subject to their own strengths and limitations.
Long COVID is a nascent condition, and longer-term follow-up is required to understand its enduring implications. For example, could there be covert effects on future cardiovascular and/or neurological development, and would these vary depending on the life-stage when Long COVID was experienced? What factors influence the trajectory, persistence of, and reduction in Long COVID symptoms? Questions also remain around designing and implementing interventions as it is yet unclear what works for whom, why and under what circumstances. For example, how should interventions be designed to be usable, targeting the range of associated symptoms without being overwhelming while simultaneously ensuring effectiveness? And how can we best exploit the potential of technology-based interventions alongside pharmaceutical and other therapeutic interventions? Importantly, when designing and implementing interventions, we need to consider their effectiveness across different sub-populations (e.g. by age, sex, ethnicity and socioeconomic position).
Finally, the current literature appears to divide health into artificially distinct physical and mental domains. This is a false dichotomy: these domains of health overlap, affecting one another. Relatedly, health does not exist in a vacuum and effects of Long COVID can extend to other aspects of life, including social, educational, employment and financial domains. Thus, Long COVID interventions should be created within an interdisciplinary setting.
Reflections
The probability of experiencing a pandemic with similar impacts to COVID-19 is estimated to be about 38% in one’s lifetime, with the potential of this doubling in coming decades.
10
Such stark projections highlight the need to adjust our perceptions of pandemic risks and expectations for preparedness. Experiences during COVID-19 demonstrate an understandably heavy investment in immediate response and research, for example on vaccinations. However, there has been comparatively less commitment to medium- and longer-term recovery, both in terms of support for Long COVID and more broadly. For example, the UK Department for Education has been criticised for not taking more effective action on education recovery
11
despite evidence that severe Long COVID is associated with worse academic performance.
12
Challenges remain and are important to address if we want to be better prepared for and recover from the next pandemic. Considerations for future pandemic preparedness include (but are not limited to):
Data issues: the need for both continued collection from large population-based samples and appropriate and swift access to routinely collected data from hospitals, GP visits, specialist care, etc. Control of patient information regulations may need to be adjusted to continue ensuring confidentiality while reducing administrative burdens for research. Where possible, standardised measures/clinical codes should be used consistently across data sources; Engagement with patient advocacy groups: guidance is needed with respect to how best to incorporate patient voices into research in circumstances where those patients are managing a highly debilitating long-term condition; expectations of researchers, advocates and Patient Public Involvement and Engagement (PPIE) members need to be appropriately managed; and resulting impact needs to be evaluated; Health inequalities: after infection, recovery and access to support in the immediate and long term and associated inequalities in wellbeing are pervasive issues that need attention. These inequalities do not occur randomly, are avoidable and are against the principles of social justice.
Notwithstanding the real and complex challenges that lie ahead in a resource-limited setting, valuable lessons have emerged from the pandemic that are worth celebrating. For example, due to social distancing requirements, PPIE recruitment became virtual, allowing research teams to recruit nationally, potentially resulting in better representation than would otherwise be achieved. Platforms such as OpenSAFELY 5 and COVID-IMPACT were developed and effectively deployed during the pandemic with a lasting legacy for use of confidential data for research. Data collections were rapidly set up at scale and some already are, 13 or will shortly be, 14 made available to bona fide researchers, so that the wider academic community can interrogate these valuable resources. In addition to prompt data access, the usual challenges related to data sharing and collaborations were set aside during the pandemic. Initiatives like the National Long COVID working group and the Long COVID qualitative network encouraged members to meet regularly to share study findings. Additionally, for example, instead of competing for funding, 20 people nationally came together to form the CLoCk consortium. Also clear is that seemly disparate research on different aspects of the pandemic are, in fact, inter-related! Clinicians, researchers and people with lived experience all struggled with similar concepts and thoughts: for example, on how to define, triage and treat Long COVID, although these thoughts are articulated differently. Given the multiple bodily systems Long COVID appears to affect, it is clearly best to not work in silos. Crucially, capacity and expertise have been built in pandemic preparedness for immediate and long-term action in both leadership and research positions. It is imperative that this capacity is sustained and continues to grow. For example, enhancing capacity within initiatives such as Biomedical Research Centres through directing themed research calls or offering specific fellowships focused on pandemic preparedness. This could foster ongoing research and develop individuals and teams to be equipped, as far as possible, to tackle future pandemics and the ensuing aftermath with greater efficacy.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768241262661 - Supplemental material for Long COVID: what do we know now and what are the challenges ahead?
Supplemental material, sj-pdf-1-jrs-10.1177_01410768241262661 for Long COVID: what do we know now and what are the challenges ahead? by Snehal M Pinto Pereira, Fiona Newlands, Jake Anders, Amitava Banerjee, Sarah Beale, Ann Blandford, Kate Brown, Feifei Bu, Wing Lam Erica Fong, Gina Gilpin, Pia Hardelid, Jana Kovar, Jason Lim, Chloe Park, Vishnuga Raveendran, Anoop D Shah, Xin Shao, Andrew Wong, Terence Stephenson and Roz Shafran in Journal of the Royal Society of Medicine
Footnotes
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.