
Abstract
Objectives
Risk of death after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has fallen during the pandemic, largely due to immunity from vaccination. In England, the timing and extent of this reduction varied due to staggered eligibility during the primary vaccination campaign, based on age and clinical risk group. Duration of protection is less well understood. Our objective was to estimate the case fatality risk (CFR) by vaccination status and time since last dose during a period of widespread community testing, to better understand the impact of coronavirus disease 2019 (COVID-19) vaccination and duration of protection.
Design
SARS-CoV-2 cases diagnosed between May 2020 and February 2022 were linked to vaccine records from the National Immunisation Management System. CFR was calculated as the proportion of cases that died of COVID-19 per the death certificate, aggregated by week of specimen and stratified by 10-year age band and vaccination status.
Setting
England, UK.
Participants
A total of 10,616,148 SARS-CoV-2 cases, aged ≥18 years, recorded by England’s laboratory reporting system.
Main outcome measures
Case fatality risk of COVID-19, stratified by age band and vaccination status.
Results
Overall, a reduction in CFR was observed for all age bands, with a clear temporal link to when the age group became eligible for primary vaccination and then the first booster. CFR increased with age (0.3% 50–59 years; 1.2% 60–69; 4.7% 70–79; 16.3% 80+) and was highest in the unvaccinated – albeit a reduction was observed over time. The highest CFR was seen in the unvaccinated 80+ group prior to vaccination rollout (30.6%). CFR was consistently lowest in vaccinated populations within 6 months of last dose, yet increased after over 6 months elapsed since last dose, across all age bands.
Conclusions
COVID-19 CFR reduced after vaccination, with the lowest CFR seen across all age bands when vaccinated up to 6 months prior to specimen date. This provides some evidence for continued booster doses in older age groups.
Keywords
Introduction
After the successful rollout of the coronavirus disease 2019 (COVID-19) vaccination programme in England, COVID-19-associated hospitalisations and deaths reduced significantly. The vaccine has been credited with directly averting an estimated 261,500 hospitalisations and 127,500 deaths in England alone. 1 While clinical trials and real-world vaccine effectiveness studies have clearly demonstrated the vaccine’s ability to significantly reduce COVID-19 disease severity,1,2 it remains useful to use ecological analyses to visualise the overall impact of vaccines on COVID-19 mortality in the population.
England staggered the rollout of vaccines through the population by priority groups based on highest risk of severe outcomes, as defined by the Joint Committee on Vaccination and Immunisation (JCVI). This allows us to observe changes in COVID-19 mortality through different risk groups over time.3,4 On 8 December 2020, the COVID-19 vaccine was first offered to care home residents and staff, people aged over 80 years and frontline healthcare staff (Supplementary Appendix Table 3).5–8 The vaccine was then offered to younger age groups and those in clinical risk groups in stages, up to mid-June 2021 when all people aged over 18 years were eligible. Booster vaccines were initially offered to people aged over 50 years and clinically vulnerable groups from September 2021, then subsequently offered to the whole population, again staggering the roll out through the priority groups.
Case fatality risk (CFR) has been a useful metric for observing changes in mortality during the pandemic. 9 When testing patterns are stable, this measure can show changes in risk of death over time, highlighting groups at higher risk of severe disease or death. In England, for COVID-19, CFR is the percentage of people who died after a positive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) test, tested by polymerase chain reaction (PCR) 10 or lateral flow device (LFD), 11 out of the total number of individuals who have tested positive, within the same time frame. The UK Health Security Agency (UKHSA) routinely published CFR estimates during the pandemic, 12 tracking CFR changes over time. While CFR cannot directly show causality, it can contextualise temporal trends in deaths when paired with information such as timings of vaccine rollout, infection trends and testing changes. Here, we report CFR in England among adults, stratified by age and vaccination status, to better understand the impact and timeliness of vaccination against COVID-19.
Methods
To examine how CFR changed throughout the COVID-19 pandemic in England and assess variations in CFR by age, we calculated CFR within 10-year age bands, considering vaccination status and time elapsed since last dose.
Data sources
In England, comprehensive, national-level SARS-CoV-2 testing data are collected in real time to inform disease trends and policy. This includes Pillar 1 data, comprising tests conducted within National Health Service (NHS) and public health laboratories for patients and healthcare workers, and Pillar 2 data, which include tests performed through community PCR programmes and self-reported LFD tests.
Test results are collated by UKHSA in the Second Generation Surveillance System (SGSS). 13 COVID-19 cases are counted at episode level, measured from an individual’s earliest positive specimen date, with infections counted as separate episodes if there are over 90 days between positive tests. In this analysis, time to death is measured from the first positive specimen date of an individual’s most recent episode. To create a person-level dataset to estimate CFR, only the most recent episode was included where individuals had multiple episodes reported.
Information on deaths was obtained from UKHSA’s COVID-19 deaths dataset. 14 Four reporting sources contribute to this dataset: (1) COVID-19 deaths in hospitals, collected through the COVID-19 Patient Notification System; (2) deaths notified to local Health Protection Teams during outbreak management; (3) death reports from NHS electronic records linked to positive SARS-CoV-2 test records; and (4) death registrations from the Office for National Statistics (ONS).
Both cases and deaths data contain information on individual’s age, sex, ethnicity, place of residence (including whether resident in a care home) and residential index of multiple deprivation (IMD). Death records were linked to COVID-19 case data using unique identifiers: NHS numbers and SGSS-derived identifiers. Only deaths linked to positive COVID-19 tests were included in the analysis.
Vaccination status data were obtained through the National Immunisation Management System (NIMS). 15 NIMS was developed to collect national COVID-19 vaccination programme data, acting as a national vaccine register and collating information on administered vaccinations. The latter is used to monitor vaccination rollout and assess vaccine coverage and effectiveness. COVID-19 case data were linked to NIMS records using NHS numbers to obtain vaccination status at the time of individual’s positive tests.
Data analysis
Definition of the CFR
For this analysis, a COVID-19 case was counted in the CFR denominator if the positive specimen date was between 28 May 2020 and 28 February 2022. As CFR is sensitive to testing pattern changes, this time period was selected as it captures when universal access to testing for symptomatic and asymptomatic individuals was available through community testing programmes. 16 It excludes the first months of the pandemic, when testing was limited to symptomatic hospital patients and healthcare workers. 17 The analysis was further limited to individuals aged 18 or over at time of their positive test, and those who had a valid NHS number recorded.
A death was counted in the CFR numerator if COVID-19 was mentioned as a cause of death on the death certificate (ICD-10 codes U07.1: laboratory-confirmed COVID-19, U07.2: probable COVID-19, U09.9: post-acute COVID-19), and the individual had died within 28 days of a positive SARS-CoV-2 test.
Vaccination status
Individuals were assigned one of the following vaccination statuses at the time of their positive test: Unvaccinated, Vaccinated (up to 6 months since last dose), Vaccinated (over 6 months since last dose) or Unknown.
Unvaccinated status was assigned when an individual was linked to a NIMS record but no vaccine doses were recorded, or the individual had an incomplete primary vaccination course (only one dose, or where fewer than 15 days had elapsed between second dose and positive test [14 days post-vaccination has been established as the onset of protection beginning]). 18 Individuals were also classified Unvaccinated if vaccination dates were invalid (i.e. before 1 May 2020, when COVID-19 vaccine trials initiated). 19 All cases with specimen dates prior to 8 December 2020 (when vaccine rollout began), not otherwise recorded as Vaccinated in NIMS (most likely individuals in vaccine trials), were coded as Unvaccinated. 6
Individuals were categorised as Vaccinated when they received at least two vaccination doses, and their positive specimen date was over 14 days after their second dose. Vaccinated individuals were further grouped by time since last vaccination:
Up to 6 months since last dose, if their most recent dose was between 15–182 days prior to their specimen date; Over 6 months since last dose, if their most recent dose was over 182 days prior to their specimen date.
Unknown status was assigned if an individual’s positive test could not be linked to a NIMS record or vaccination dates were erroneous, such as the second dose preceding the first.
Analytical methods
CFR was calculated by week of positive specimen date, as the percentage of total cases that week who died, presented as a monthly rolling average. CFR is not presented in weeks with fewer than 10 cases in any given age and vaccination group.
CFR was calculated for the total study population and stratified by vaccination status and age. Age-specific analyses were limited to adults aged over 50 years (grouped as 50–59 years, 60–69, 70–79 and 80+). Small numbers of COVID-19 deaths among those under 50 prevented more detailed analysis.
Sensitivity analyses
The impact of additional demographic factors on CFR was investigated, focusing on potential confounders that could lead to over- or under-estimation of the impact of vaccination status on CFR. Factors where large variations in mortality rate have been observed throughout the pandemic were explored, including residential IMD, region and ethnicity. 12 Additionally, to assess whether overall trends in CFR by vaccination status remain despite varied severity of disease, a sensitivity analysis was performed by stratifying CFR by testing Pillar. Tests via Pillar 1 broadly represent individuals with more severe illness as they were mainly administered in hospital settings, whereas tests via Pillar 2 broadly represent less severe cases, tested in community settings. 20
Data linkage was carried out using Stata 17.0 and Microsoft SQL Server Management Studio 18. Analyses were conducted using Stata 17.0.
Results
A total of 15,900,905 COVID-19 cases were captured in SGSS with specimen dates between 28 May 2020 and 28 February 2022. Of these, 1,424,072 (9.0%) were excluded due to missing NHS numbers, 3684 (0.02%) due to missing age and 3,351,480 (21.1%) as they were aged under 18 years. Only the most recent infection was used if more than one was recorded, achieving a person-level dataset, excluding 505,521 cases (3.2% of cases over this period). In total, 10,616,148 COVID-19 cases were included in the analysis.
Within 10,616,148 included COVID-19 cases, 90,542 individuals died with COVID-19 on their death certificate and within 28 days of a positive test, giving overall CFR of 0.85%. Among all adults, CFR was highest in those unvaccinated (1.65%), compared with those who had been vaccinated within 6 months prior to their positive test (0.23%) (Table 1).
CFR of COVID-19 cases between 28 May 2020 and 28 February 2022, aged 18 years and over, by vaccination status or age band.
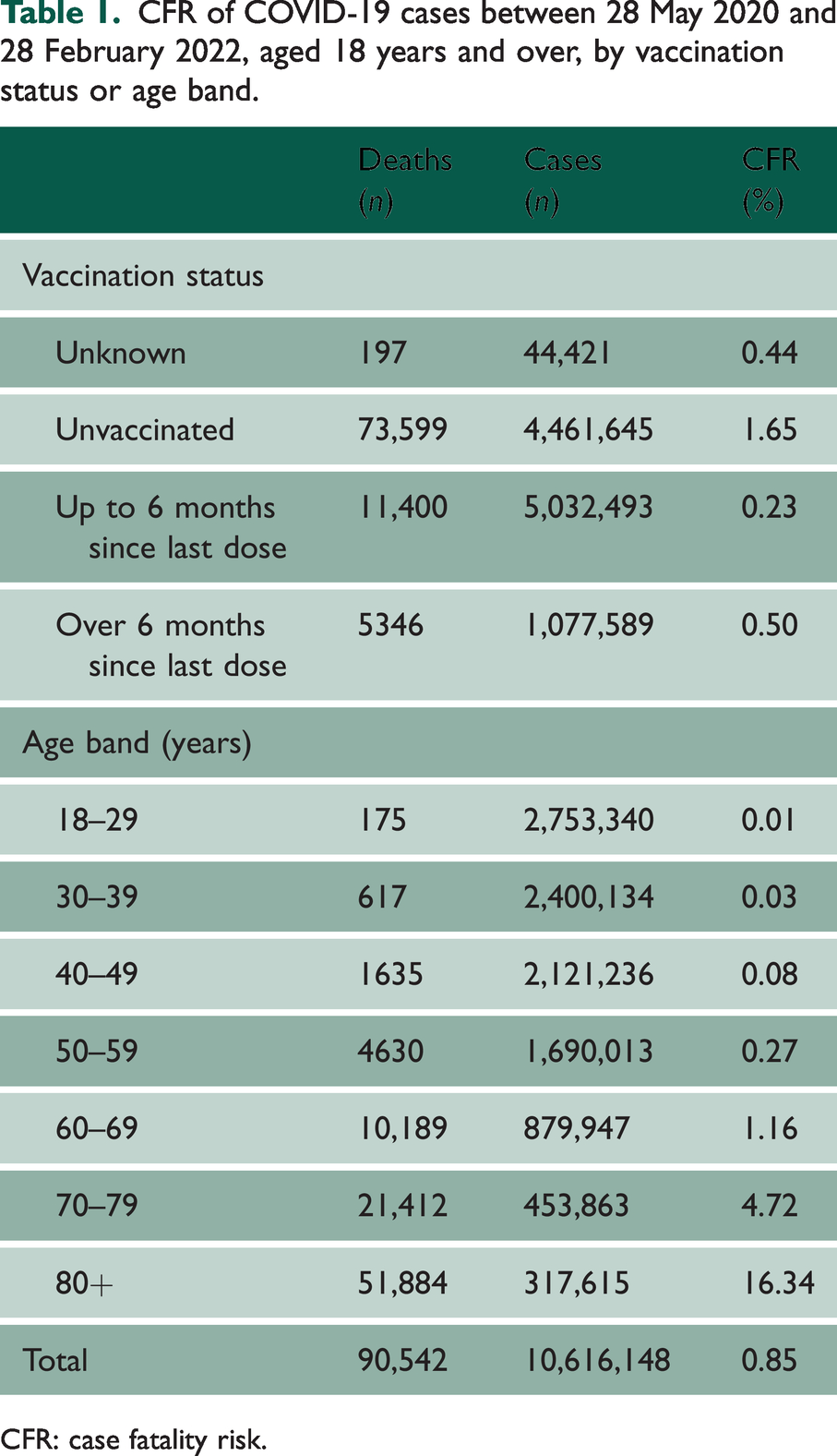
CFR: case fatality risk.
The age band with the lowest CFR was 18–29-year-olds (0.01%), increasing with age to the highest CFR observed in those aged over 80 years (16.3%). CFR was consistently higher among older age bands throughout the study period (Figure 1(d)).
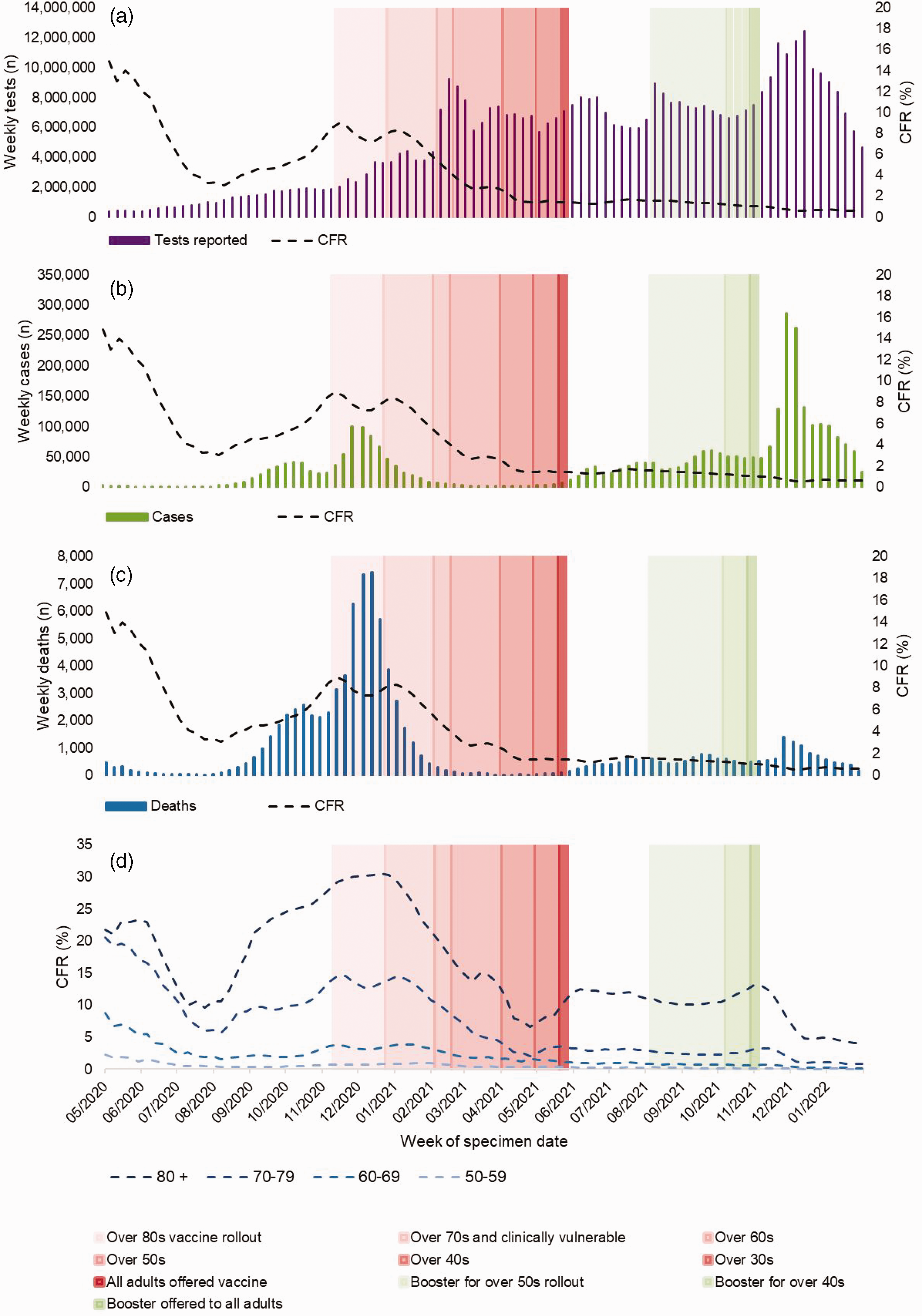
COVID-19 tests reported (all ages; positive, negative and void) (a), cases (all ages) (b), deaths (all ages) (c) and case fatality rate (CFR) (d) between 28 May 2020 and 28 February 2022, in those aged over 50 years, by age band and week of specimen.
Among those aged over 50 years, CFR was highest at the start of the study in May 2020 (14.9%) (Figure 1). This was followed by a decline from June to August 2020 when CFR dropped to 2.4%, coinciding with the end of the first wave of SARS-CoV-2 infections, an increase in tests performed and a decrease in test positivity. CFR increased again towards the end of 2020 during the Alpha variant wave, to a maximum of 9.6% in December 2020. A steep decline in CFR was observed in early 2021, coinciding with the start of the COVID-19 vaccine rollout. By May 2021, CFR plateaued between 0% and 2%.
Among those aged over 50 years, overall CFR was 10 times higher in those who were unvaccinated (6.3%) compared with those vaccinated in the 6 months prior to their positive test (0.6%). The highest CFR observed during the study period was among unvaccinated cases aged over 80 years, in the week commencing 15 January 2021 (30.6%) (Figure 2(d)). The lowest CFR was observed among vaccinated 50–59-year-olds from May 2021 onwards (0.02%), after the primary vaccine course rollout in this age band.
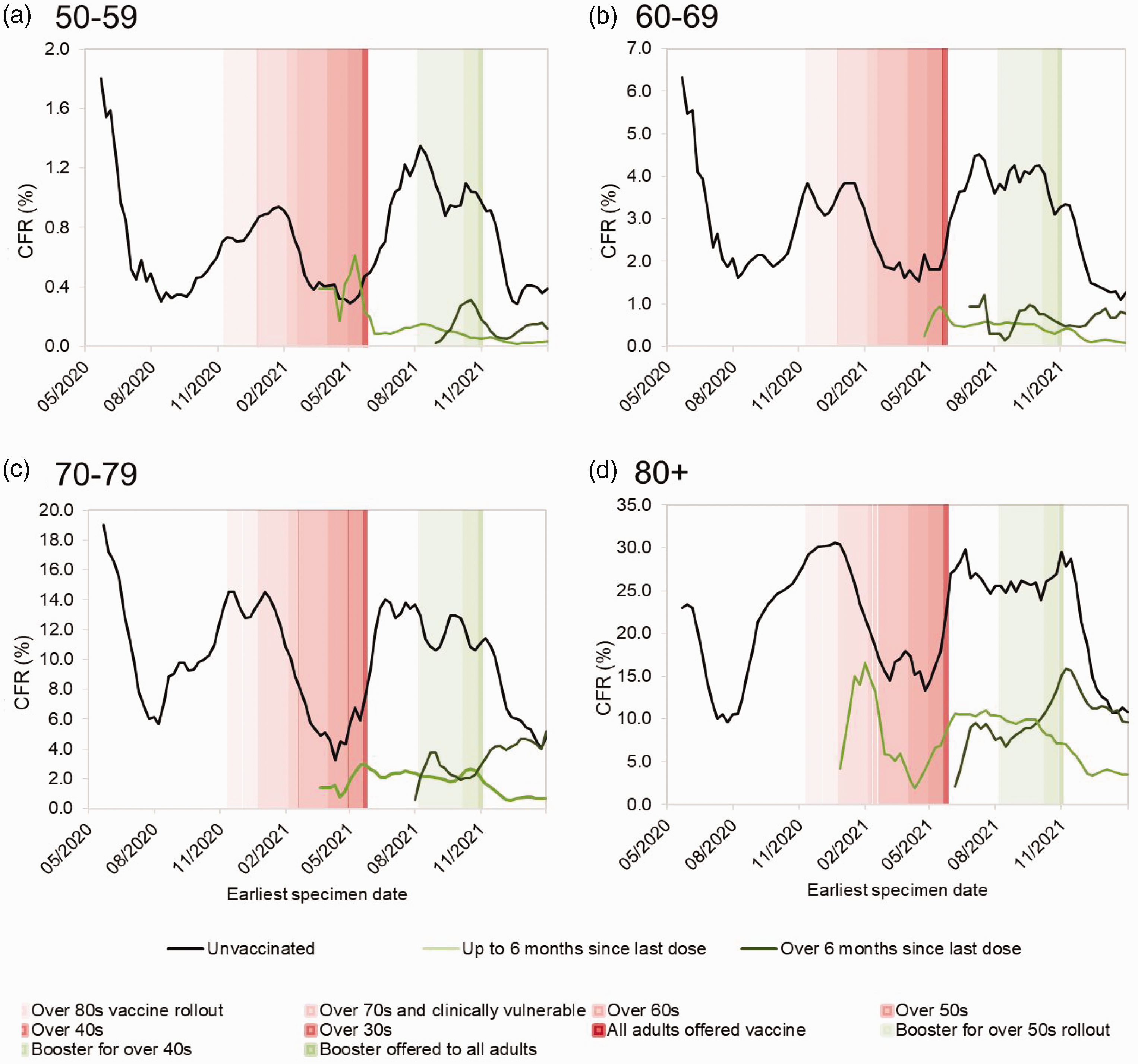
Case fatality rate (CFR) of COVID-19 cases between 28 May 2020 and 28 February 2022, by vaccination status and week of positive specimen in those aged 50–59 years (a), 60–69 (b), 70–79 (c) and 80+ years (d).
Although low, a slight decline in CFR was observed after the COVID-19 booster dose rollout in late 2021, notably among those aged over 70 years. However, at the same time, CFR declined in all groups, including a steep decline in unvaccinated populations. At this point, the Omicron variant had emerged and both SARS-CoV-2 tests and COVID-19 case numbers (Figure 1) were at their highest point of the pandemic, resulting in widespread immunity.
Towards the end of the study period, an increase in CFR can be seen among those whose most recent vaccine dose was over 6 months prior to their positive test. In the oldest age bands (70–79 and over 80 years), CFR approaches that of their unvaccinated same-age peers.
Further analysis of CFR stratified by sex, residential IMD and ethnic group is presented in Supplementary Appendix Table 4. The highest overall CFR when stratified by ethnic group was observed among those of unknown ethnic group (7.13%), followed by those of Asian/Asian British and Black/Black British ethnicity (2.79% and 2.73%, respectively). CFR was highest among those living in the most deprived IMD quintile (3.49%) and was higher among men (3.05%) compared with women (2.27%). These analyses all show similar CFR trends by vaccination status, with higher CFR seen in unvaccinated groups compared with vaccinated.
Sensitivity analysis
A sensitivity analysis stratifying CFR by testing Pillar (Pillar 1 representing tests within healthcare settings; Pillar 2 community-based testing) shows the same patterns in CFR by vaccination status and age band as the overall CFR, yet with higher CFR seen in Pillar 1 cases. In both testing Pillars, CFR is considerably higher in unvaccinated groups (21.1% under Pillar 1; 2.2% under Pillar 2) and lowest in those vaccinated within 6 months prior to their positive test (4.9% under Pillar 1; 0.23% under Pillar 2).
Discussion
In this analysis, COVID-19 CFR in England is presented during a period of widely available SARS-CoV-2 testing, stratified by vaccination status and age band. Overall, CFR was found to be highest in older individuals and those who were unvaccinated. The results also show that demographic factors, particularly sex, geographical region of residence, residential IMD and ethnicity also play a role in determining CFR. During the study period, CFR fluctuated considerably over time among all groups. This could be attributed to several factors, including changes to virulence, with emerging genomic variants of SARS-CoV-2 circulating in the population at different times, and the demographics of the population susceptible to infection shifting as vaccine-derived and natural immunity from increased exposure became more likely. Artefactual factors, such as testing availability and coverage, and changes in clinical management, may also impact both numerator and denominator when calculating CFR.
Following onset of the COVID-19 vaccination programme in England, in December 2020, there was a marked reduction in overall CFR and among all age bands over 50 years, with CFR then remaining low until the end of the study. This trend was not mirrored when observing the unvaccinated population independently where, from mid-2021 to the start of 2022, the CFR for all age bands increased to levels close to those observed at the outset of the study period, prior to the vaccination rollout. It is important to note that as the vaccine programme was delivered, individuals who remained unvaccinated represent a small and potentially distinct proportion of the overall population. Nevertheless, high CFR was maintained in this group amid changing transmission rates and severity associated with different SARS-CoV-2 variants, and despite widespread infection-acquired immunity. These results indicate that vaccination is indeed a key factor in reducing mortality associated with COVID-19.
Our results also suggest that, despite the evident reduction in CFR after SARS-CoV-2 vaccination, the benefit in reducing disease-associated mortality is not indefinite. Towards the end of the study period, an increase in CFR was observed for individuals vaccinated over 6 months prior to their specimen date, across all age bands, with CFR reaching levels closer to that of unvaccinated groups. This suggests that the protective benefit of the vaccine against mortality wanes after around 6 months post-vaccination, a conclusion supported by other research.21–23 ONS’s findings show that all-cause mortality was lower in vaccinated individuals and specifically, from September 2021, monthly age-standardised mortality rates were lower for all months until December 2022 (end of their study period) after the initiation of the booster programme among people who had received a booster dose at least 21 days prior.8,24 Both these studies’ results support the continuation of the vaccination booster programme, focusing on those at highest risk of death and severe outcomes of COVID-19, to maintain a low CFR. The risk is highest to those in older age groups, and so continued boosters should also be focused on these groups, where resources may be limited.
CFR has been a useful metric for observing changes in mortality; however, robust CFR measures rely on the assumption that all individuals with or without the infection have equal likelihood of being tested during the study period, which is not the case for most respiratory infections. CFR is highly sensitive to changes in testing patterns. We observed fluctuations in case numbers, along with changes to testing coverage and availability over the study period, resulting in varying CFR. We chose a study period when community testing was widely available and weekly numbers of tests performed were relatively consistent, particularly from early 2021 (Figure 1(a)). However, even during this time, England’s COVID-19 testing policy and programme underwent many changes; for example, in April 2021, LFD tests became available to all, resulting in a large increase in numbers of tests performed and a decrease in CFR.20,25 After this date, with many individuals routinely testing without signs of illness, it becomes more likely that asymptomatic positive infections would be captured in case data. Furthermore, certain populations may have been more or less likely to seek testing during this time period; for example, contingent upon whether they would be entitled to sick pay, these inequalities would be masked in a descriptive analysis of CFR that does not adjust for confounding factors, which may result in over- or under-estimation of CFR. 26
The highest CFR across all groups was seen in the period prior to vaccination rollout when population-level natural immunity was low, with some non-pharmaceutical interventions in place to reduce the spread of COVID-19 in the population. Although (PCR) testing was universally available at this point, it was only offered to symptomatic individuals. The second peak in overall CFR was seen when death counts were highest during the Alpha variant wave, 27 and coincided with when vaccines were offered to those aged over 70 years or at high risk of severe disease. The highest CFR across all age bands was observed in those aged over 80 years (30.6% in January 2021). This occurred when testing was primarily available within healthcare settings (PCR, under Pillar 1) 27 ; therefore, it is probable that individuals tested were more likely to be at higher risk of severe disease and death. Additionally, this peak in CFR was observed over Winter, when all-cause risk of death is higher than during other seasons. 28 Nevertheless, clear trends of reduced CFR over time, across all age bands, were observed after the introduction of both the initial vaccination and booster programmes.
This study has several strengths, in particular the use of comprehensive, national-level, testing data that can be linked to death records, including cause of death information and robust vaccination information. However, there are some limitations, including that vaccination records may not be entirely complete. Individuals may have had vaccine doses abroad, resulting in an incomplete NIMS record, thus being potentially included in the unvaccinated group when they have in fact completed their course, which could result in underestimating CFR. Furthermore, 9% of cases were excluded as they had no NHS number, as this is required for data linkage. It is possible there are inherent differences between individuals with and without NHS numbers, such as those not registered with a GP for specific reasons, who were still eligible for vaccination in England. 29 These individuals, such as asylum seekers or rough sleepers, 30 may be at higher risk of adverse outcomes from COVID-19.
Additionally, there may have been individuals undertaking self-testing who did not self-report their result. Sensitivity analyses assessed this potential bias, showing that under Pillar 1, where testing was undertaken primarily within healthcare settings and routinely reported, trends of CFR by vaccination status were the same as those undertaken via community testing and self-testing. This trend showed the highest CFR among the unvaccinated, followed by those who were vaccinated over 6 months prior to their specimen date (Table 2). Further analyses (Supplementary Appendix Table 4) also show that this study is robust to changes in assumptions that the population is demographically homogenous (specifically sex, residential IMD and ethnic group), as similar trends are observed in each sub-group, including highest CFR seen in unvaccinated individuals.
Cases, deaths and CFR (%) of COVID-19 cases aged over 50 years, between 28 May 2020 and 28 February 2022, by time since last vaccination dose and testing Pillar.
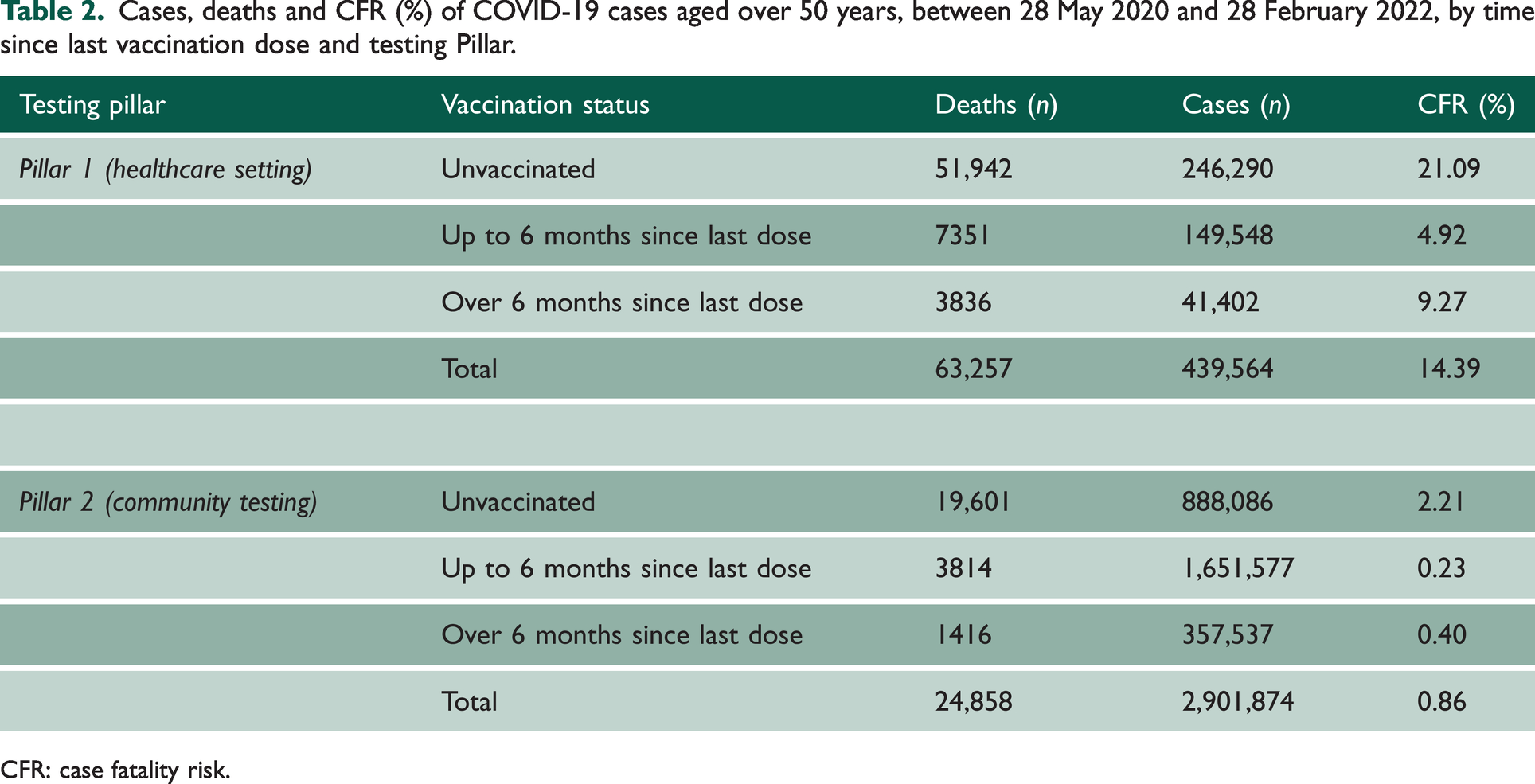
CFR: case fatality risk.
There are likely several clinical risk factors that were not included in the data used for this study, which may also contribute to the differences in CFR observed. By not adjusting for these factors, there are limitations to our understanding of the mechanisms for why CFR varies by vaccination status and among specific risk groups, particularly for those at high risk of severe disease (individuals in the first cohort offered the vaccine). Further studies stratifying by underlying clinical risk factors are advised to further understand these differences and inform on the populations for which continued booster vaccination are most beneficial.
In our study design, to assess CFR at person- rather than infection-level, we prioritised individual’s most recent SARS-CoV-2 infection if they had multiple infections. This could result in the impact of COVID-19 and its severity not being fully captured, with CFR being biased towards the outcomes of those with reinfections, as well as overestimation of CFR compared with calculating this metric at infection-level. However, the impact of this on findings is likely small, as 3.2% of cases in this period were reinfections. Further studies should consider a design that includes all infections, stratified by infection number, to assess the impact of repeat infections on CFR.
CFR calculations can be skewed by trends in cases and deaths. In Spring 2021, in the 50–59-year age band, CFR was highest in those recently vaccinated (0.62% vs. 0.32% in the unvaccinated group) (Figure 2(a)). At this point in the study, case and death numbers were very low, potentially biasing the CFR. In addition, those at higher risk of severe disease, therefore death, were invited to vaccinate before the rest of their age band, which may have inflated the CFR at this time.
Investigations into vaccine effect waning, beyond observing a 6-month cut-off, were not possible in this study as the population with sufficient time between their last vaccination dose and COVID-19 infection, stratified by age, was too small. This was in part due to regular booster dose availability in the latter part of the study, resulting in few individuals with extended dose intervals. Therefore, 6 months since last dose was the longest feasible period to present CFR within. Further analysis, including a longer period after vaccination, is needed to fully investigate the extent of this.
This investigation into the varied CFR between May 2020 and February 2022 highlights the importance of looking at CFR by vaccination status, rather than focusing on overall trends. Despite limitations, this study demonstrates that the national vaccination programme had a notable impact on reducing COVID-19-related mortality, particularly in older age bands, and that continued booster programmes are required in maintaining low COVID-19 CFR. Further investigations into the appropriate cut-off age for the booster doses is required, yet we have shown that CFR risk increases with increasing age and with increasing time since last dose. Sensitivity analyses gave evidence to support this claim and thus, future research could also focus on exploring how best to increase vaccination uptake within the unvaccinated population in England, to reduce the prevalence of adverse outcomes associated with COVID-19 infection.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768231216332 - Supplemental material for Temporal changes to adult case fatality risk of COVID-19 after vaccination in England between May 2020 and February 2022: a national surveillance study
Supplemental material, sj-pdf-1-jrs-10.1177_01410768231216332 for Temporal changes to adult case fatality risk of COVID-19 after vaccination in England between May 2020 and February 2022: a national surveillance study by Florence Halford, Kathryn Yates, Tom Clare, Jamie Lopez-Bernal, Meaghan Kall and Hester Allen in Journal of the Royal Society of Medicine
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.